
26 February 2014 - Case #302
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Don Xu, University of California, San Diego, for contributing this case.
Case #302
Clinical history:
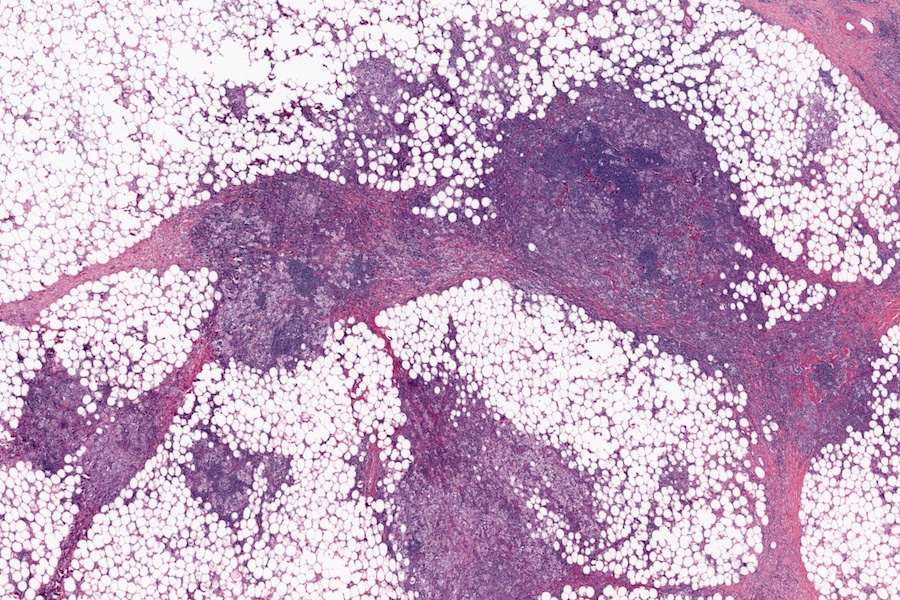
A 45 year old woman presented with a right breast mass, which was biopsied.
Microscopic images:


What is your diagnosis?
Diagnosis: Rosai-Dorfman disease
Discussion:
Rosai-Dorfman disease, also called sinus histiocytosis with massive lymphadenopathy, is a disorder of massive lymph node involvement that may also involve extranodal sites. It often presents with systemic symptoms (fever, leukocytosis, anemia), and most commonly involves the skin, subcutis / soft tissue, upper respiratory tract, bone, eye or CNS. Cases in the breast are rare.
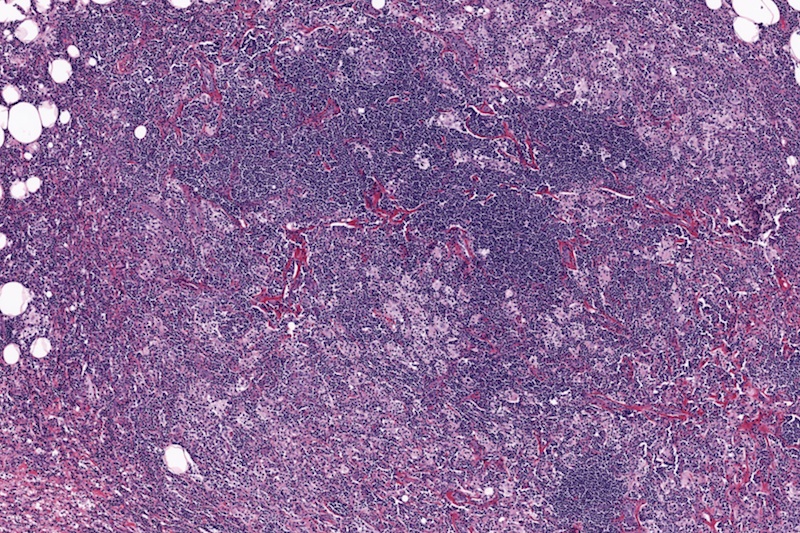
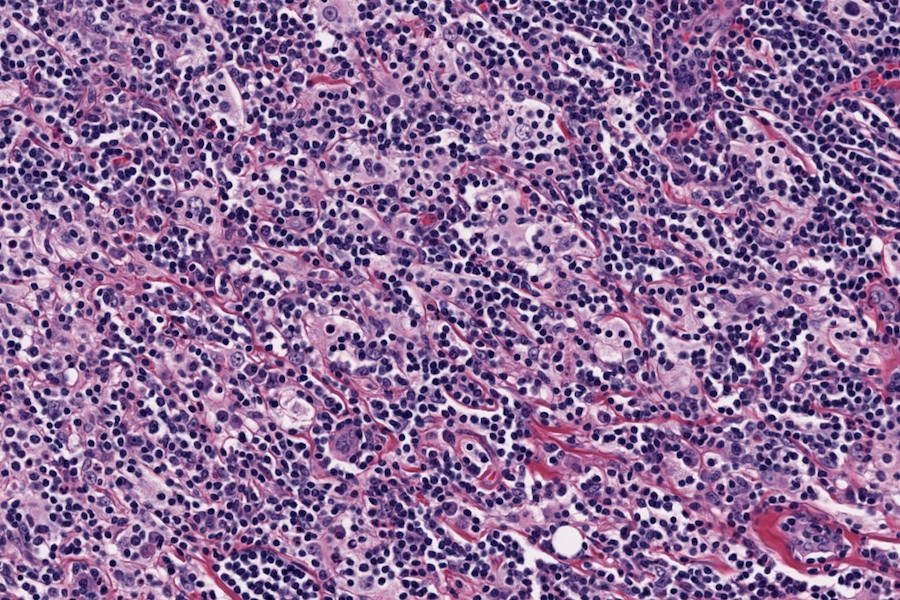
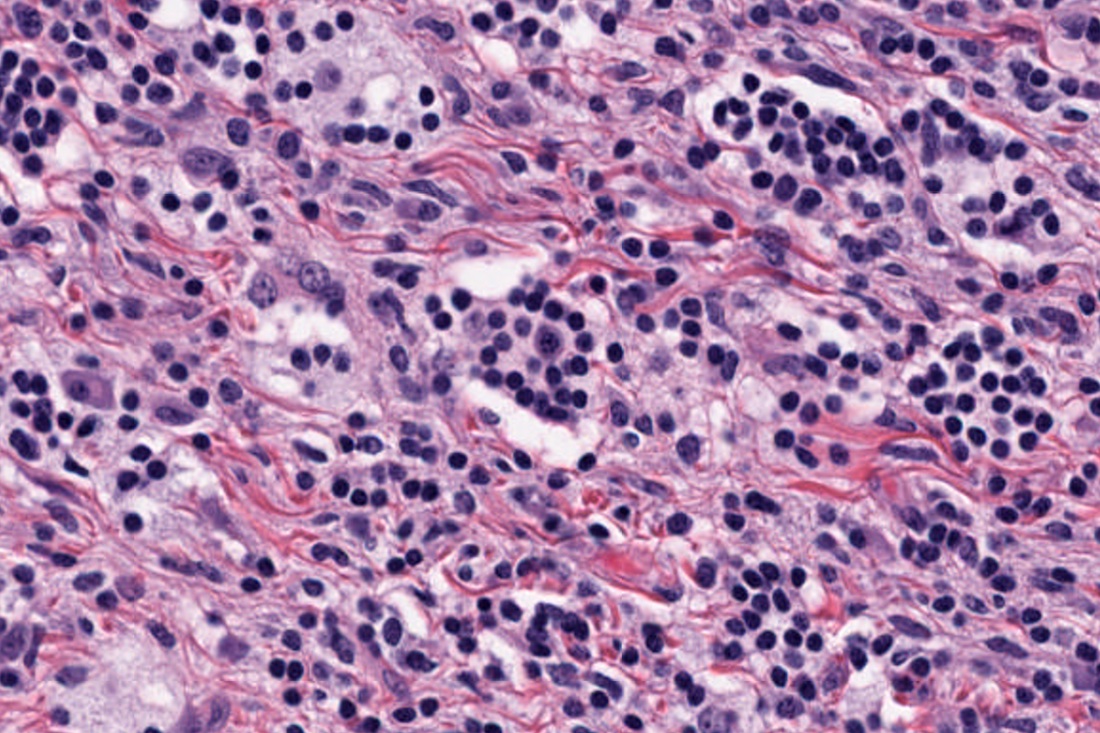
Grossly, there are circumscribed, often multinodular masses in the breast stroma, which typically do not involve the dermis or subcutis. Histologically, large histiocytes are present with abundant pale eosinophilic cytoplasm and mildly atypical round vesicular nuclei (Am J Surg Pathol 1997;21:664). The background shows lymphocytophagocytosis (emperipolesis) in a background of mature lymphocytes and plasma cells. The histiocytes are immunoreactive for S100 and CD68 and negative for CD1a.
The differential diagnosis includes other histiocyte-like disorders:
Rosai-Dorfman disease usually resolves spontaneously, although systemic cases may cause death. Recent reports suggest that a subset of Rosai-Dorfman disease exhibit features of IgG4 related disease (Korean J Pathol 2012;46:489, Am J Clin Pathol 2013;139:622, Am J Clin Pathol 2013;140:395).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Don Xu, University of California, San Diego, for contributing this case.
Website news:
(1) We have just about converted all 80 chapters to our popular topic format - see the recently updated Aggressive Angiomyxoma topic as an example. Next we will be adding more images from various sources, adding some new chapter sections, and continuing / expanding our topic reviews.
(2) We are looking for authors for these existing chapters: Clinical Chemistry and CNS nontumor, and for new chapters on Heart-nontumor, Informatics, Muscle Pathology, Quality Control (CP), Pediatric Pathology and Syndromes. Authors first provide us an outline of what they want to do, then start with a topic or two. You don't have to complete the entire chapter. If interested, contact us.
(3) We have updated these CD Markers: CD20 and CD21, and added these new stains: MAST2 (rearranged in 2% of invasive breast carcinomas), MED12 (mutated in most uterine leiomyomas), PHF1 (rearranged in most ossifying fibromyxoid tumors), SOX10 (expressed by melanocytes / cells of neural crest origin, breast myoepithelial cells).
(4) We have added new Board Review questions for January and February 2014, courtesy of BoardVitals, which are accessible via our CME page. They relate to translocations / cytogenetics and clinical pathology.
(5) We continue to add conferences to our Conferences page. Conferences are now listed by date, date posted, subspecialty and location. To see the most recently posted conferences, click here. Are your favorite conferences advertising at PathologyOutlines.com? If not, please suggest that they do so. The cost is modest, but the rewards are great.
Visit and follow our Blog to see recent updates to the website.
(1) We have just about converted all 80 chapters to our popular topic format - see the recently updated Aggressive Angiomyxoma topic as an example. Next we will be adding more images from various sources, adding some new chapter sections, and continuing / expanding our topic reviews.
(2) We are looking for authors for these existing chapters: Clinical Chemistry and CNS nontumor, and for new chapters on Heart-nontumor, Informatics, Muscle Pathology, Quality Control (CP), Pediatric Pathology and Syndromes. Authors first provide us an outline of what they want to do, then start with a topic or two. You don't have to complete the entire chapter. If interested, contact us.
(3) We have updated these CD Markers: CD20 and CD21, and added these new stains: MAST2 (rearranged in 2% of invasive breast carcinomas), MED12 (mutated in most uterine leiomyomas), PHF1 (rearranged in most ossifying fibromyxoid tumors), SOX10 (expressed by melanocytes / cells of neural crest origin, breast myoepithelial cells).
(4) We have added new Board Review questions for January and February 2014, courtesy of BoardVitals, which are accessible via our CME page. They relate to translocations / cytogenetics and clinical pathology.
(5) We continue to add conferences to our Conferences page. Conferences are now listed by date, date posted, subspecialty and location. To see the most recently posted conferences, click here. Are your favorite conferences advertising at PathologyOutlines.com? If not, please suggest that they do so. The cost is modest, but the rewards are great.
Visit and follow our Blog to see recent updates to the website.
Case #302
Clinical history:
A 45 year old woman presented with a right breast mass, which was biopsied.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Rosai-Dorfman disease
Discussion:
Rosai-Dorfman disease, also called sinus histiocytosis with massive lymphadenopathy, is a disorder of massive lymph node involvement that may also involve extranodal sites. It often presents with systemic symptoms (fever, leukocytosis, anemia), and most commonly involves the skin, subcutis / soft tissue, upper respiratory tract, bone, eye or CNS. Cases in the breast are rare.
Grossly, there are circumscribed, often multinodular masses in the breast stroma, which typically do not involve the dermis or subcutis. Histologically, large histiocytes are present with abundant pale eosinophilic cytoplasm and mildly atypical round vesicular nuclei (Am J Surg Pathol 1997;21:664). The background shows lymphocytophagocytosis (emperipolesis) in a background of mature lymphocytes and plasma cells. The histiocytes are immunoreactive for S100 and CD68 and negative for CD1a.
The differential diagnosis includes other histiocyte-like disorders:
- Erdheim-Chester disease: usually a systemic disease with large foamy histiocytes containing lipid
- Idiopathic granulomatous mastitis: granulomas with epithelioid histiocytes
- Langerhans cell histiocytosis: Langerhans cells are large, ovoid with pale pink cytoplasm and indented bland nuclei; CD1a+
- Tuberculosis or other infectious granulomas
- Benign fibrous histiocytoma: storiform pattern of spindled and bland fibroblasts and histiocyte-like cells in mid-dermis and subcutaneous tissue with infiltrative margins but sparing epidermis
Rosai-Dorfman disease usually resolves spontaneously, although systemic cases may cause death. Recent reports suggest that a subset of Rosai-Dorfman disease exhibit features of IgG4 related disease (Korean J Pathol 2012;46:489, Am J Clin Pathol 2013;139:622, Am J Clin Pathol 2013;140:395).
