
7 August 2014 - Case #321
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mauro Garcia-Montenegro, Hospital Dr. Guillermo Rawson (Argentina), for contributing this case.

Advertisement
Case #321
Clinical history:
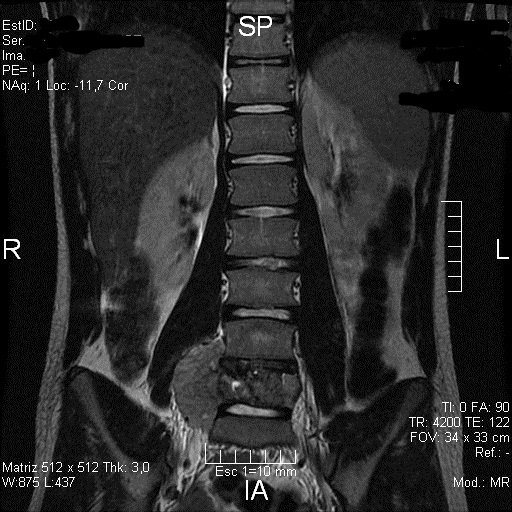
A 14 year old boy had a mass in the L5 vertebral body, with extension to the right paravertebral tissues, which was biopsied.
Radiology images:
Microscopic images:

What is your diagnosis?
Diagnosis: Primary Ewing sarcoma of lumbar vertebrae
Immunostains:


Discussion:
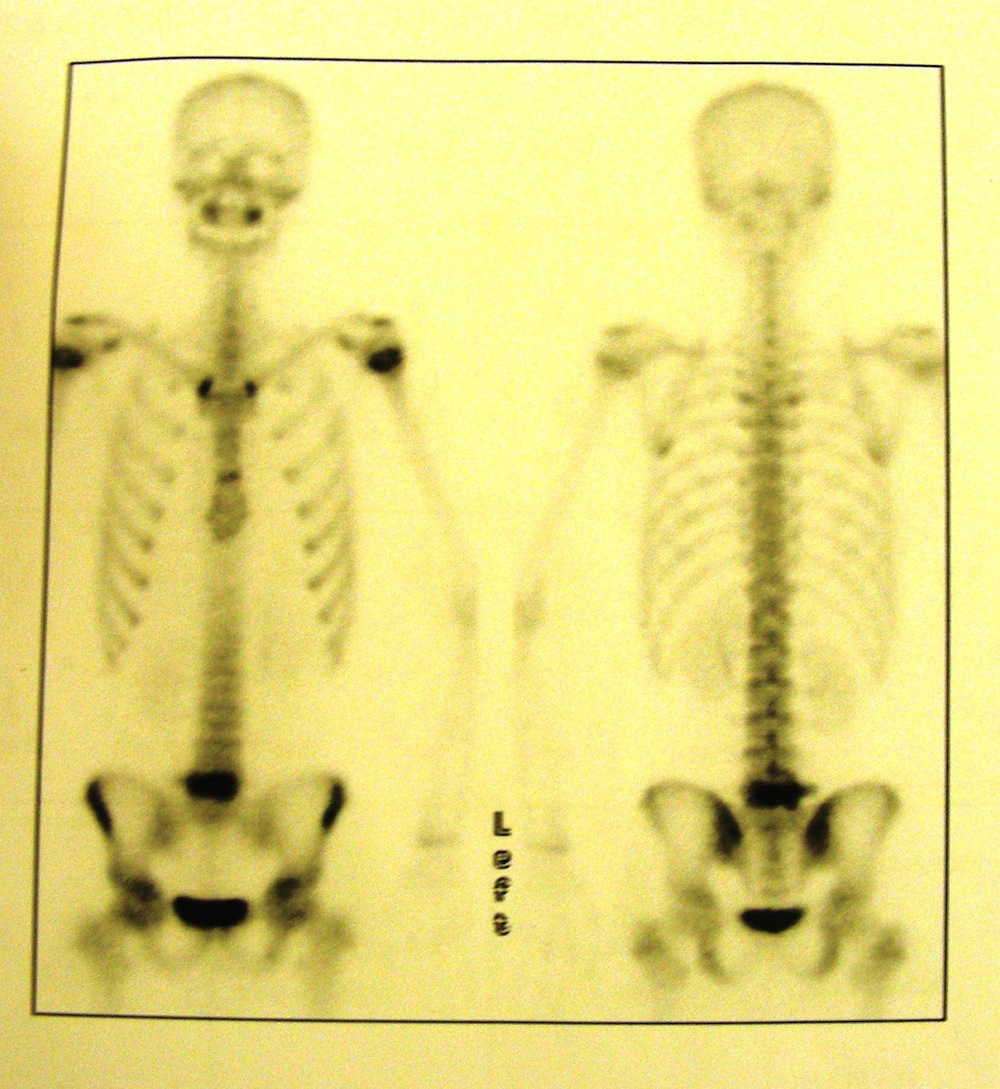
Bone scintigraphy shows a single hyperenhanced image at L5 with normal and symmetric uptake in hematopoietic areas.
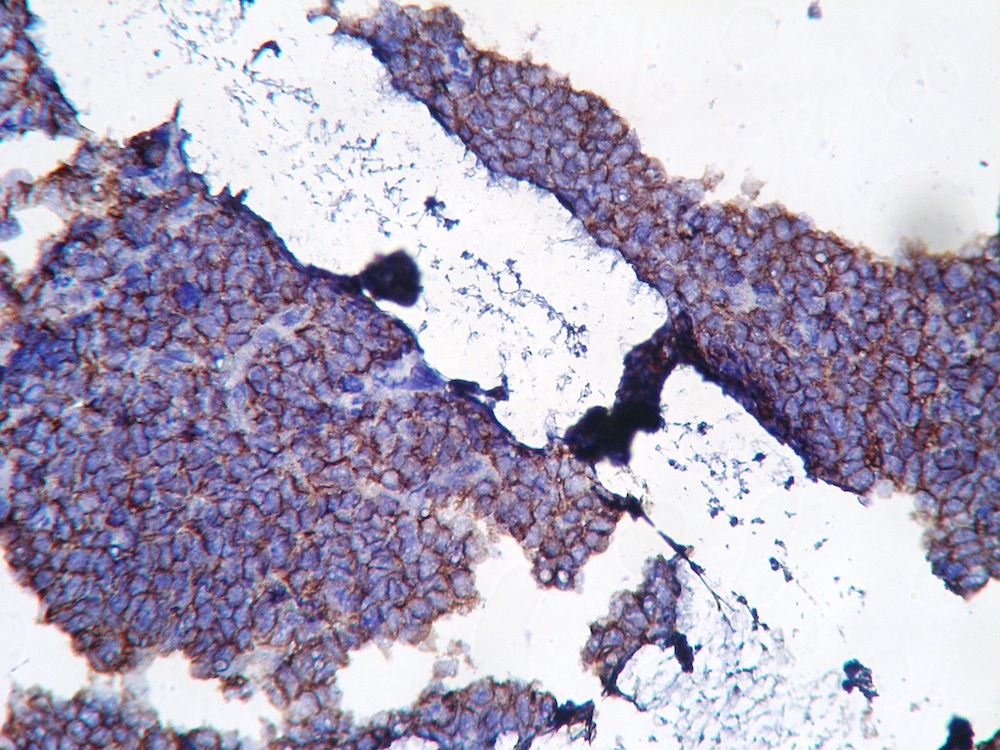
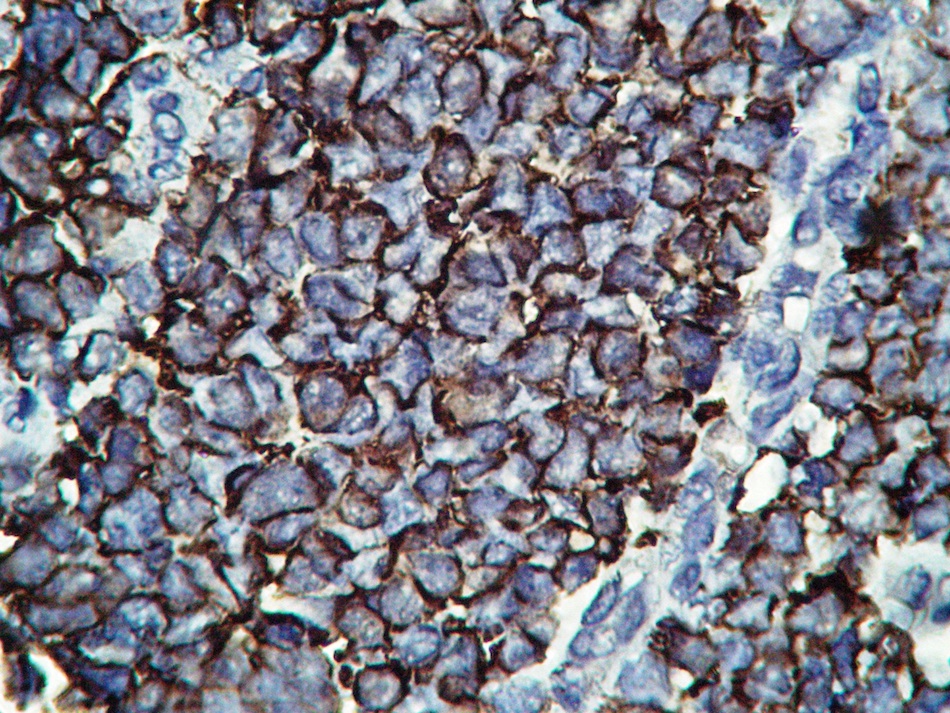
Stains include CD99 (positive and strong in membrane), NSE (positive), PAS (positive in cytoplasmic granules), vimentin (negative) and desmin (negative). MyoD1 shows cytoplasmic staining, due to a cross reaction with an unknown antigen, which has been described in Ewing sarcoma / PNET and neuroblastoma (Dabbs & Thompson: Diagnostic Immunohistochemistry, 4th Edition, 2013).
Fewer than 10% of Ewing tumors arise in the vertebrae. In a study of 33 cases, the median age at diagnosis was 13 years and 64% were male (Med Pediatr Oncol 2001;37:30). 6 patients had metastatic disease and 10 had tumors 8 cm or larger. Primary sites were sacral (13), thoracic (10), lumbar (8) and cervical (2) vertebrae. Pain and neurologic deficits were common.
Histology shows sheets of small, round, uniform cells, 10-15 microns with scant clear cytoplasm, divided into irregular lobules by fibrous strands. The nuclei are round with indentations and small nucleoli. Homer-Wright rosettes (central fibrillary space) or pseudorosettes (cells arrange themselves around vessels) may be present (Bone-Ewing sarcoma / PNET).
The differential diagnosis includes other small blue cell tumors:
Treatment is combination chemotherapy and local radiotherapy, with a 5 year survival of 48 - 70% (Eur J Cancer 2013;49:1314), comparable to this tumor at other sites. Most of the mortality is due to metastatic disease, which occurs in 30% (Case Rep Oncol Med 2012;2012:165289).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mauro Garcia-Montenegro, Hospital Dr. Guillermo Rawson (Argentina), for contributing this case.
Wayne State University
Karmanos Cancer Center
Detroit Medical Center
Presents the 11th Annual Conference
Contemporary Issues in Diagnostic Pathology
Program Director: Rouba Ali-Fehmi, MD

October 18, 2014
The Henry, Autograph Collection
Dearborn, Michigan (USA)
Brochure (link invalid)
Registration (link invalid)
Website
Website news:
(1) We continue to add more surveys to our Surveys and Buyers guide pages. Check out what is new in products and services for Pathologists.
(2) We have now posted the top books sold at Amazon.com through PathologyOutlines.com, click here or on the Top Books link from the Books page. Buy your books through PathologyOutlines.com - we are the only place where you can see all the books that have been recently published!
(3) Our Feature Page for August is Books & Journals, and highlights the publishers ARP Press, ASCP, CAP, LWW and WHO Press. It also contains an original short article, Pathology Books and Journals: A Multidisciplinary Approach, by Jaleh Mansouri, M.D.
Visit and follow our Blog to see recent updates to the website.
(1) We continue to add more surveys to our Surveys and Buyers guide pages. Check out what is new in products and services for Pathologists.
(2) We have now posted the top books sold at Amazon.com through PathologyOutlines.com, click here or on the Top Books link from the Books page. Buy your books through PathologyOutlines.com - we are the only place where you can see all the books that have been recently published!
(3) Our Feature Page for August is Books & Journals, and highlights the publishers ARP Press, ASCP, CAP, LWW and WHO Press. It also contains an original short article, Pathology Books and Journals: A Multidisciplinary Approach, by Jaleh Mansouri, M.D.
Visit and follow our Blog to see recent updates to the website.
Case #321
Clinical history:
A 14 year old boy had a mass in the L5 vertebral body, with extension to the right paravertebral tissues, which was biopsied.
Radiology images:
Bone scintigraphy
MRI
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Primary Ewing sarcoma of lumbar vertebrae
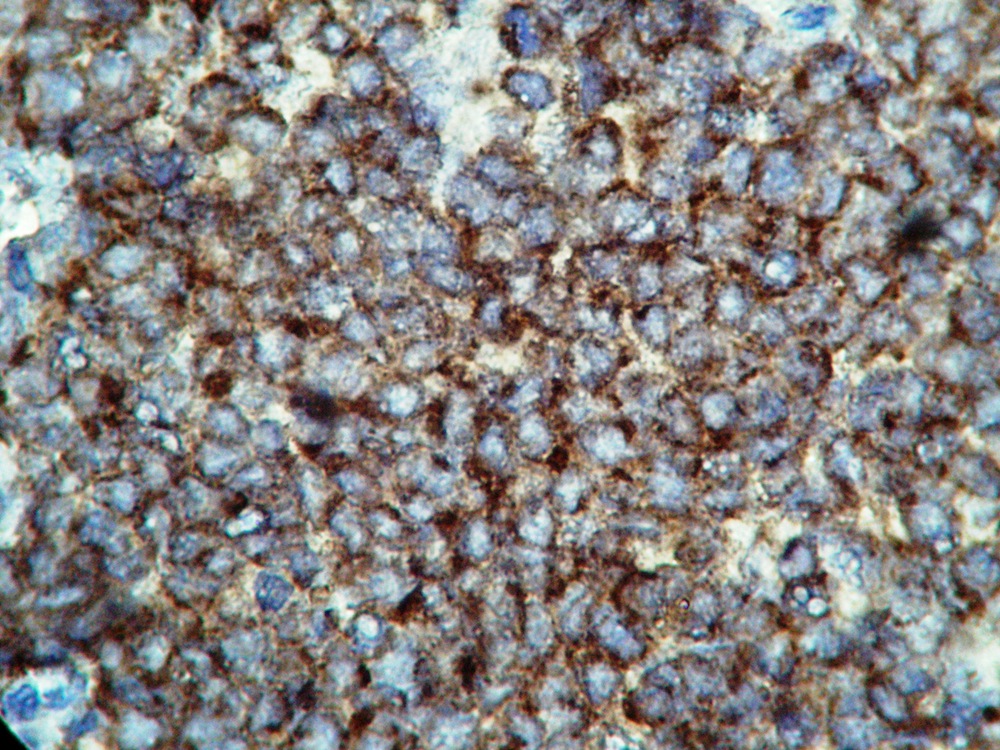
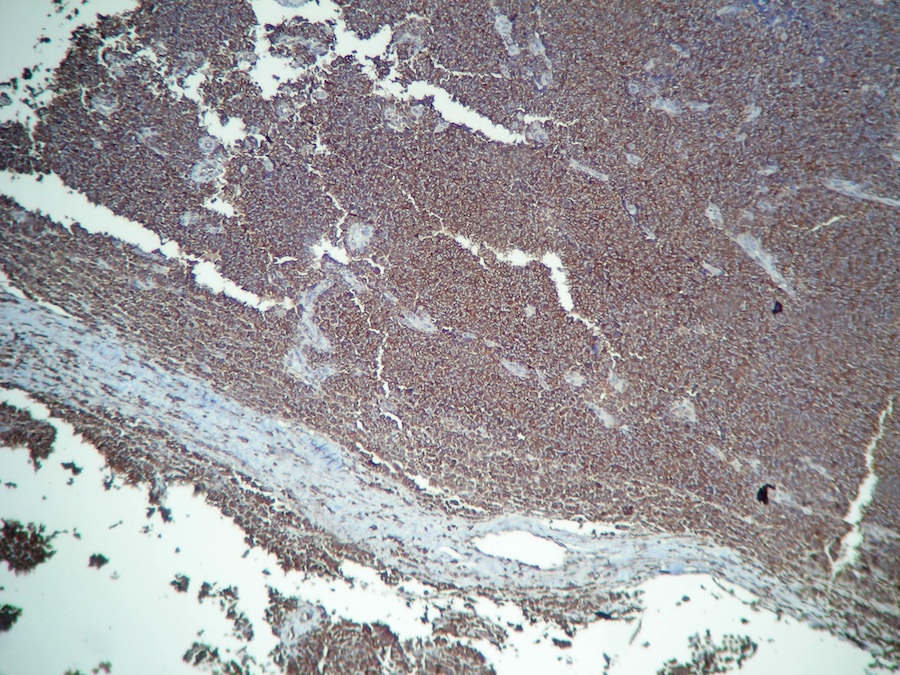
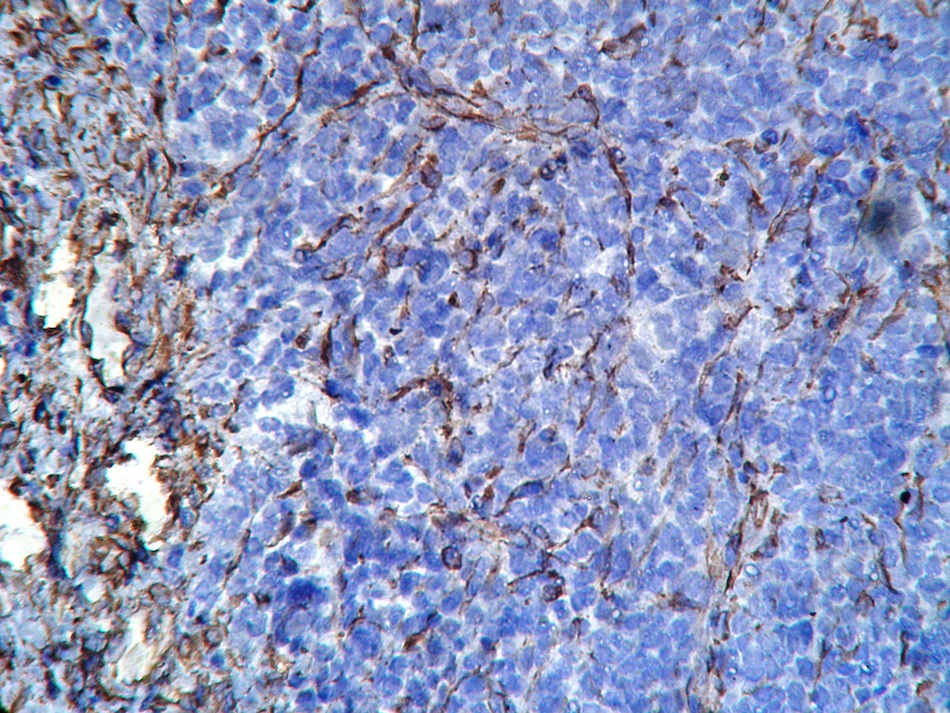
Immunostains:
CD99
MyoD1
NSE
PAS
Vimentin
Desmin
Discussion:
Bone scintigraphy shows a single hyperenhanced image at L5 with normal and symmetric uptake in hematopoietic areas.
Stains include CD99 (positive and strong in membrane), NSE (positive), PAS (positive in cytoplasmic granules), vimentin (negative) and desmin (negative). MyoD1 shows cytoplasmic staining, due to a cross reaction with an unknown antigen, which has been described in Ewing sarcoma / PNET and neuroblastoma (Dabbs & Thompson: Diagnostic Immunohistochemistry, 4th Edition, 2013).
Fewer than 10% of Ewing tumors arise in the vertebrae. In a study of 33 cases, the median age at diagnosis was 13 years and 64% were male (Med Pediatr Oncol 2001;37:30). 6 patients had metastatic disease and 10 had tumors 8 cm or larger. Primary sites were sacral (13), thoracic (10), lumbar (8) and cervical (2) vertebrae. Pain and neurologic deficits were common.
Histology shows sheets of small, round, uniform cells, 10-15 microns with scant clear cytoplasm, divided into irregular lobules by fibrous strands. The nuclei are round with indentations and small nucleoli. Homer-Wright rosettes (central fibrillary space) or pseudorosettes (cells arrange themselves around vessels) may be present (Bone-Ewing sarcoma / PNET).
The differential diagnosis includes other small blue cell tumors:
- Desmoplastic small round cell tumor
- Embryonal rhabdomyosarcoma
- Lymphoma: CD20+, older patients, polymorphic infiltrate
- Mesenchymal chondrosarcoma
- Metastatic neuroblastoma: patients younger than 5 years, primary should be evident
- Lymphoma
- Small cell osteosarcoma
Treatment is combination chemotherapy and local radiotherapy, with a 5 year survival of 48 - 70% (Eur J Cancer 2013;49:1314), comparable to this tumor at other sites. Most of the mortality is due to metastatic disease, which occurs in 30% (Case Rep Oncol Med 2012;2012:165289).
