
18 February 2015 - Case #343
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mouna Khmou, University Hospital CHU IBN SINA, Children's Hospital (Morocco), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case #343
Clinical history:
A 35 year old woman with no prior medical history consulted for a painless vulvar nodule, first noted 3 years before, which had enlarged over the last few months. There was no history of pain or bleeding. Local and colposcopic examinations revealed a 2 cm freely mobile nontender nodule in the left labium majus. It was excised under local anesthesia.
Microscopic images:
What is your diagnosis?
Diagnosis: Papillary hidradenoma (hidradenoma papilliferum)
Discussion:
Papillary hidradenoma of the vulva is also known as papillary hidradenoma and is the most common benign vulvar adnexal neoplasm (Arch Pathol Lab Med 2013;137:1237). It typically occurs in the perianal or vulvar regions.
Clinically, it is a small, slow growing, firm, red nodule covered by normal skin, often on the labia majora or interlabial folds. It may ulcerate through the skin and simulate carcinoma. The lesion is thought to arise from mammary type glands in the anogenital region (ectopic mammary tissue). Histologically, it resembles intraductal papilloma of the breast, due to its well differentiated papillary fronds in a complex pattern with some stratification and pleomorphism, with ducts lined by mammary type columnar cells that often display apocrine metaplasia. A distinct myoepithelial layer is usually present underneath the columnar epithelium. Mitoses may be present in both epithelial and myoepithelial cells but this does not predict an aggressive course (Am J Dermatopathol 2006;28:322).
Tumor cells are immunoreactive for AE1/AE3, CK5/6, GCDFP-15, androgen receptor and ER (Adv Anat Pathol 2011;18:1) and negative for S100 and high molecular weight cytokeratin.
The differential diagnosis includes
Mammary type adenocarcinoma of the vulva, which in contrast to papillary hidradenoma presents as a rapidly enlarging mass, shows variable nuclear atypia, architectural abnormalities including irregular glandular and solid architecture and absence of myoepithelial cells.
Simple excision is curative.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mouna Khmou, University Hospital CHU IBN SINA, Children's Hospital (Morocco), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.

- Sternberg's Diagnostic Surgical Pathology (2015) by Stacey Mills, Joel Greenson, Jason Hornick, Teri Longacre and Victor Reuter. Visually stunning and thoroughly up to date, the sixth edition of Sternberg's Diagnostic Surgical Pathology continues to set the standard for differential diagnosis of the surgical specimen. Offering the latest information on all currently known diseases, this classic two-volume reference presents advanced diagnostic techniques from a virtual "who's who" of experts in the field - pathologists who provide authoritative guidance on the diagnostic evaluation of every type of specimen from every anatomic site. No matter what your level of training or experience, keeping Sternberg's near your microscope is the next best thing to a personal consultation with a trusted colleague.
- Sternberg's Diagnostic Surgical Pathology Review (2015) by Pier Luigi Di Patre and Darryl Carter. Based on the sixth edition of Sternberg's Diagnostic Surgical Pathology, this multiple choice question and answer resource covers all aspects of Surgical Pathology and is an ideal review tool for board preparation, recertification exams, or just brushing up. Now significantly revised, it includes more than 1,000 questions and answers that emphasize differential diagnostic aspects of problem solving, accompanied by more than 600 full-color illustrations.
For more information, visit our New Books page.
Website news:
(1) We are making some minor changes in designating those writing or updating topics in our Textbook. We will now be calling them "authors" instead of "reviewers", the previous designation. "Author" is more accurate, particularly when substantial changes are made to the topic. If the topic has minimal changes by the new author, we may also keep the prior author's name on the topic, to give credit where credit is due.
(2) We have just posted a new Mystery Case at the bottom left of the Home page. Can you figure out the diagnosis?
(3) We have added more books to the Top Books page for the second half of 2014 (sold at Amazon.com).
Visit Amazon.com for great shopping deals and support PathologyOutlines.com at the same time with any purchase (if you visit Amazon through a link from our website, Amazon will pay us part of their profits on any items purchased, with no extra cost to you)!
(4) Our Feature page for February is Microscopes / Microscopy Products and highlights our advertiser OPTRONICS. It also contains an original short article, "Ultrastructural Microscopy: Beyond Light and Cells", by Jaleh Mansouri, M.D.
Visit and follow our Blog to see recent updates to the website.
(1) We are making some minor changes in designating those writing or updating topics in our Textbook. We will now be calling them "authors" instead of "reviewers", the previous designation. "Author" is more accurate, particularly when substantial changes are made to the topic. If the topic has minimal changes by the new author, we may also keep the prior author's name on the topic, to give credit where credit is due.
(2) We have just posted a new Mystery Case at the bottom left of the Home page. Can you figure out the diagnosis?
(3) We have added more books to the Top Books page for the second half of 2014 (sold at Amazon.com).
Visit Amazon.com for great shopping deals and support PathologyOutlines.com at the same time with any purchase (if you visit Amazon through a link from our website, Amazon will pay us part of their profits on any items purchased, with no extra cost to you)!
(4) Our Feature page for February is Microscopes / Microscopy Products and highlights our advertiser OPTRONICS. It also contains an original short article, "Ultrastructural Microscopy: Beyond Light and Cells", by Jaleh Mansouri, M.D.
Visit and follow our Blog to see recent updates to the website.
Case #343
Clinical history:
A 35 year old woman with no prior medical history consulted for a painless vulvar nodule, first noted 3 years before, which had enlarged over the last few months. There was no history of pain or bleeding. Local and colposcopic examinations revealed a 2 cm freely mobile nontender nodule in the left labium majus. It was excised under local anesthesia.
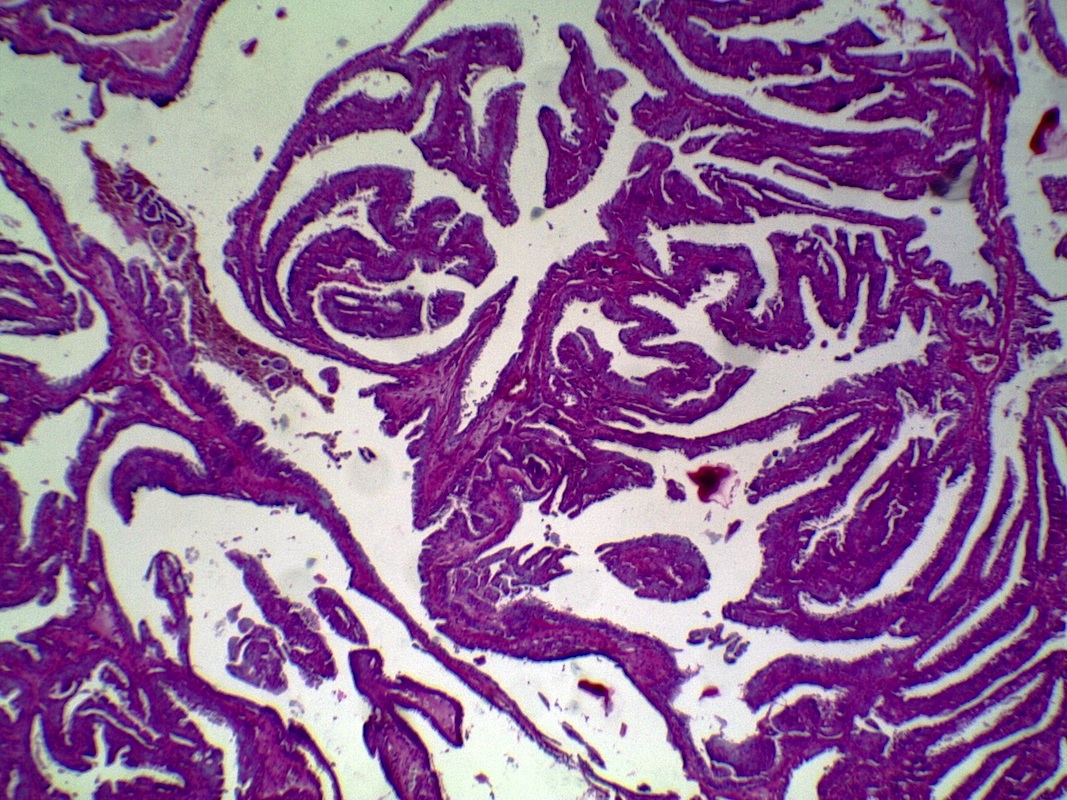
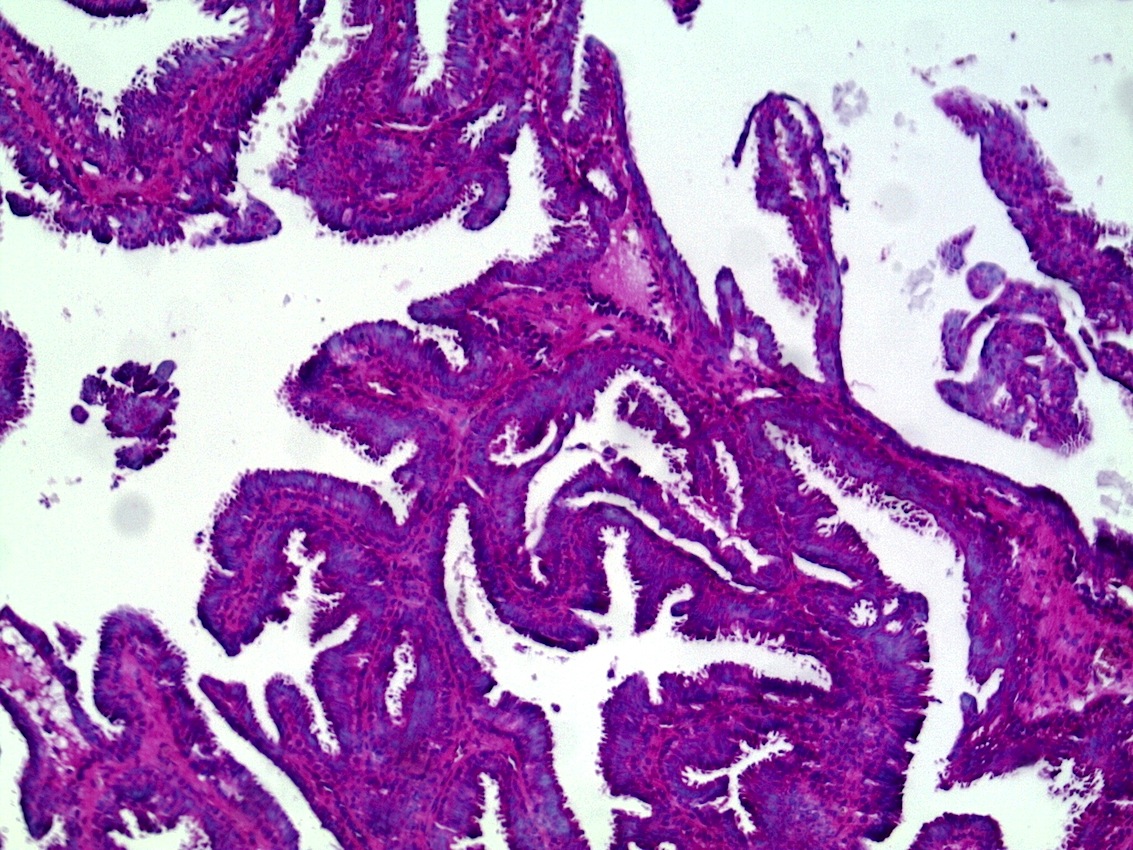
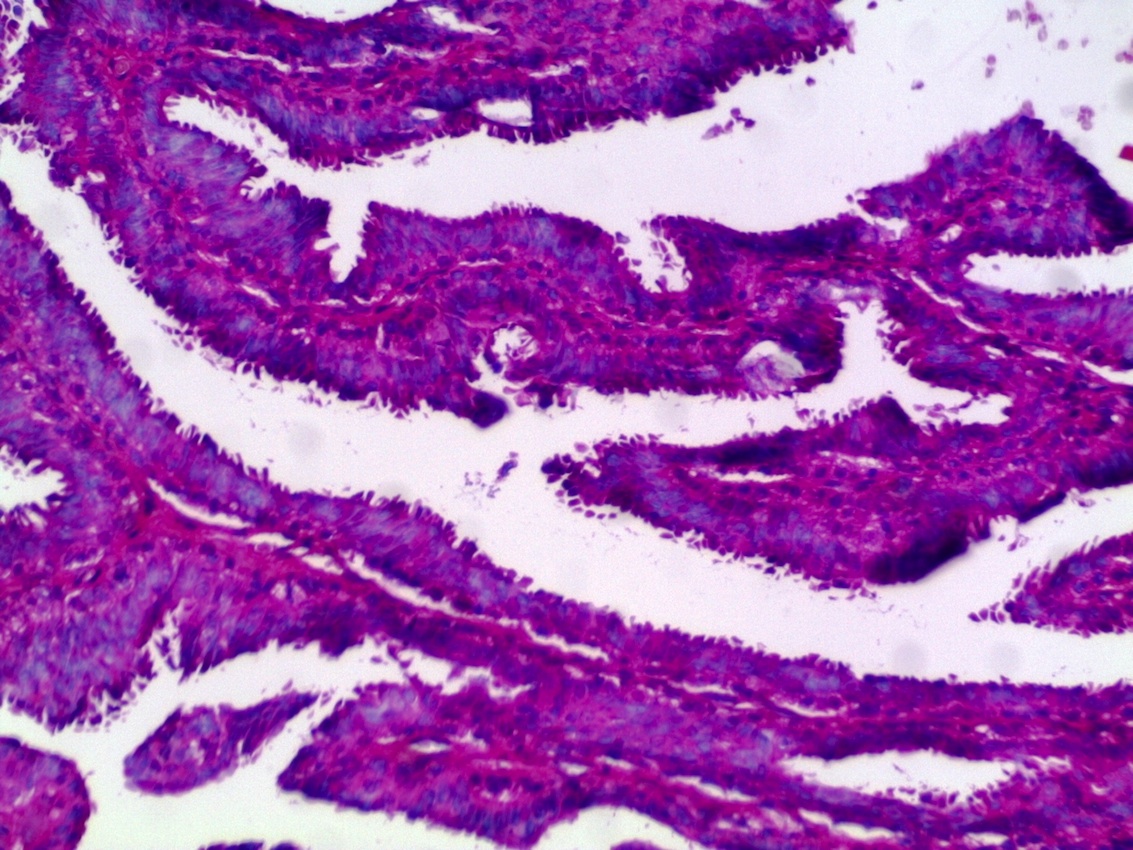
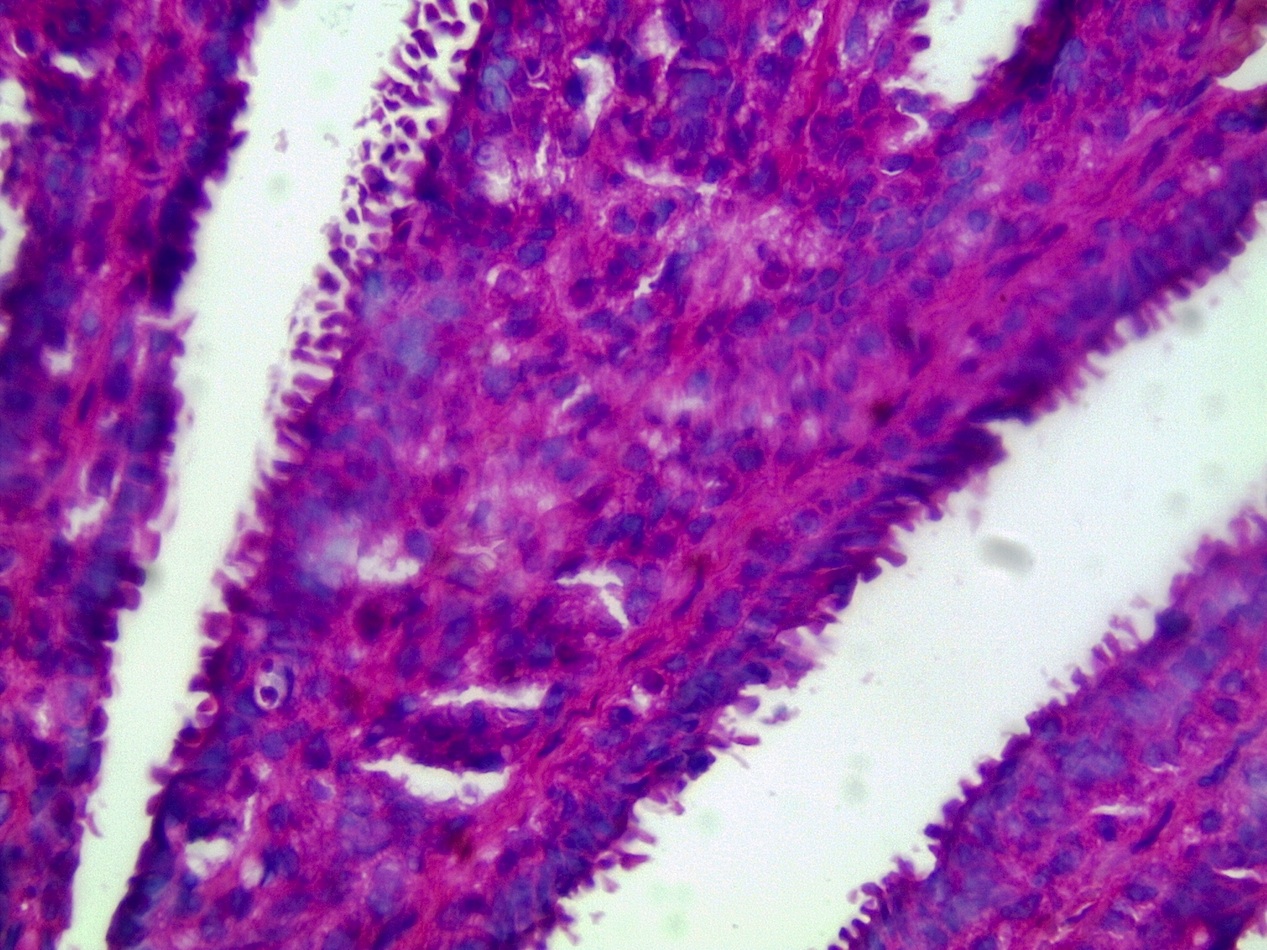
Microscopic images:
H&E images
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Papillary hidradenoma (hidradenoma papilliferum)
Discussion:
Papillary hidradenoma of the vulva is also known as papillary hidradenoma and is the most common benign vulvar adnexal neoplasm (Arch Pathol Lab Med 2013;137:1237). It typically occurs in the perianal or vulvar regions.
Clinically, it is a small, slow growing, firm, red nodule covered by normal skin, often on the labia majora or interlabial folds. It may ulcerate through the skin and simulate carcinoma. The lesion is thought to arise from mammary type glands in the anogenital region (ectopic mammary tissue). Histologically, it resembles intraductal papilloma of the breast, due to its well differentiated papillary fronds in a complex pattern with some stratification and pleomorphism, with ducts lined by mammary type columnar cells that often display apocrine metaplasia. A distinct myoepithelial layer is usually present underneath the columnar epithelium. Mitoses may be present in both epithelial and myoepithelial cells but this does not predict an aggressive course (Am J Dermatopathol 2006;28:322).
Tumor cells are immunoreactive for AE1/AE3, CK5/6, GCDFP-15, androgen receptor and ER (Adv Anat Pathol 2011;18:1) and negative for S100 and high molecular weight cytokeratin.
The differential diagnosis includes
- Apocrine tubular adenoma: well defined nodule, usually 2 cm or less on the scalp, only rarely on the vulva; has lobular pattern of dermal and subcutaneous tubular apocrine structures with epidermal connection, resembling papillary syringadenoma
- Syringocystadenoma papilliferum: warty tumor of the scalp, neck and face that occurs at any age, is associated with nevus sebaceus and basal cell carcinoma; has a glandular papillary pattern with a prominent plasma cell infiltrate.
Mammary type adenocarcinoma of the vulva, which in contrast to papillary hidradenoma presents as a rapidly enlarging mass, shows variable nuclear atypia, architectural abnormalities including irregular glandular and solid architecture and absence of myoepithelial cells.
Simple excision is curative.
