
26 March 2014 - Case #305
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Raul Gonzalez, Vanderbilt University Medical Center, Tennessee (USA) for contributing this case.
Case #305
Clinical history:
A 63 year old man with a history of tubular adenoma presented with a new colon polyp.
Microscopic images:
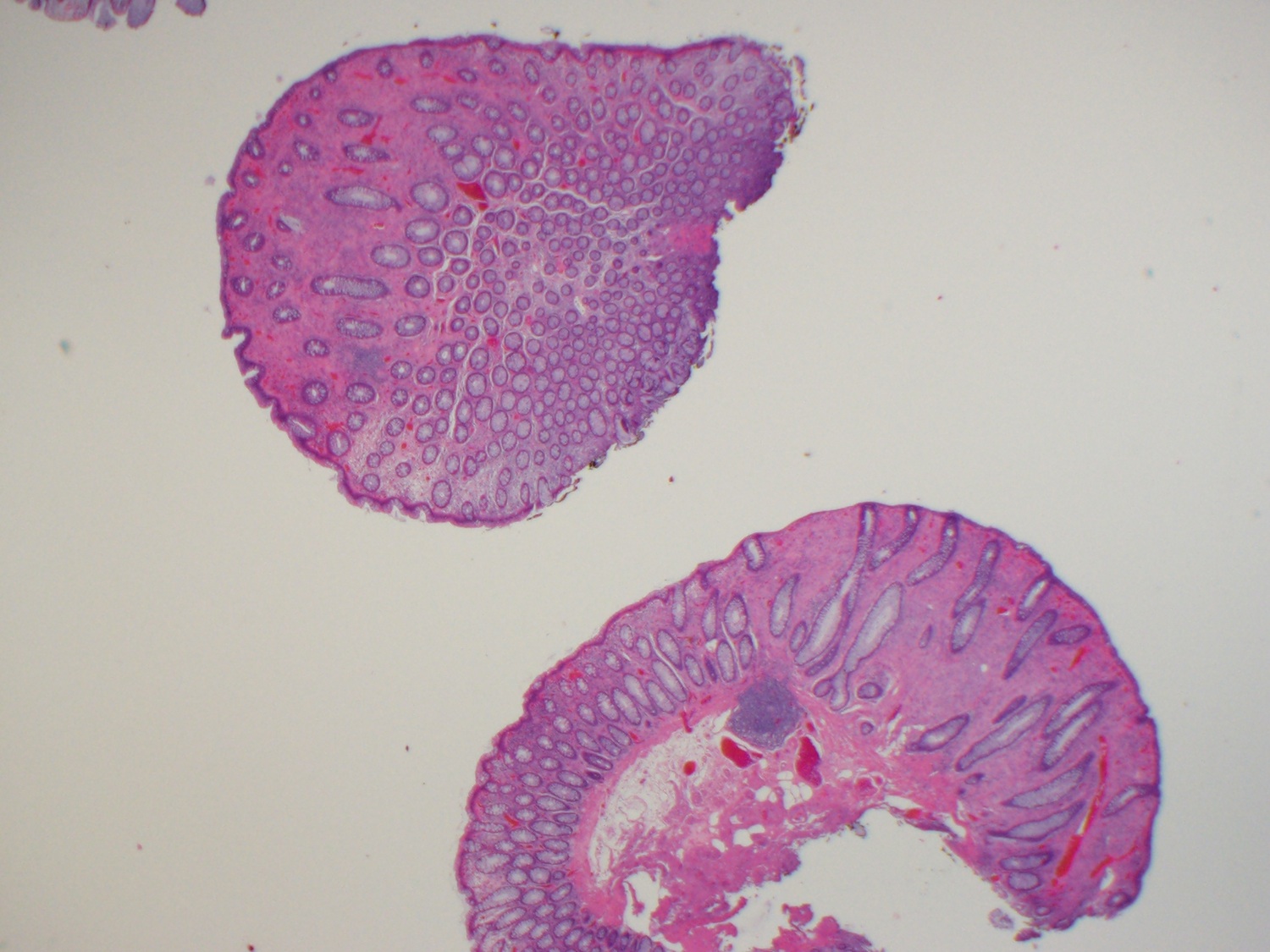
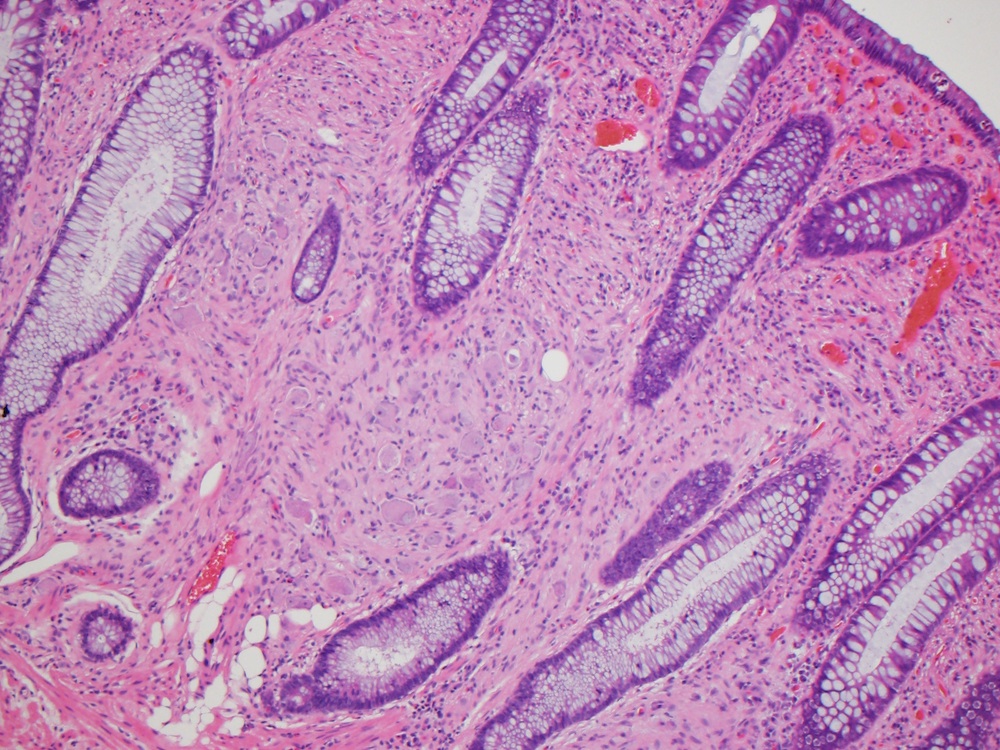
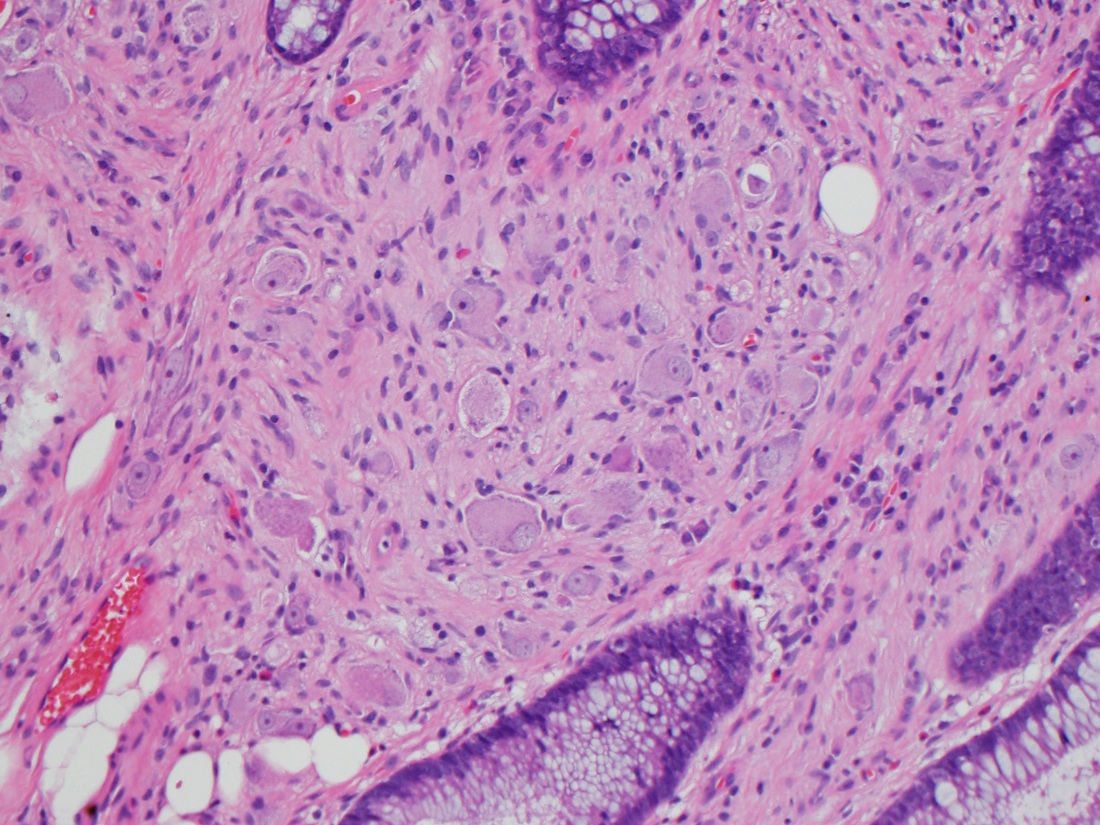
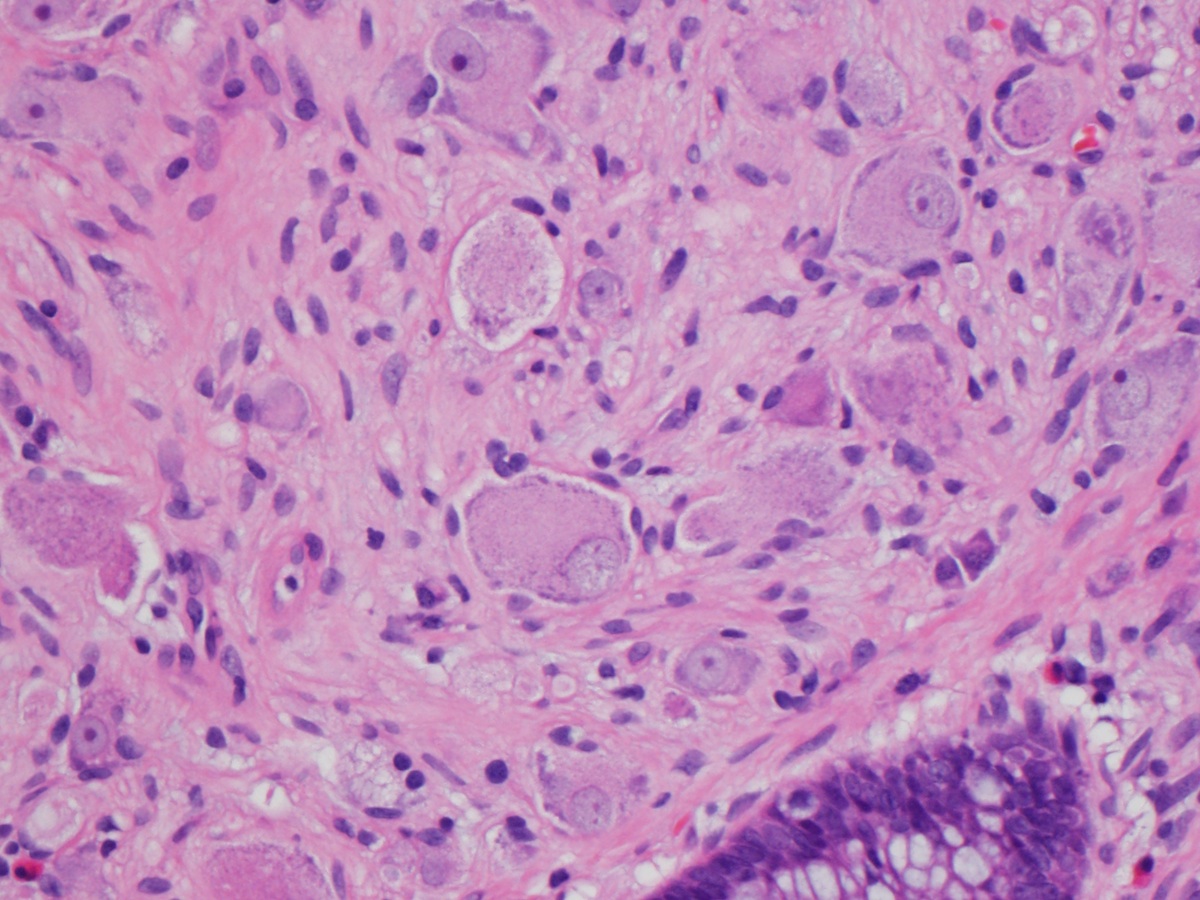
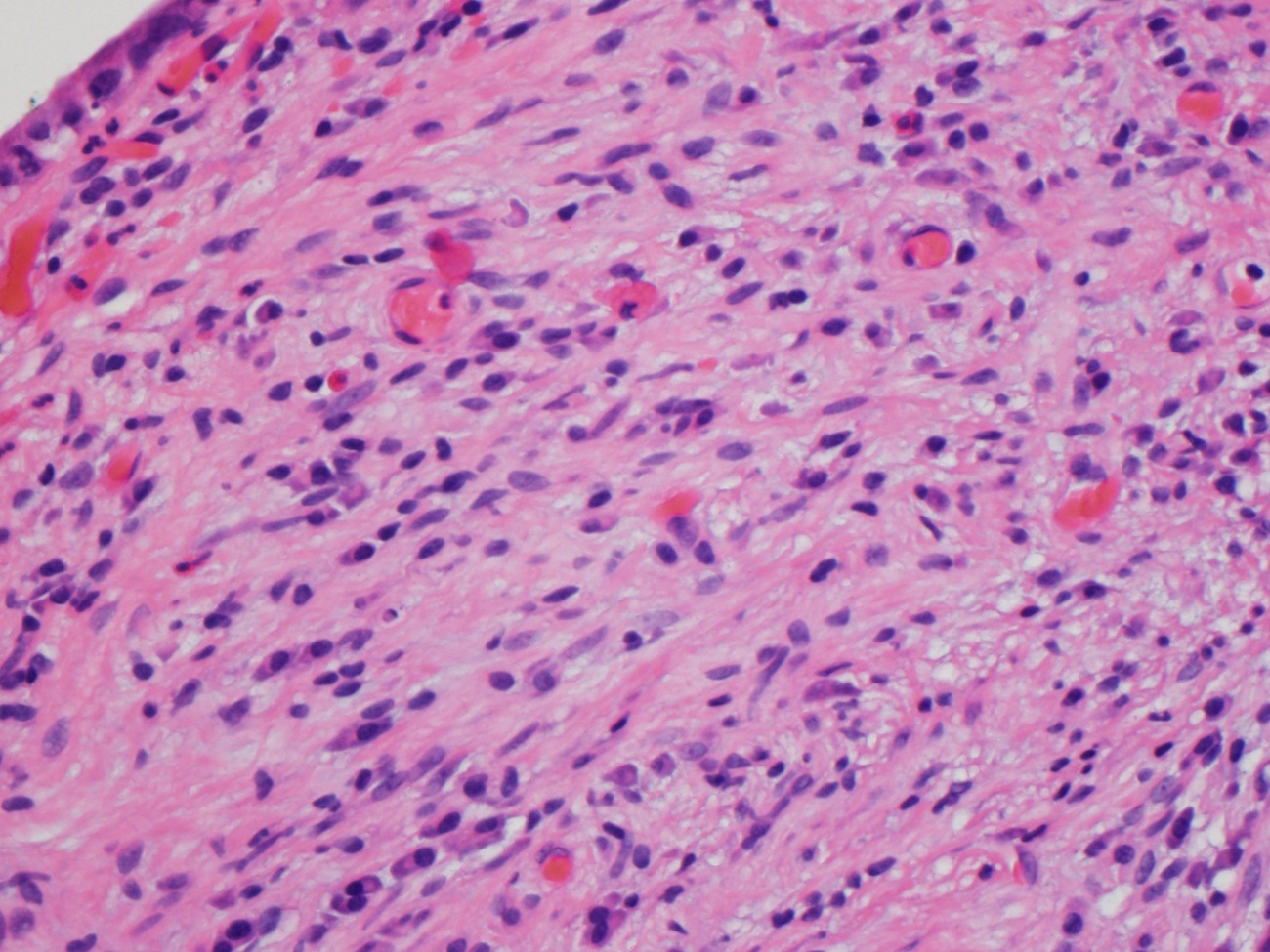
What is your diagnosis?
Diagnosis: Ganglioneuroma (colon polyp)
Discussion:
Ganglioneuroma is a rare, benign, slow growing, peripheral neuroblastic tumor characterized by ganglion cell hyperplasia, nerve fibers and supporting cells. It derives from sympathetic neuronal cells and occurs mostly in children. It is found in various anatomic locations, but only rarely in the colon, where it is associated with multiple endocrine neoplasia type IIB (MEN IIB), neurofibromatosis type 1 (NF1), juvenile polyposis, polyposis coli, tuberous sclerosis and the PTEN hamartoma tumor syndrome (which includes Cowden and Bannayan-Riley-Ruvalcaba syndromes) (J Med Case Rep 2012;6:304, World J Gastroenterol 2014;20:1833). Syndromic cases tend to be associated with ganglioneuromatosis, not solitary polyps.
Solitary polyps are often incidental findings at endoscopy, although they are rarely associated with colonic intussusception (J Pediatr Surg 2009;44:e17). Excision is adequate treatment.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Raul Gonzalez, Vanderbilt University Medical Center, Tennessee (USA) for contributing this case.
Website news:
(1) We received a comment about establishing a Forum for pathology related questions. Is this needed, or does this already exist? Let us know what you think.
Visit and follow our Blog to see recent updates to the website.
(1) We received a comment about establishing a Forum for pathology related questions. Is this needed, or does this already exist? Let us know what you think.
Visit and follow our Blog to see recent updates to the website.
Case #305
Clinical history:
A 63 year old man with a history of tubular adenoma presented with a new colon polyp.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Ganglioneuroma (colon polyp)
Discussion:
Ganglioneuroma is a rare, benign, slow growing, peripheral neuroblastic tumor characterized by ganglion cell hyperplasia, nerve fibers and supporting cells. It derives from sympathetic neuronal cells and occurs mostly in children. It is found in various anatomic locations, but only rarely in the colon, where it is associated with multiple endocrine neoplasia type IIB (MEN IIB), neurofibromatosis type 1 (NF1), juvenile polyposis, polyposis coli, tuberous sclerosis and the PTEN hamartoma tumor syndrome (which includes Cowden and Bannayan-Riley-Ruvalcaba syndromes) (J Med Case Rep 2012;6:304, World J Gastroenterol 2014;20:1833). Syndromic cases tend to be associated with ganglioneuromatosis, not solitary polyps.
Solitary polyps are often incidental findings at endoscopy, although they are rarely associated with colonic intussusception (J Pediatr Surg 2009;44:e17). Excision is adequate treatment.
