
7 May 2014 - Case #311
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Raul Gonzalez, Vanderbilt University Medical Center, Tennessee (USA), for contributing this case.
Advertisement
Case #311
Clinical history:
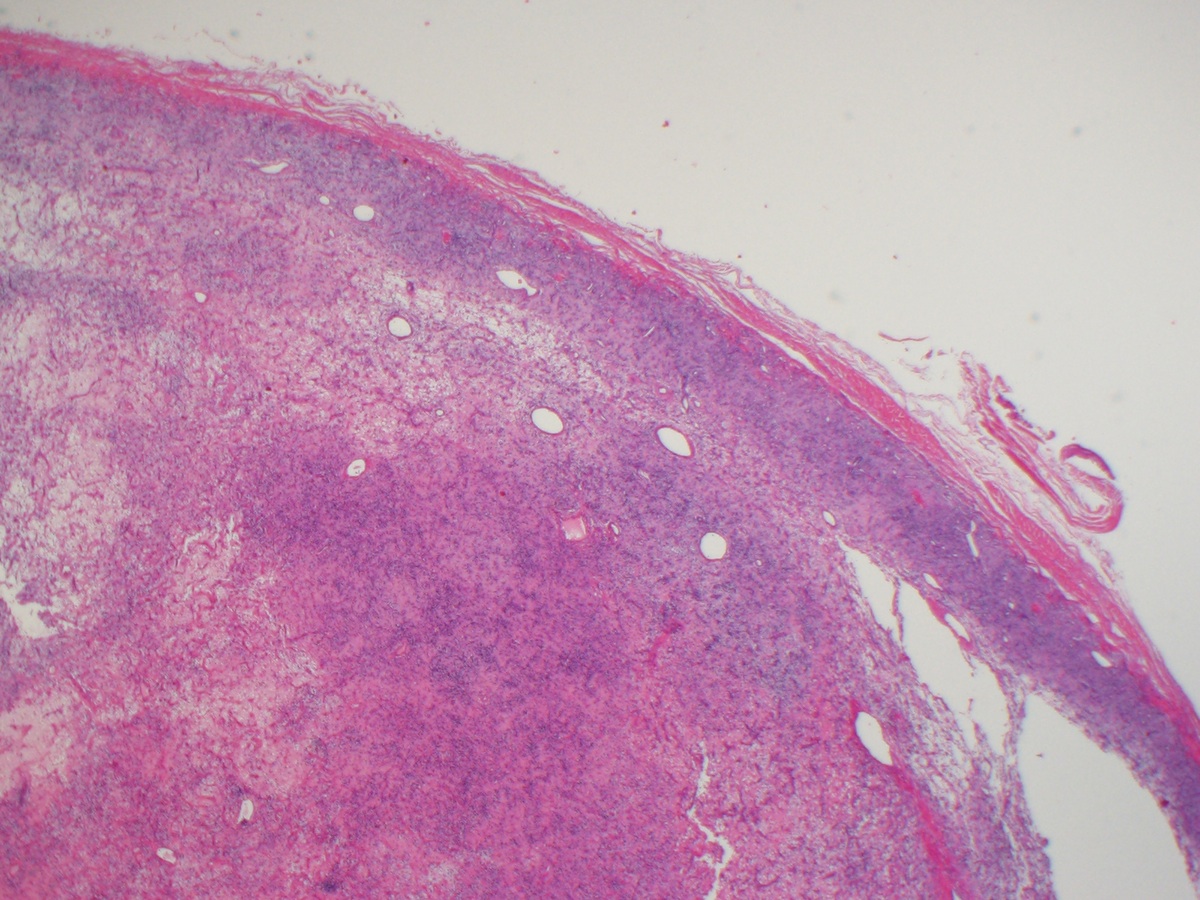
A 38 year old woman presented with a 4 cm ankle mass, which was biopsied.
Microscopic images:

What is your diagnosis?
Diagnosis: Angiofibroma of soft tissue of the ankle
Discussion:
Angiofibroma of soft tissue was first described in 2012 by Mario-Enrquez and Fletcher as a benign fibrovascular tumor that resembles a low grade sarcoma (Am J Surg Pathol 2012;36:500). These tumors typically present as a slow growing painless mass of the extremities and occur at all ages (median age 49 years), more commonly in women.
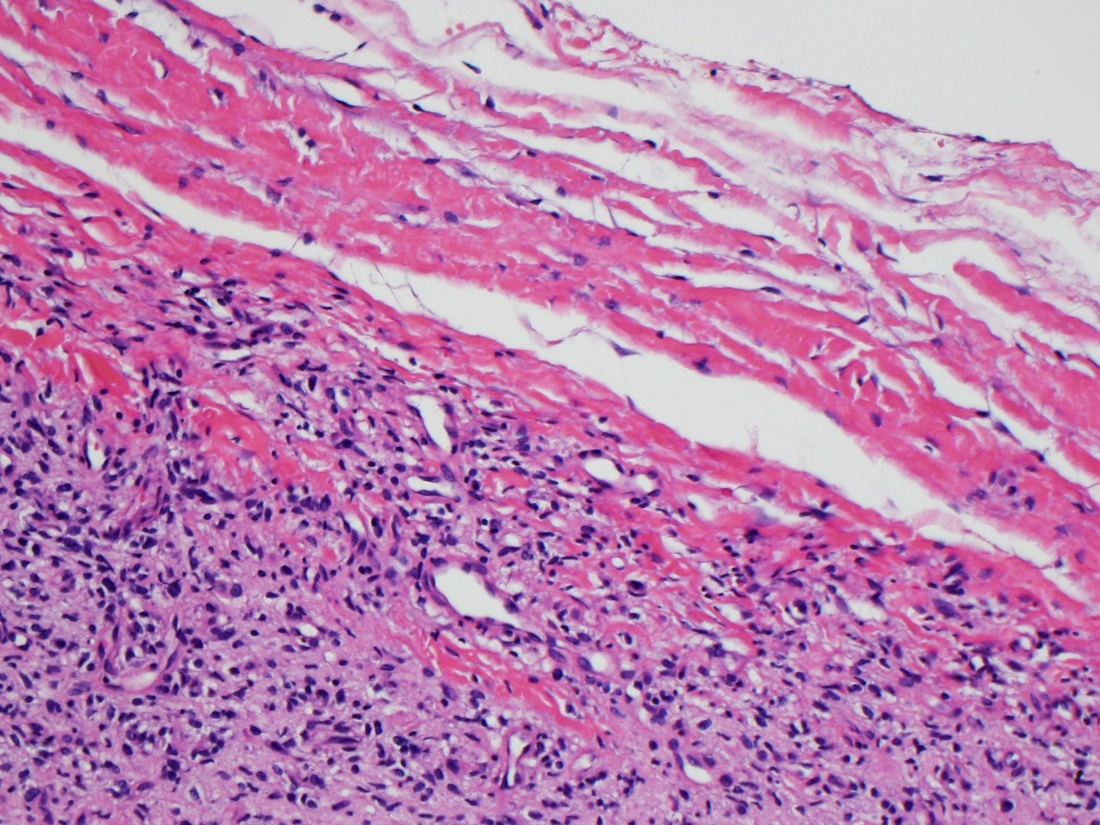
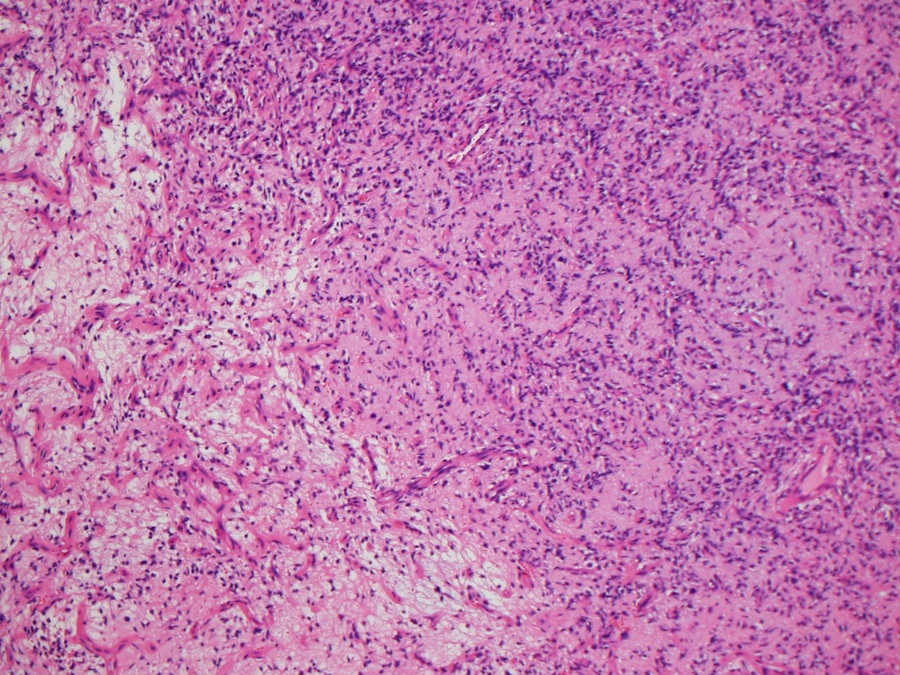
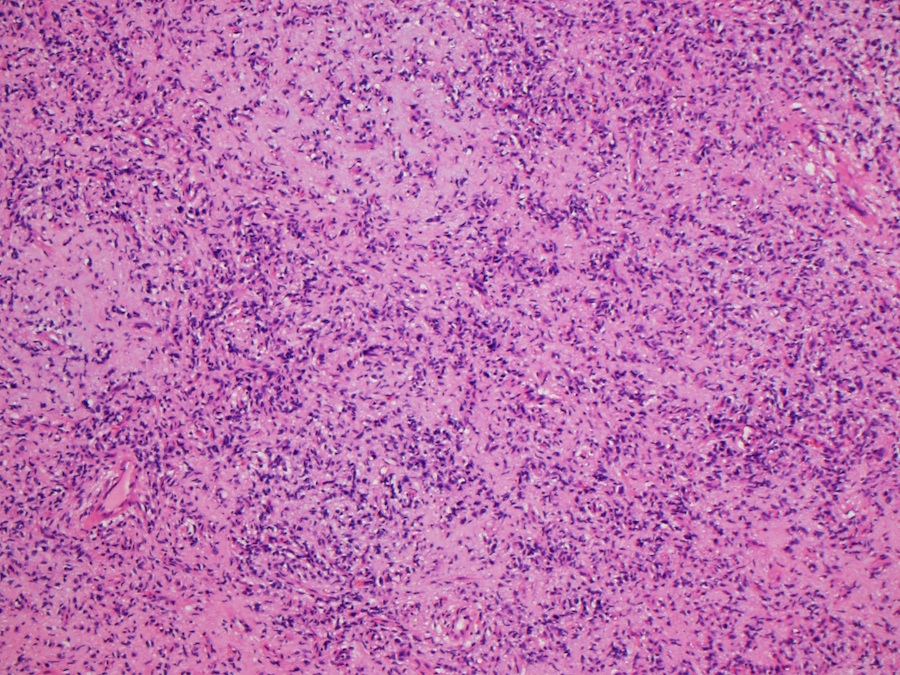
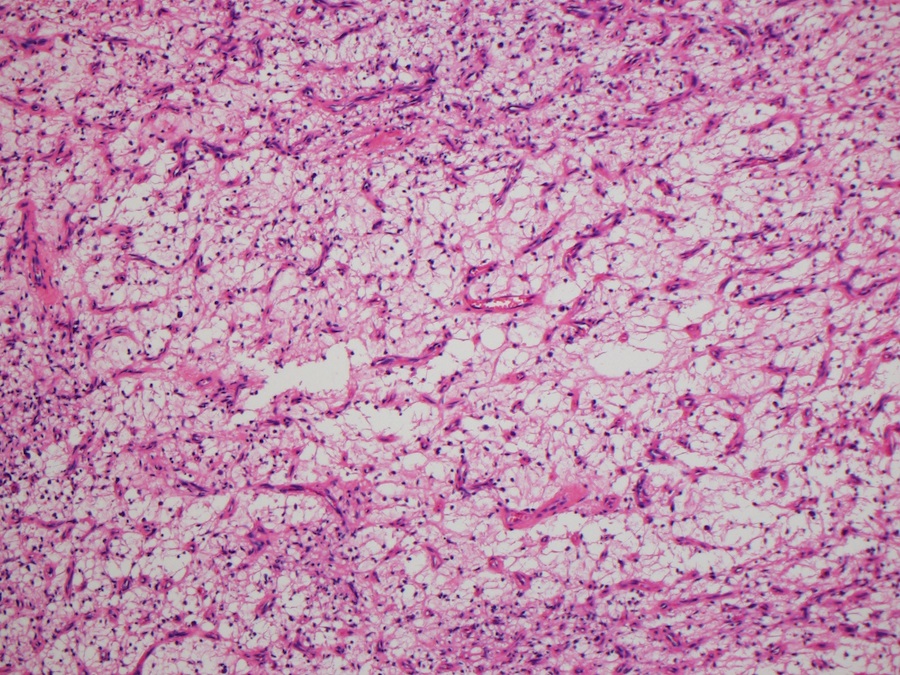
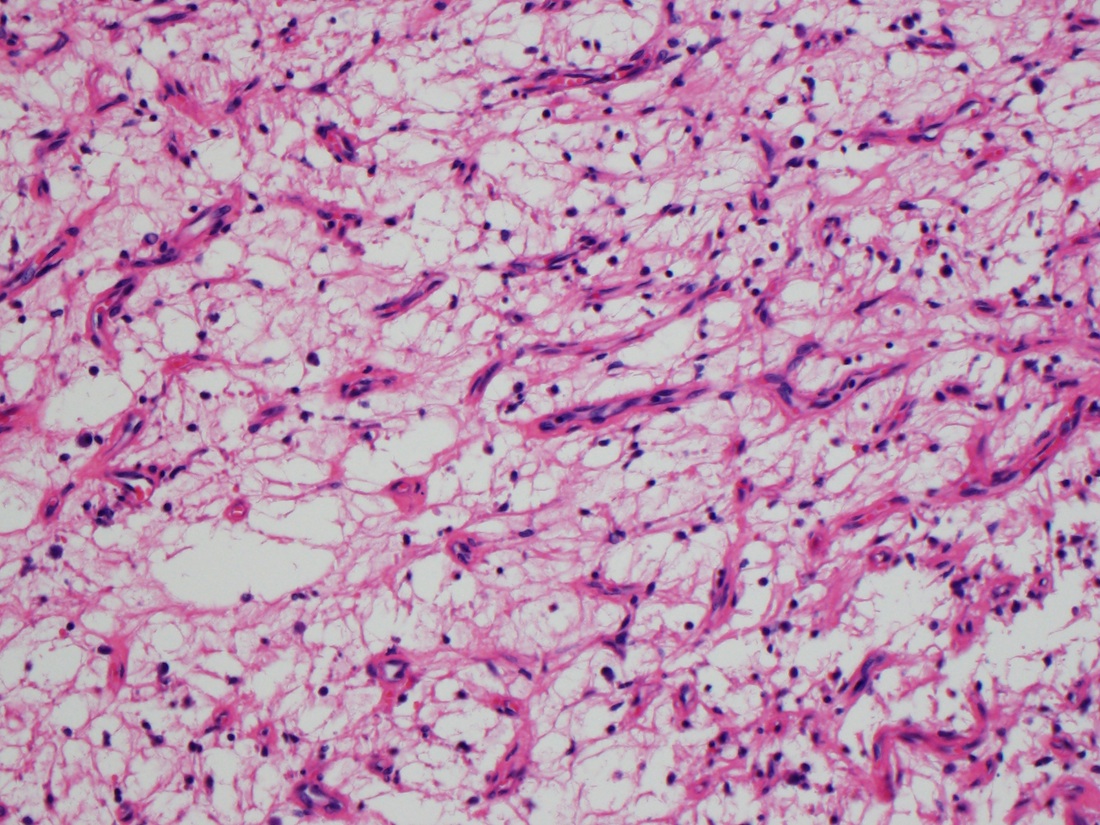
Grossly, the tumors are well circumscribed, median 3.5 cm. Histologically, there are 2 distinct components: (a) uniform proliferation of bland, spindled cells with scant cytoplasm and ovoid / tapered nuclei and (b) myxoid or collagenous stroma with prominent vasculature, usually small, branching, thin walled vessels. Occasional findings are mild mitotic activity, mild degenerative atypia, short fascicles, vaguely storiform or swirling arrangements (Int J Clin Exp Pathol 2013;6:2208).
Immunohistochemistry is not diagnostic. Tumor cells often express EMA (44%), and occasionally CD34, SMA or desmin but are consistently S100-. The t(5;8)(p15;q13) translocation is common, which results in a fusion of AHRR and NCOA2 (Genes Chromosomes Cancer 2012;51:510).
The differential diagnosis includes:
Excision is typically adequate, even with involved surgical margins, although local recurrence is possible. No metastases have been reported to date.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Raul Gonzalez, Vanderbilt University Medical Center, Tennessee (USA), for contributing this case.

Scientific Symposiums International Summer CME Series
Diagnosing Lymphomas and Leukemias: Challenges for the Surgical Pathologist
June 16-19, 2014
Hilton Head Island, South Carolina (USA)
Still looking to fulfill your 2014 CME, SAMS/MOCS accreditation?
Join us this summer for an ALL NEW Surgical Pathology course on Hilton Head Island, SC.
Register for our upcoming Surgical Pathology course being held this June in order to learn how to diagnose lymphomas and leukemias.
Our world-renowned faculty include Steven Swerdlow, M.D., Kathy Foucar, M.D., Marsha Kinney, M.D. and Lawrence Weiss, M.D.
This course is one not to be missed!
Website news:
(1) We have updated numerous topics in the Ovary-nontumor chapter to add images with captions from Scully, Young & Clement: Atlas of Tumor Pathology (AFIP 3rd series, Volume 23, 1999).
(2) We posted a detailed and important article, Part A and Medical Directorship Contracts, by Mick Raich, Vachette Pathology.
Visit and follow our Blog to see recent updates to the website.
(1) We have updated numerous topics in the Ovary-nontumor chapter to add images with captions from Scully, Young & Clement: Atlas of Tumor Pathology (AFIP 3rd series, Volume 23, 1999).
(2) We posted a detailed and important article, Part A and Medical Directorship Contracts, by Mick Raich, Vachette Pathology.
Visit and follow our Blog to see recent updates to the website.
Case #311
Clinical history:
A 38 year old woman presented with a 4 cm ankle mass, which was biopsied.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Angiofibroma of soft tissue of the ankle
Discussion:
Angiofibroma of soft tissue was first described in 2012 by Mario-Enrquez and Fletcher as a benign fibrovascular tumor that resembles a low grade sarcoma (Am J Surg Pathol 2012;36:500). These tumors typically present as a slow growing painless mass of the extremities and occur at all ages (median age 49 years), more commonly in women.
Grossly, the tumors are well circumscribed, median 3.5 cm. Histologically, there are 2 distinct components: (a) uniform proliferation of bland, spindled cells with scant cytoplasm and ovoid / tapered nuclei and (b) myxoid or collagenous stroma with prominent vasculature, usually small, branching, thin walled vessels. Occasional findings are mild mitotic activity, mild degenerative atypia, short fascicles, vaguely storiform or swirling arrangements (Int J Clin Exp Pathol 2013;6:2208).
Immunohistochemistry is not diagnostic. Tumor cells often express EMA (44%), and occasionally CD34, SMA or desmin but are consistently S100-. The t(5;8)(p15;q13) translocation is common, which results in a fusion of AHRR and NCOA2 (Genes Chromosomes Cancer 2012;51:510).
The differential diagnosis includes:
- Cellular angiofibroma: usually in genital region, more cellular, usually ER+, PR+
- Low grade fibromyxoid sarcoma: often > 6 cm and infiltrative, 45% have epithelioid areas, 40% contain poorly formed but large collagen rosettes
- Low grade myxofibrosarcoma: infiltrative borders, often sends out long tentacles, more solid areas are often seen similar to typical undifferentiated pleomorphic sarcom; has curvilinear vessels (thick walled with broad arc) with condensation of cells around vessels
- Myxoid liposarcoma: prominent chicken wire vasculature, numerous signet ring lipoblasts particularly at periphery of lobules, mucoid matrix rich in hyaluronidase sensitive acid mucopolysaccharides, may have large mucoid pools, S100+
- Solitary fibrous tumor: fibroblast-like cells with patternless pattern, thick bands of collagen and prominent branching, hyalinized vessels; CD34+, CD99+
Excision is typically adequate, even with involved surgical margins, although local recurrence is possible. No metastases have been reported to date.
