
31 July 2013 - Case #281
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mingyi Chen, University of California Davis Medical Center (USA), for contributing this case and the discussion.
 Advertisement
Advertisement
Case #281
Clinical history:
A 48 year old man presented with a left eyelid mass. PET-CT scan showed a markedly increased uptake in the ocular region. An excisional biopsy was performed.
Radiology images:
Microscopic images:

What is your diagnosis?
Diagnosis: Ocular adnexal mantle cell lymphoma
Immunostains:
Discussion:
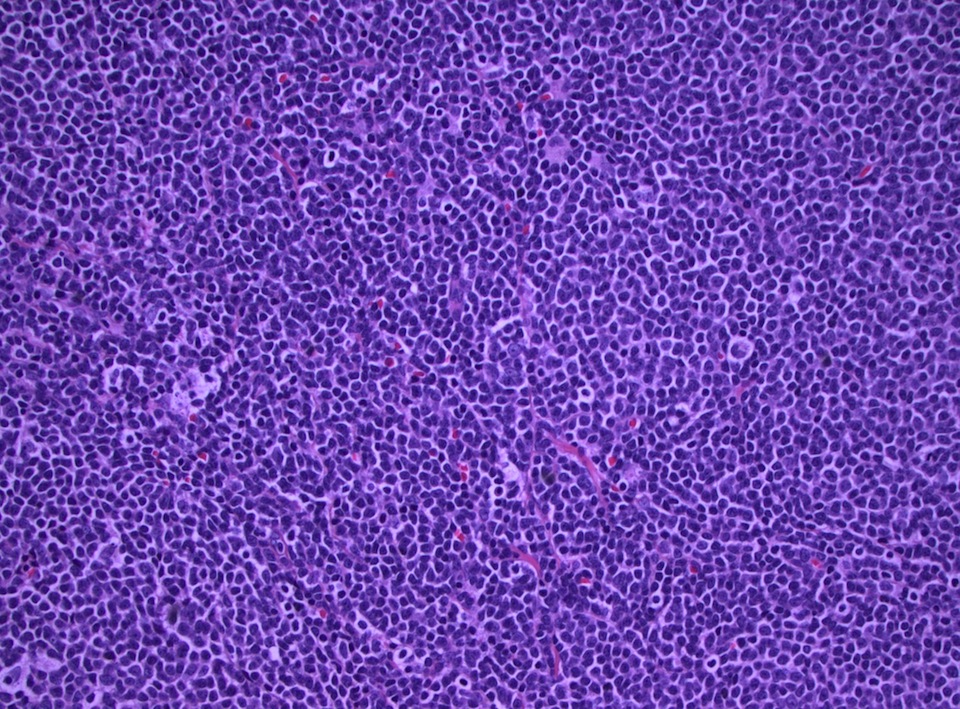
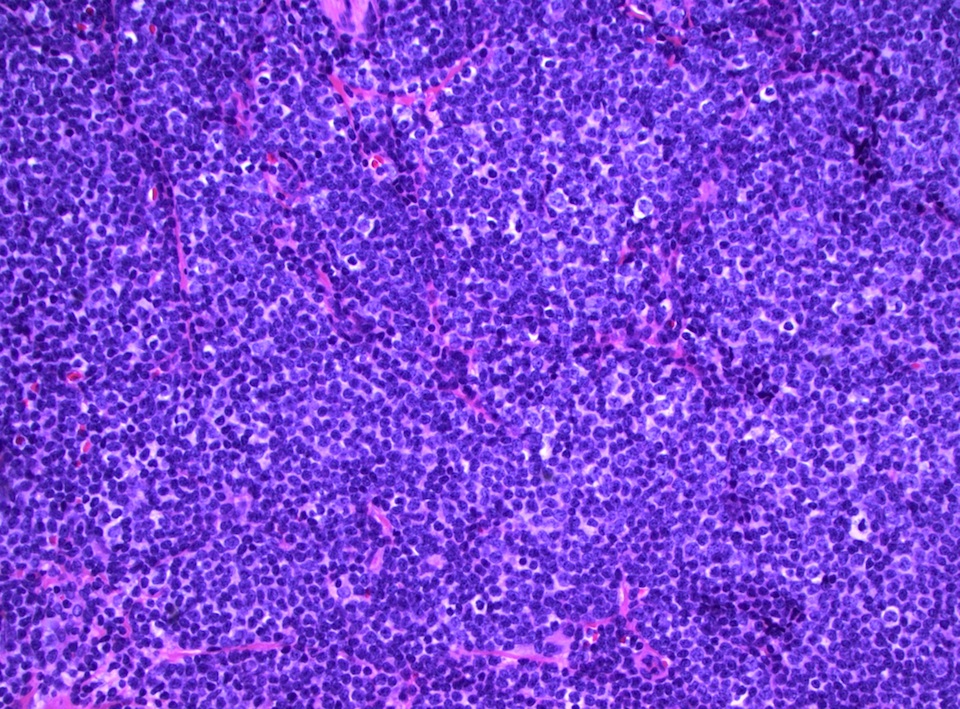
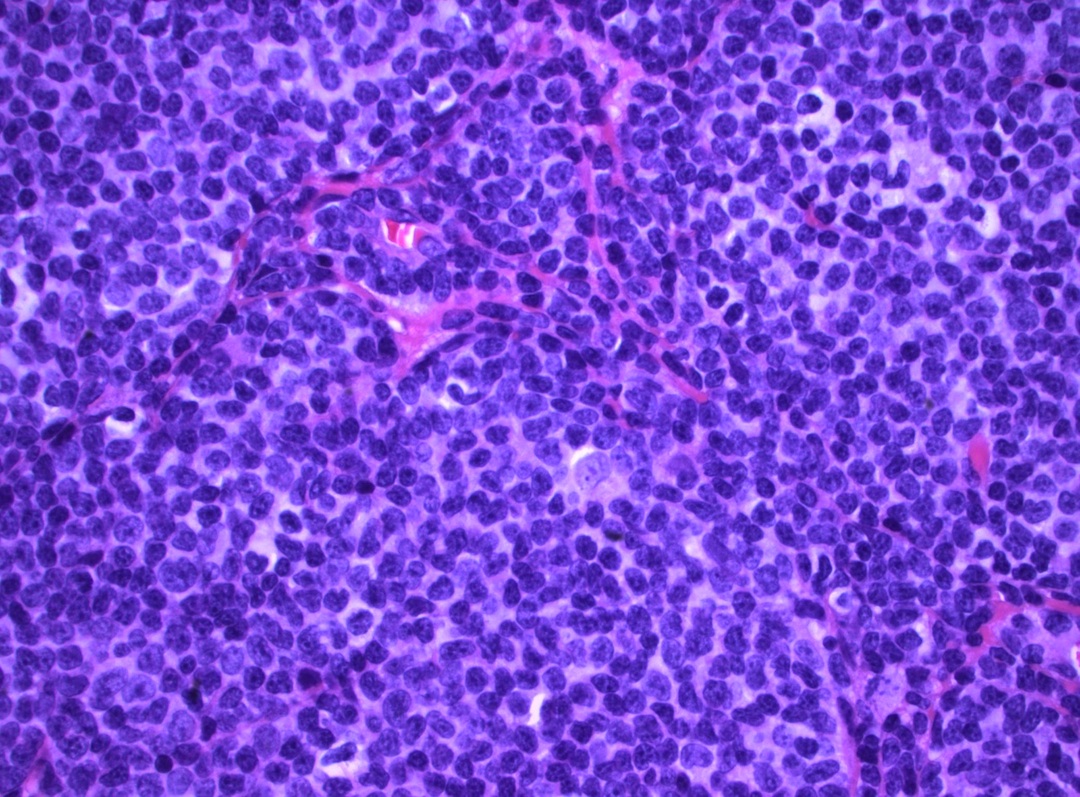
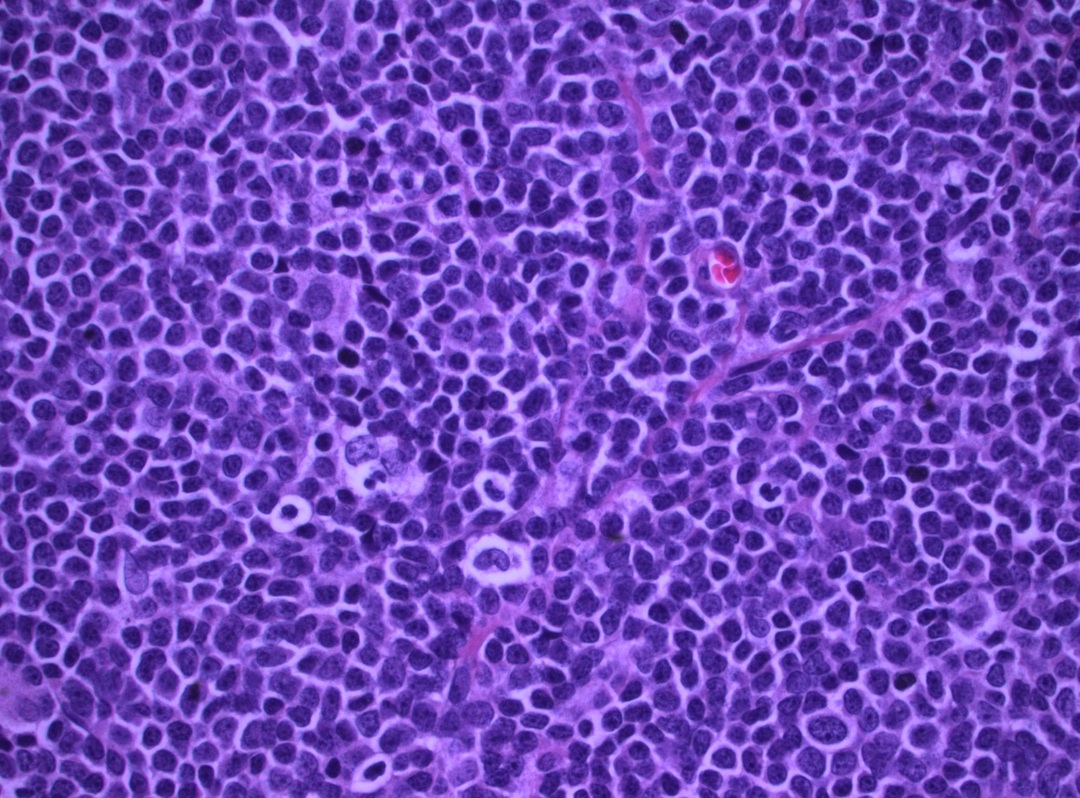
The H&E stained sections show sheets of an atypical lymphoid infiltrate with occasional hyalinized small vessels in the background. The tumor cells are monomorphic, small mature lymphocytes with scant cytoplasm, round to oval, cleaved nuclei, dense chromatin and inconspicuous nucleoli. No mitotic figures were seen. Flow cytometry (not shown) revealed monoclonal B cells with lambda light chain restriction, which coexpress CD19 and CD5. These cells were also positive for CD20 (bright) and FMC7, and are negative for CD23, CD10 and CD11c. Immunostains demonstrated that the neoplastic cells were B cells (CD20+, PAX5+) with coexpression of BCL2, CD5, CD43 and cyclin D1, and they were negative for AE1 / AE3, CD3, CD10, CD23 and CD30. The cell proliferation index marker Ki67 was 20 - 30%, confirming a relatively low grade process. Conventional cytogenetics analysis showed 46, XY, t(11;14)(q13;q32).
Ocular lymphomas can be primary or secondary, and occur in the orbit, conjunctiva and eyelids. Most lymphomas in the ocular adnexa are B cell non-Hodgkin lymphomas, most commonly extranodal marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALToma). Less common B cell subtypes include lymphoplasmacytic lymphoma, mantle cell lymphoma, plasmacytoma and follicular lymphoma. At all sites, mantle cell lymphoma (MCL) represents 3 - 5% of non-Hodgkin lymphomas. It predominantly occurs in older ages with a higher frequency in men, usually presenting with widespread disease and an aggressive course. Mantle cell lymphoma most commonly occurs in lymph nodes and in the GI tract but it presents as secondary involvement of ocular adnexal structures in 6% of the ocular lymphomas. There are limited studies of primary ocular mantle cell lymphoma.
References: Arch Ophthalmol 2007;125:1668, Br J Ophthalmol 2009;93:1047, Semin Diagn Pathol 2011;28:245
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Mingyi Chen, University of California Davis Medical Center (USA), for contributing this case and the discussion.
Advertisement
Website news:
(1) We have updated the Joints chapter based on reviews by Vijay Shankar, M.D.
(2) We have added new Board Review questions, courtesy of BoardVitals, which is accessible via our CME page.
(3) We have recently updated these topics in our Stains and CD Markers chapters based on the reviews by Nat Pernick, M.D.: CD Markers-general, CD1, CD1a, CD1b, CD1c, CD1d, CD1e, enzyme cytochemistry, ATM, Hansel stain, keratin AE1/AE3. We now have a plan to update all the Stains and CD Markers on a regular basis. If topics are missing, or you are interested in doing a review, please contact us at comments@pathologyoutlines.com.
(4) On 23 July 2013, we had record traffic of 18,131 visits. Let us know what we can do to make PathologyOutlines.com even more useful to you.
Visit and follow our Blog to see recent updates to the website.
(1) We have updated the Joints chapter based on reviews by Vijay Shankar, M.D.
(2) We have added new Board Review questions, courtesy of BoardVitals, which is accessible via our CME page.
(3) We have recently updated these topics in our Stains and CD Markers chapters based on the reviews by Nat Pernick, M.D.: CD Markers-general, CD1, CD1a, CD1b, CD1c, CD1d, CD1e, enzyme cytochemistry, ATM, Hansel stain, keratin AE1/AE3. We now have a plan to update all the Stains and CD Markers on a regular basis. If topics are missing, or you are interested in doing a review, please contact us at comments@pathologyoutlines.com.
(4) On 23 July 2013, we had record traffic of 18,131 visits. Let us know what we can do to make PathologyOutlines.com even more useful to you.
Visit and follow our Blog to see recent updates to the website.
Case #281
Clinical history:
A 48 year old man presented with a left eyelid mass. PET-CT scan showed a markedly increased uptake in the ocular region. An excisional biopsy was performed.
Radiology images:
PET scan
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Ocular adnexal mantle cell lymphoma
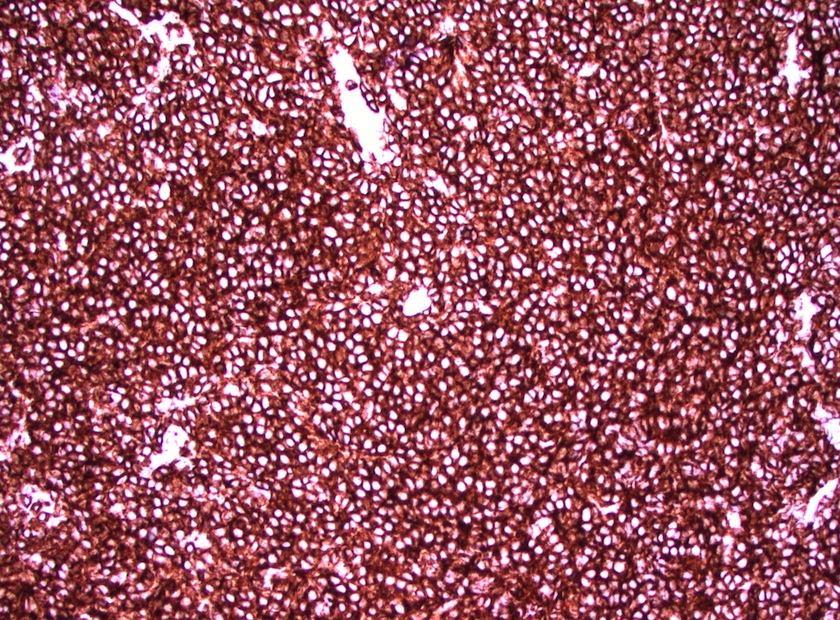
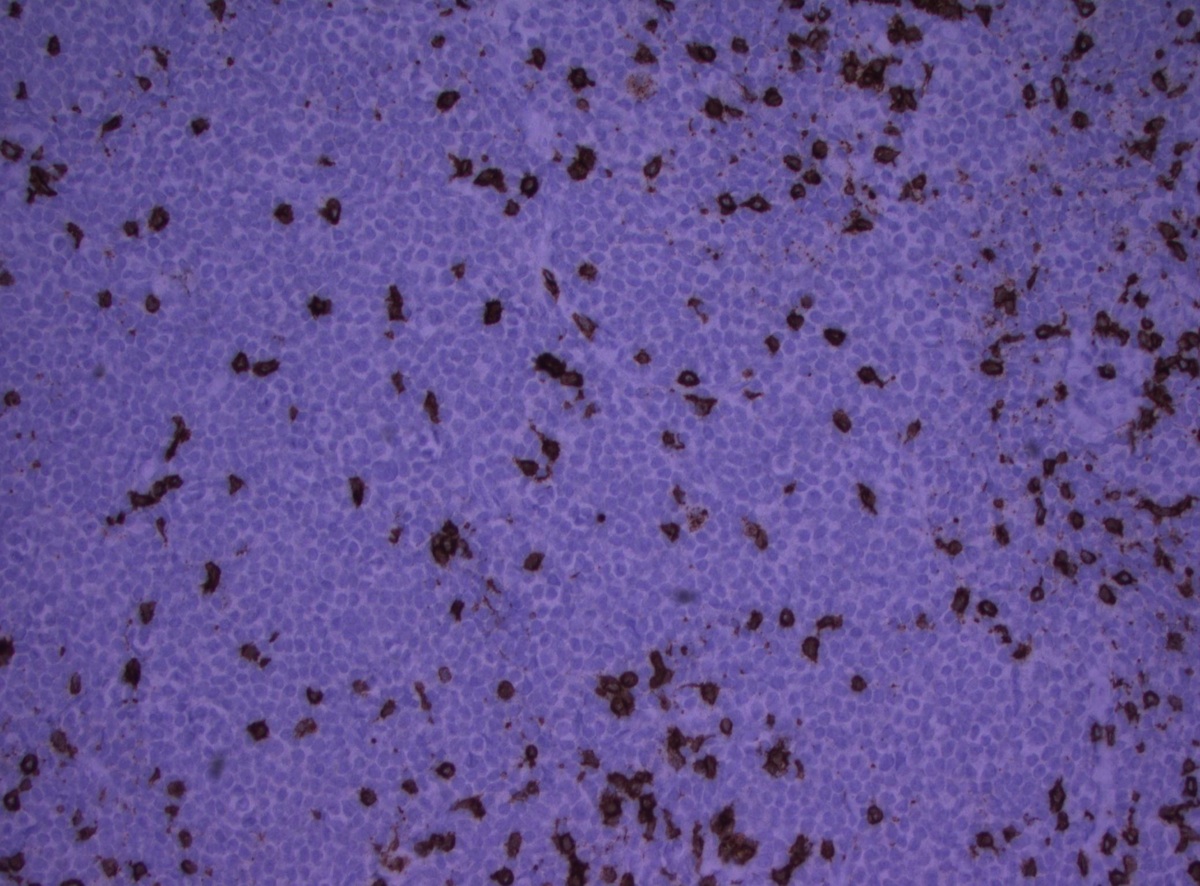
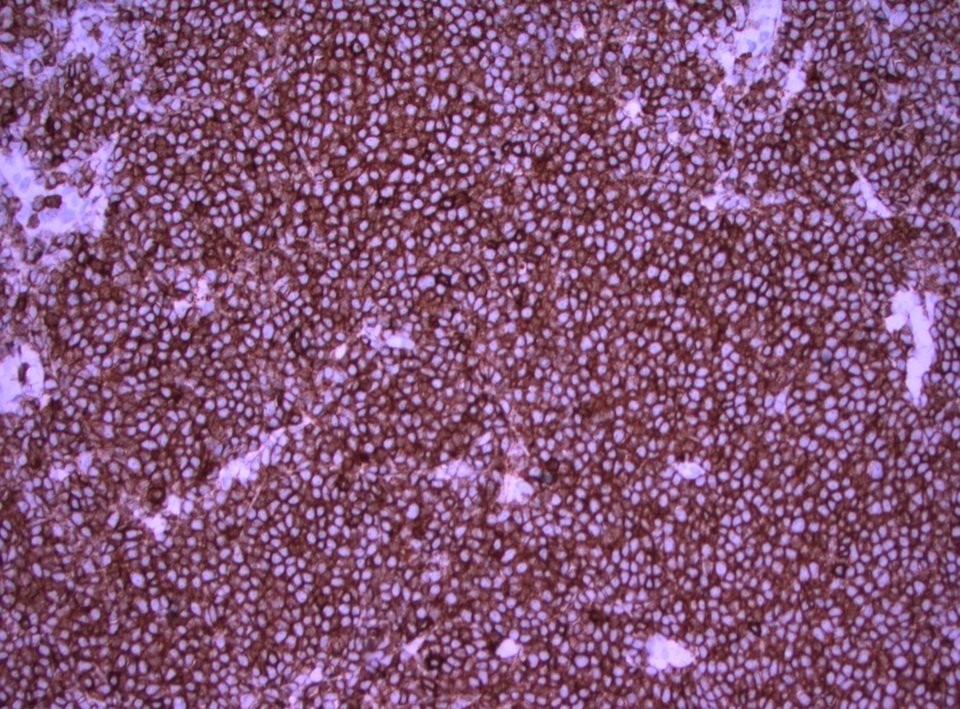
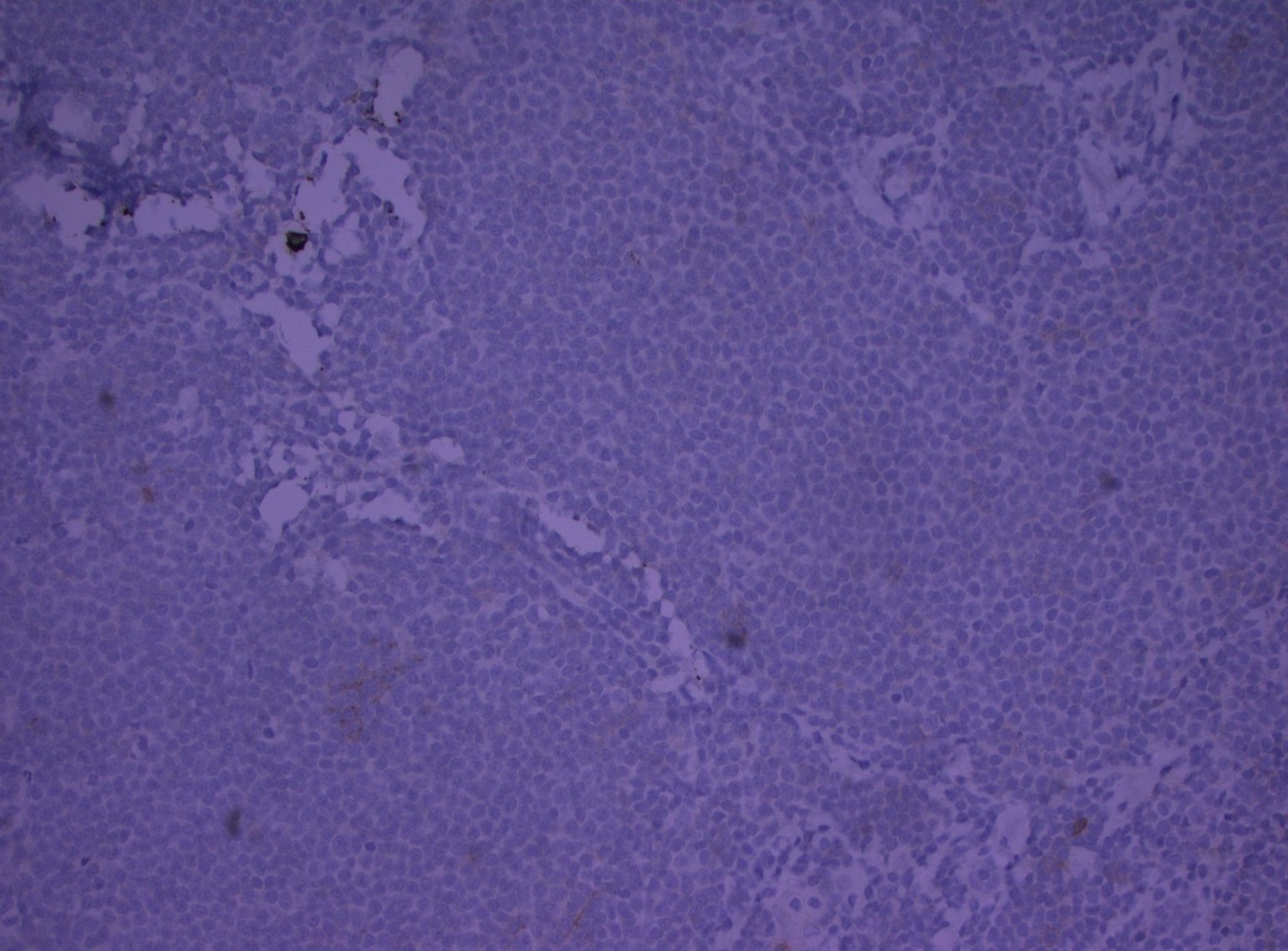
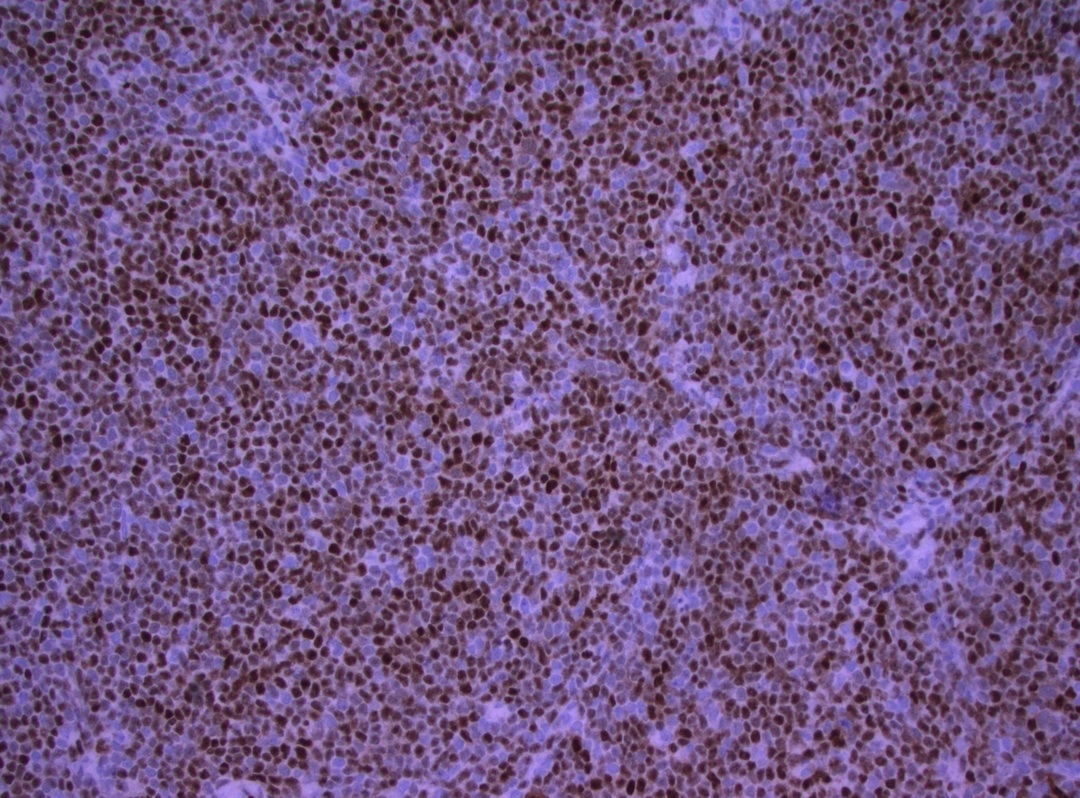
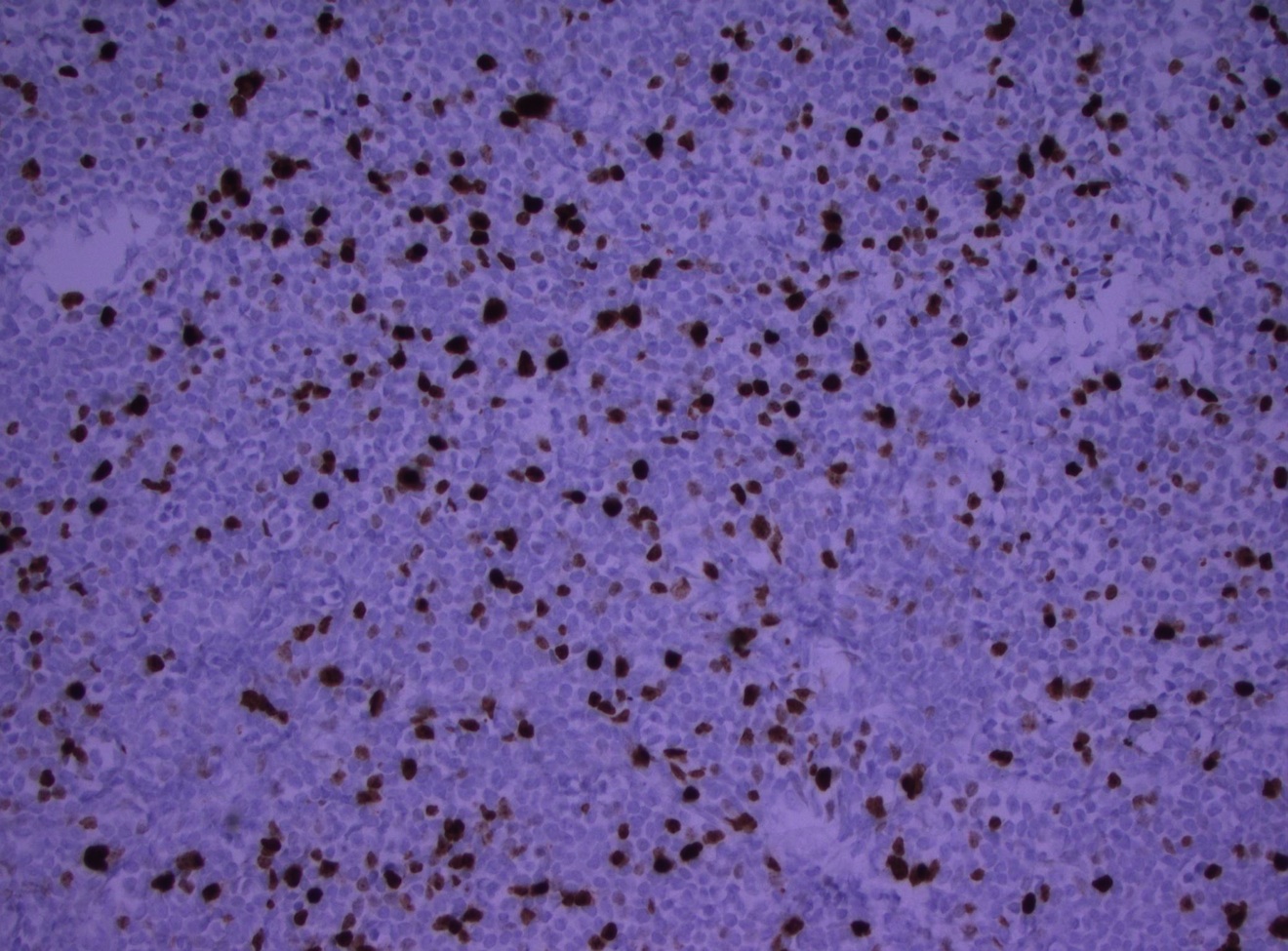
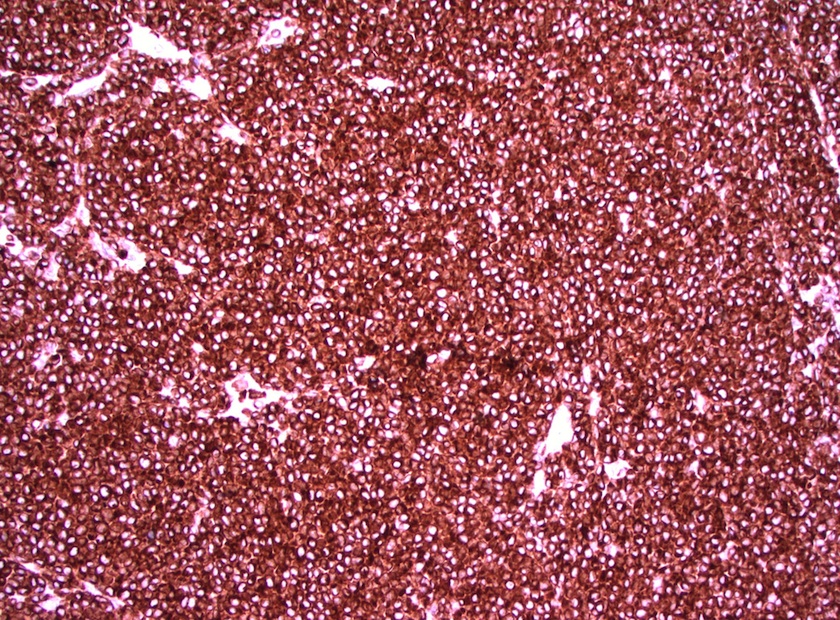
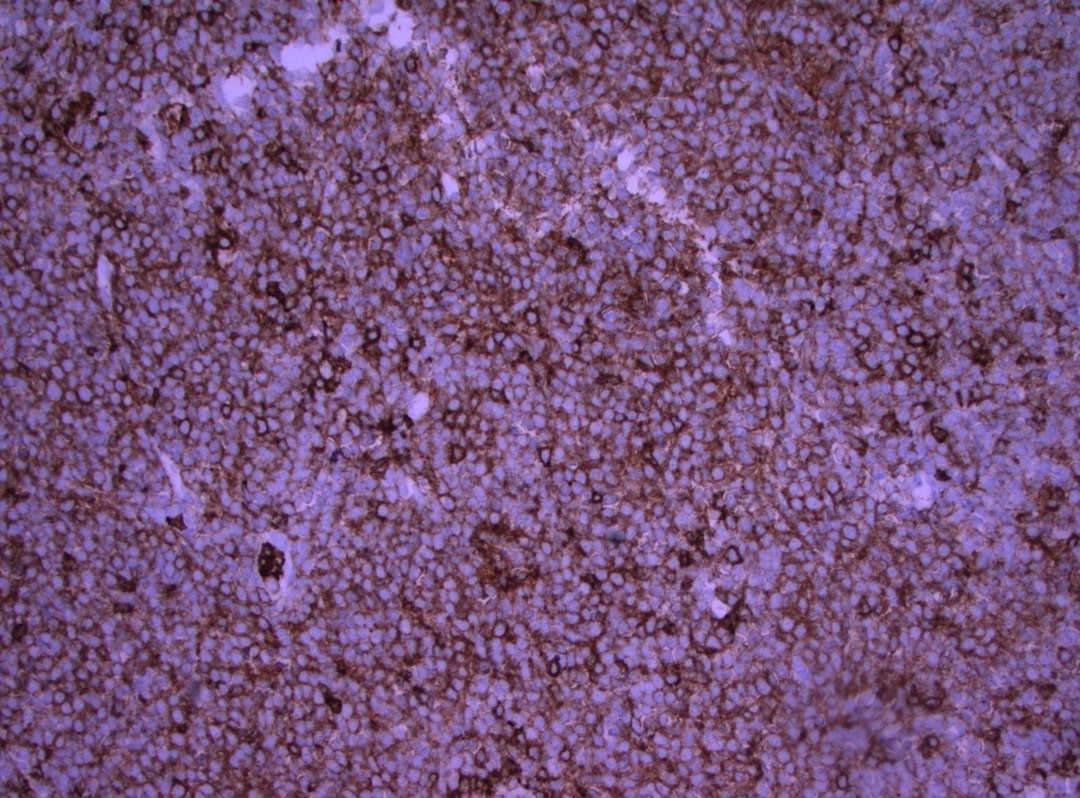
Immunostains:
Left to right: CD20+, CD3- (T cells are CD3+), CD5+
Left to right: CD23-, cyclinD1+, Ki67+
Left to right: bcl2+, CD43+
Discussion:
The H&E stained sections show sheets of an atypical lymphoid infiltrate with occasional hyalinized small vessels in the background. The tumor cells are monomorphic, small mature lymphocytes with scant cytoplasm, round to oval, cleaved nuclei, dense chromatin and inconspicuous nucleoli. No mitotic figures were seen. Flow cytometry (not shown) revealed monoclonal B cells with lambda light chain restriction, which coexpress CD19 and CD5. These cells were also positive for CD20 (bright) and FMC7, and are negative for CD23, CD10 and CD11c. Immunostains demonstrated that the neoplastic cells were B cells (CD20+, PAX5+) with coexpression of BCL2, CD5, CD43 and cyclin D1, and they were negative for AE1 / AE3, CD3, CD10, CD23 and CD30. The cell proliferation index marker Ki67 was 20 - 30%, confirming a relatively low grade process. Conventional cytogenetics analysis showed 46, XY, t(11;14)(q13;q32).
Ocular lymphomas can be primary or secondary, and occur in the orbit, conjunctiva and eyelids. Most lymphomas in the ocular adnexa are B cell non-Hodgkin lymphomas, most commonly extranodal marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALToma). Less common B cell subtypes include lymphoplasmacytic lymphoma, mantle cell lymphoma, plasmacytoma and follicular lymphoma. At all sites, mantle cell lymphoma (MCL) represents 3 - 5% of non-Hodgkin lymphomas. It predominantly occurs in older ages with a higher frequency in men, usually presenting with widespread disease and an aggressive course. Mantle cell lymphoma most commonly occurs in lymph nodes and in the GI tract but it presents as secondary involvement of ocular adnexal structures in 6% of the ocular lymphomas. There are limited studies of primary ocular mantle cell lymphoma.
References: Arch Ophthalmol 2007;125:1668, Br J Ophthalmol 2009;93:1047, Semin Diagn Pathol 2011;28:245
