
24 July 2013 - Case #280
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Hanni Gulwani, Bhopal Memorial Hospital and Research Centre (India), for contributing this case and the discussion.
Advertisement
Case #280
Clinical history:
A 15 year old girl presented with left hip pain for a few months. CT scan showed a well circumscribed mass of the left sacroiliac bone with no soft tissue invasion.
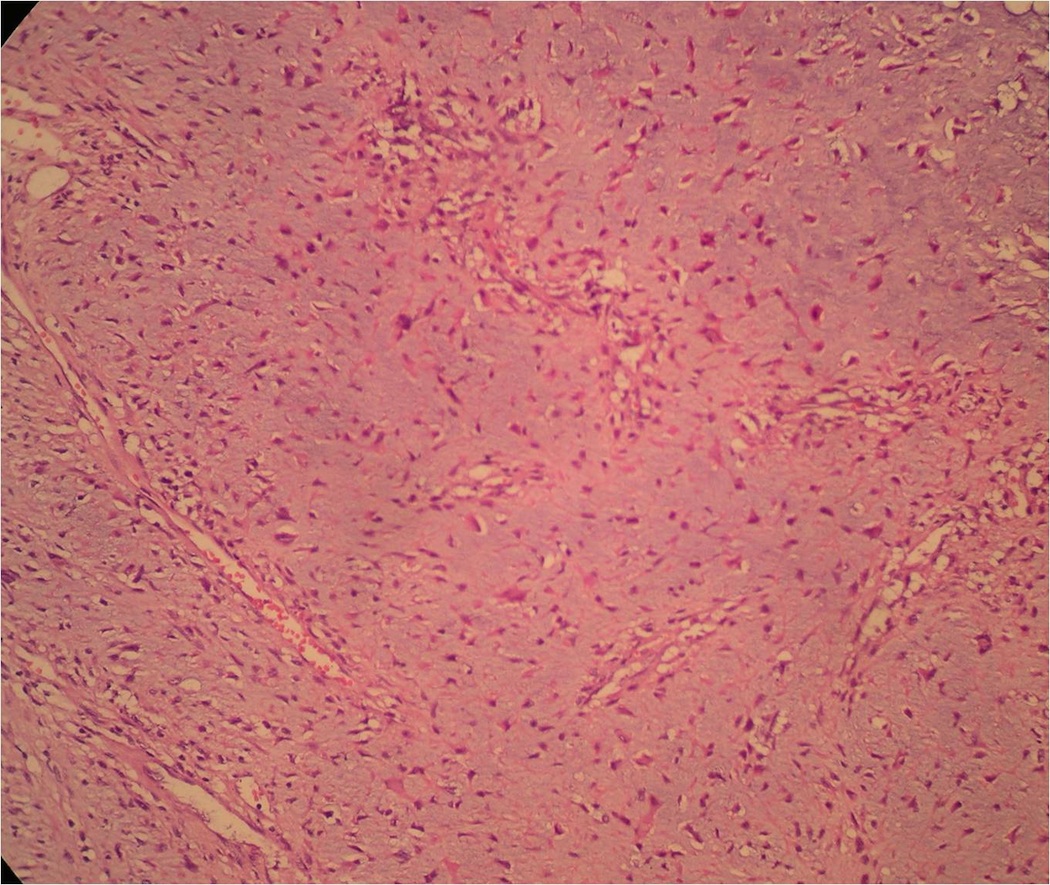
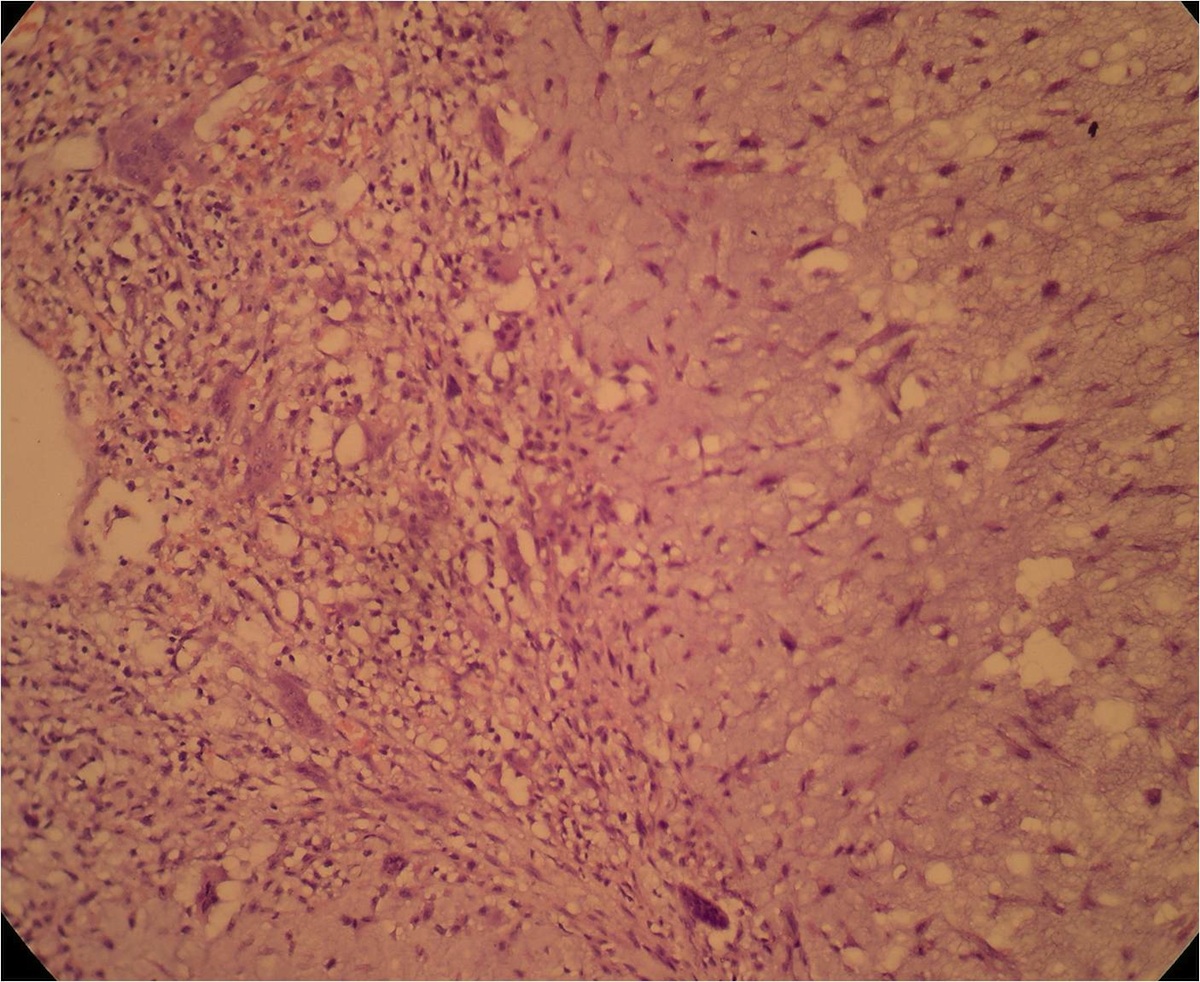
Microscopic images:
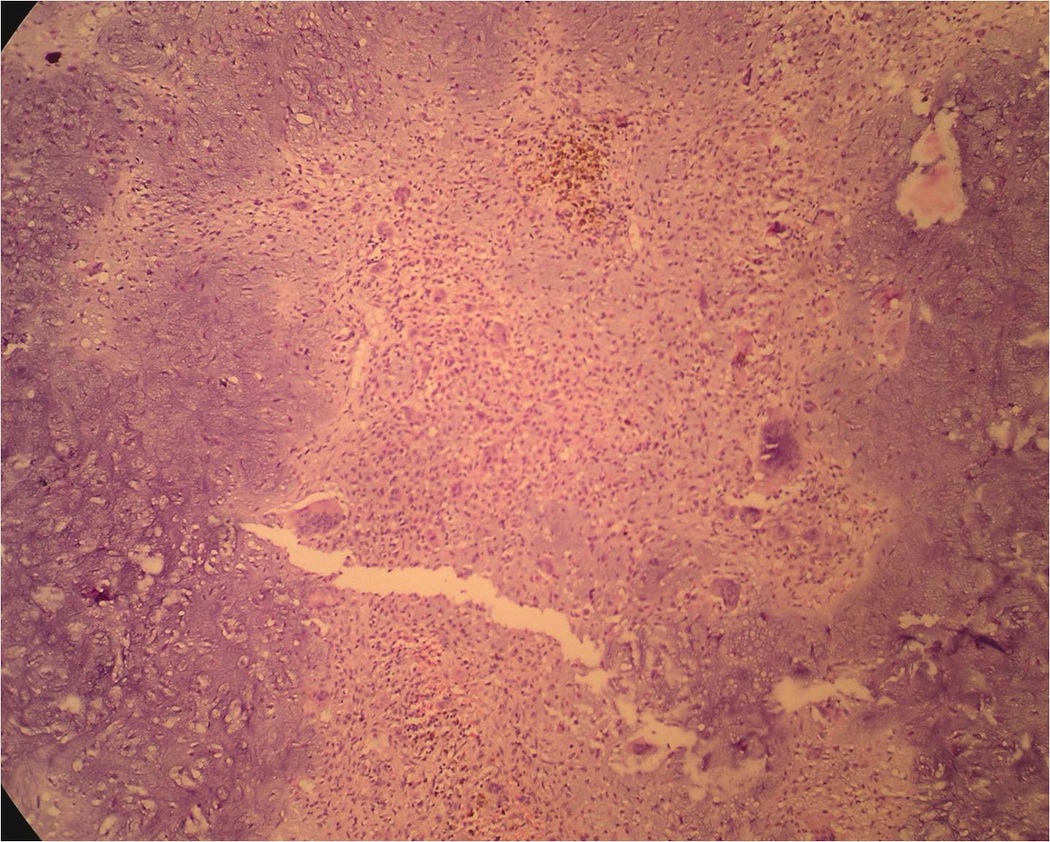
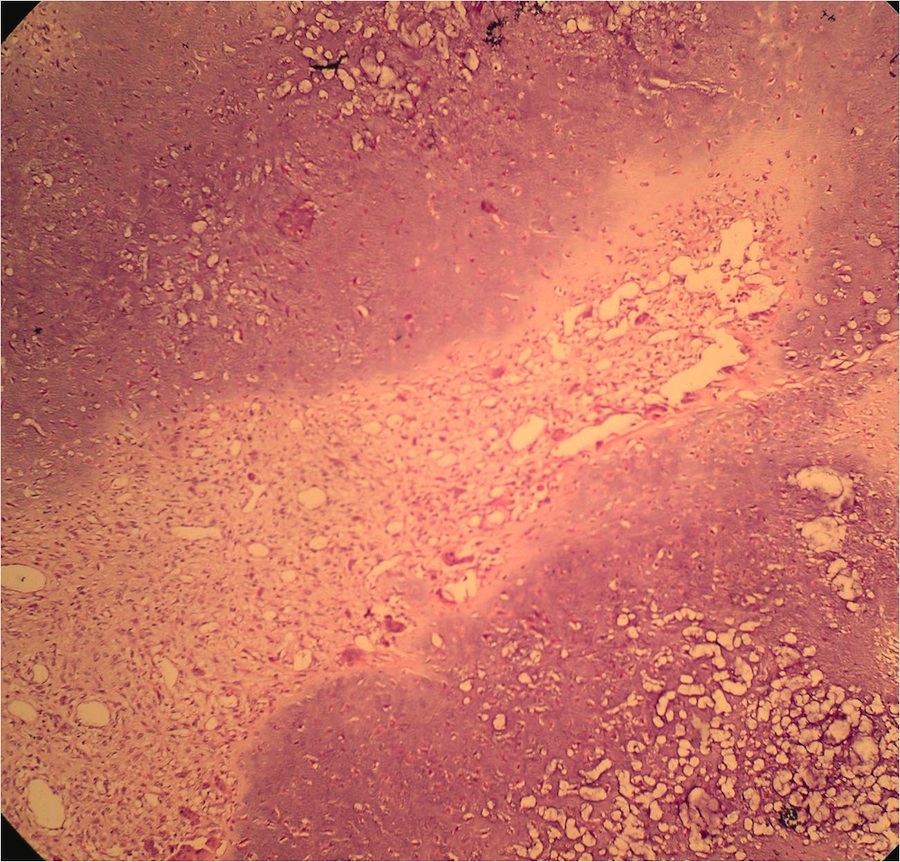
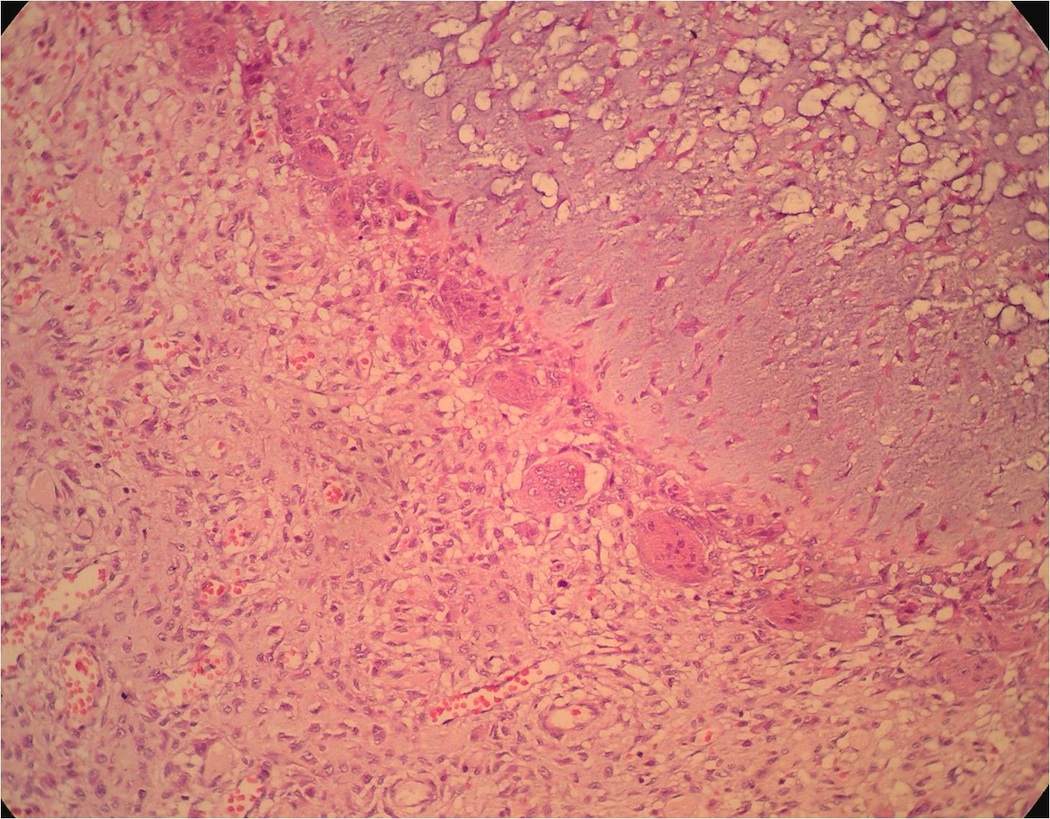
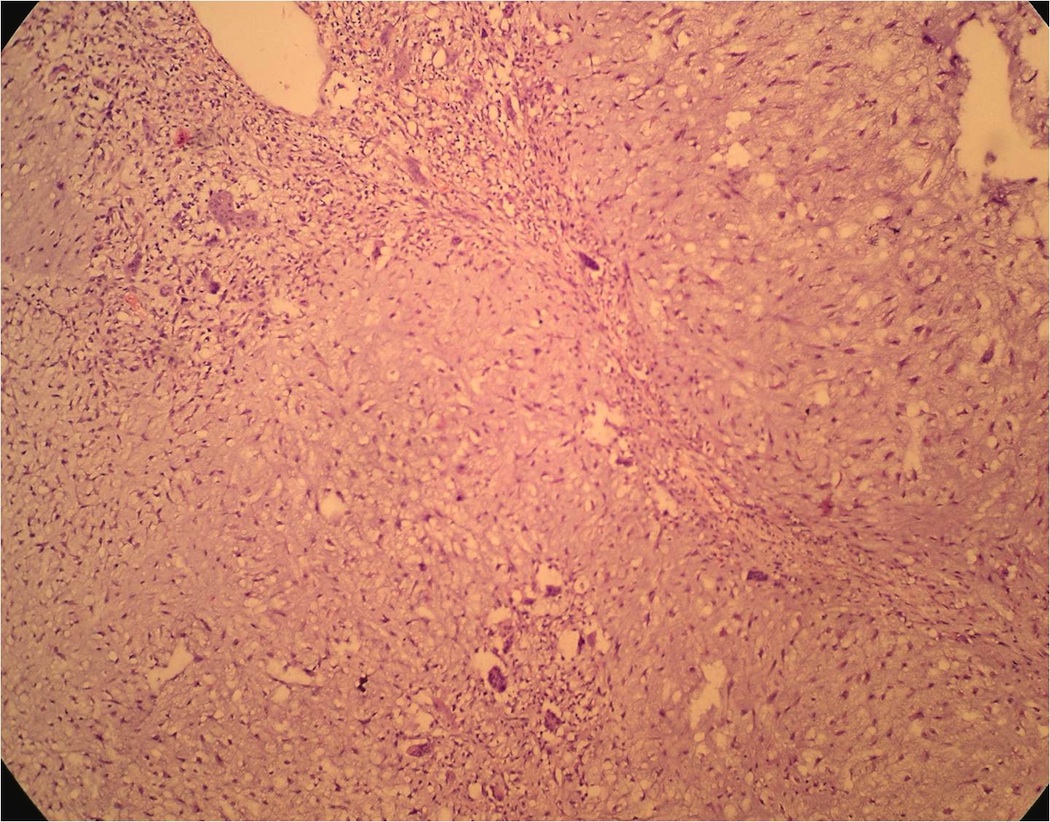

What is your diagnosis?
Diagnosis: Chondromyxoid fibroma
Discussion:
Chondromyxoid fibroma is a rare benign cartilaginous bone tumor arising in young adults aged 15 - 25 years (Hum Pathol 2010;41:208). It presents with a dull, achy pain and often occurs in the metaphysis of long tubular bones or in the small bones of the feet. Radiographs show an extremely well circumscribed lytic defect with a scalloped, sclerotic margin similar to metaphyseal fibrous defect.
At gross exam, the tumor is 3 - 8 cm, well circumscribed, solid and glistening. It is often lobulated with zonation. Older tumors are more hyalinized. Microscopic examination reveals well circumscribed, hypocellular lobules of poorly formed hyaline cartilage composed of chondroblasts with abundant pink cytoplasm and myxoid tissue with fibrous septae containing spindle cells and osteoclasts. Atypia is common, including large, hyperchromatic nuclei. Scattered calcification and osteoclast-like giant cells are present. At the periphery, the tumor is more cellular and vascular (Mod Pathol 1999;12:514). There is no / rare mitotic activity. Tumors often have 6q13 rearrangements, with recurrent 6p25 and 6q25 anomalies (Mod Pathol 2009;22:1499).
The differential diagnosis includes:
Chondromyxoid fibroma is benign, although 25% recur after curettage. They may erode through the bone cortex but there are no distant metastases.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Hanni Gulwani, Bhopal Memorial Hospital and Research Centre (India), for contributing this case and the discussion.
Wayne State University
Karmanos Cancer Center
Detroit Medical Center
Present the 10th Annual Conference
Contemporary Issues in Diagnostic Pathology
Program Director: Rouba Ali-Fehmi, MD

November 2, 2013
The Henry, Autograph Collection
Dearborn, Michigan (USA)
For more information: https://pathology.med.wayne.edu
Website news:
(1) We have recently updated these topics in our Stains and CD Markers chapters: arginase1, beta-catenin, CCR9, CD25, cathepsin K and CDK4. If you are interested in reviewing a topic in these chapters, please take a look at our new Stains in Review page to see how you can contribute.
(2) As you know, PathologyOutlines.com has always been a free resource for you and your fellow pathologists. The companies and institutions that post Jobs, Fellowships and Conferences, and that sponsor the website with various Banners and Buyer's Guide listings, help us to continue providing free, comprehensive, and up-to-date content. Please remember to thank our advertisers and let them know that you saw them on PathologyOutlines.com.
Visit and follow our Blog to see recent updates to the website.
(1) We have recently updated these topics in our Stains and CD Markers chapters: arginase1, beta-catenin, CCR9, CD25, cathepsin K and CDK4. If you are interested in reviewing a topic in these chapters, please take a look at our new Stains in Review page to see how you can contribute.
(2) As you know, PathologyOutlines.com has always been a free resource for you and your fellow pathologists. The companies and institutions that post Jobs, Fellowships and Conferences, and that sponsor the website with various Banners and Buyer's Guide listings, help us to continue providing free, comprehensive, and up-to-date content. Please remember to thank our advertisers and let them know that you saw them on PathologyOutlines.com.
Visit and follow our Blog to see recent updates to the website.
Case #280
Clinical history:
A 15 year old girl presented with left hip pain for a few months. CT scan showed a well circumscribed mass of the left sacroiliac bone with no soft tissue invasion.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Chondromyxoid fibroma
Discussion:
Chondromyxoid fibroma is a rare benign cartilaginous bone tumor arising in young adults aged 15 - 25 years (Hum Pathol 2010;41:208). It presents with a dull, achy pain and often occurs in the metaphysis of long tubular bones or in the small bones of the feet. Radiographs show an extremely well circumscribed lytic defect with a scalloped, sclerotic margin similar to metaphyseal fibrous defect.
At gross exam, the tumor is 3 - 8 cm, well circumscribed, solid and glistening. It is often lobulated with zonation. Older tumors are more hyalinized. Microscopic examination reveals well circumscribed, hypocellular lobules of poorly formed hyaline cartilage composed of chondroblasts with abundant pink cytoplasm and myxoid tissue with fibrous septae containing spindle cells and osteoclasts. Atypia is common, including large, hyperchromatic nuclei. Scattered calcification and osteoclast-like giant cells are present. At the periphery, the tumor is more cellular and vascular (Mod Pathol 1999;12:514). There is no / rare mitotic activity. Tumors often have 6q13 rearrangements, with recurrent 6p25 and 6q25 anomalies (Mod Pathol 2009;22:1499).
The differential diagnosis includes:
- Chondroblastoma:
- Usually epiphysis (open) or apophysis; compact polyhedral chondroblasts with well defined cell borders, abundant pink cytoplasm, hyperlobulated nuclei with grooves in mineralized, chicken wire matrix that surrounds chondroblasts
- May be a related entity, since both have similar expression profile for skeletal development markers (Mod Pathol 2012;25:1452)
- Chondrosarcoma:
- Similar histology but malignant radiologically, no hypocellular center, infiltrates surrounding tissue
- Fibromyxoma:
- Usually older adults, no cartilaginous areas
- Fibrous dysplasia with myxoid change:
- Curvilinear trabeculae (Chinese letters) of metaplastic woven bone in hypocellular fibroblastic stroma
- Not lobulated
Chondromyxoid fibroma is benign, although 25% recur after curettage. They may erode through the bone cortex but there are no distant metastases.
