
11 July 2013 - Case #278
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Vaidehi Avadhani, St. Luke's Roosevelt Hospital, New York (USA), for contributing this case and the discussion.
Advertisement
Case #278
Clinical history:
A 62 year old man with COPD and myelofibrosis presented with shortness of breath. Chest CT showed an anterior mediastinal mass, accompanied by enlarged regional lymph nodes. The mass was excised, and a lymph node dissection was performed.
Gross examination revealed a 3.2 cm nodular mass with a tan white cut surface.
Microscopic images:

What is your diagnosis?
Diagnosis: Well differentiated neuroendocrine carcinoma / atypical carcinoid of the thymus gland
Immunostains:

Discussion:
The tumor infiltrates into adjacent adipose tissue. Metastatic carcinoma was identified in 2 of 3 lymph nodes.
According to the World Health Organization (WHO), thymic epithelial tumors with predominant neuroendocrine differentiation are classified as neuroendocrine carcinomas (NEC) of the thymus (IARC: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart, 1st Edition, 2004). Thymic neuroendocrine carcinomas are classified as well differentiated NEC and poorly differentiated NEC.
Classification
A. Well differentiated NEC
a. Typical carcinoid: no necrosis and <2 mitoses per 2 mm2 (10 hpf)
b. Atypical carcinoid: necrosis present and 2-10 mitoses per 2 mm2(10 hpf)
B. Poorly differentiated NEC:
a. Large cell NEC: non-small cell NEC with > 10 mitoses per 10 hpf
b. Small cell NEC: small cell cytology
Neuroendocrine differentiation can be demonstrated by immunohistochemistry (synaptophysin, chromogranin and CD56 positive) or by identification of neurosecretory granules by electron microscopy.
The main differential diagnosis includes:
Tumor stage has been found to be an important prognostic factor. Due to the rarity of the tumor, well defined guidelines for management are not yet published. However, most studies show that atypical carcinoids of the thymus are aggressive (Semin Diagn Pathol 2005;22:223, Korean J Pathol 2012;46:221). Radical resection of the primary tumor with local lymph nodes is the standard of care.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Vaidehi Avadhani, St. Luke's Roosevelt Hospital, New York (USA), for contributing this case and the discussion.
December 7, 2013
The Inn at St. John's
Plymouth, Michigan (USA)
Michigan Society of Pathologists
2013 Winter Conference

Website
Hotel
Register
Website news:
(1) As you know, PathologyOutlines.com has always been a free resource for you and your fellow pathologists. The companies and institutions that post Jobs, Fellowships and Conferences, and that sponsor the website with various Banners and Buyer's Guide listings, help us to continue providing free, comprehensive, and up-to-date content. If you use our website to find products and services or Jobs, Conferences and Fellowships, please remember to thank our advertisers and let them know that you saw them on PathologyOutlines.com.
(2) We have updated our popular Soft tissue chapter based on reviews by the following Reviewers and Editors: Komal Arora, M.D., Ali Chaudhri, M.D., Jerad Gardner, M.D., Raul Gonzalez, M.D., Ashley Gullett, M.D., Christine E. Jabcuga, M.D., David Lucas, M.D., Ricardo M. Mendoza, M.D., Annie S. Morrison, M.D., Deepti Reddi, M.D., Vijay Shankar, M.D., Lauren N. Stuart M.D., M.B.A., Cliff Sullivan, M.D., Meggen Walsh, M.D., Daniel Wimmer, D.O.
(3) On 25 June 2013, we had record traffic of 17,210 visits (378,692 "hits"). In June 2013, we had record average traffic of 13,320 visits. Thanks for your support!
(4) Our Feature Page for July highlights Imaging / Digital / Photography and includes Celestron, Leica Microsystems, Milestone Medical, Optronics, and Photodyne Technologies.
(5) Here is how to cite PathologyOutlines.com as a reference, according to the MLA:
Author/Reviewer Last Name, Author/Reviewer First Name, Degrees. "Page Title." Website title. Publisher, Date published, Web. Date viewed.
For example, Bone - Osteoblastoma, would be cited like this:
Lucas, David, MD. "Bone - Osteoblastoma." PathologyOutlines.com. PathologyOutlines.com, 14 March 2013. Web. 18 June 2013.
Visit and follow our Blog to see recent updates to the website.
(1) As you know, PathologyOutlines.com has always been a free resource for you and your fellow pathologists. The companies and institutions that post Jobs, Fellowships and Conferences, and that sponsor the website with various Banners and Buyer's Guide listings, help us to continue providing free, comprehensive, and up-to-date content. If you use our website to find products and services or Jobs, Conferences and Fellowships, please remember to thank our advertisers and let them know that you saw them on PathologyOutlines.com.
(2) We have updated our popular Soft tissue chapter based on reviews by the following Reviewers and Editors: Komal Arora, M.D., Ali Chaudhri, M.D., Jerad Gardner, M.D., Raul Gonzalez, M.D., Ashley Gullett, M.D., Christine E. Jabcuga, M.D., David Lucas, M.D., Ricardo M. Mendoza, M.D., Annie S. Morrison, M.D., Deepti Reddi, M.D., Vijay Shankar, M.D., Lauren N. Stuart M.D., M.B.A., Cliff Sullivan, M.D., Meggen Walsh, M.D., Daniel Wimmer, D.O.
(3) On 25 June 2013, we had record traffic of 17,210 visits (378,692 "hits"). In June 2013, we had record average traffic of 13,320 visits. Thanks for your support!
(4) Our Feature Page for July highlights Imaging / Digital / Photography and includes Celestron, Leica Microsystems, Milestone Medical, Optronics, and Photodyne Technologies.
(5) Here is how to cite PathologyOutlines.com as a reference, according to the MLA:
Author/Reviewer Last Name, Author/Reviewer First Name, Degrees. "Page Title." Website title. Publisher, Date published, Web. Date viewed.
For example, Bone - Osteoblastoma, would be cited like this:
Lucas, David, MD. "Bone - Osteoblastoma." PathologyOutlines.com. PathologyOutlines.com, 14 March 2013. Web. 18 June 2013.
Visit and follow our Blog to see recent updates to the website.
Case #278
Clinical history:
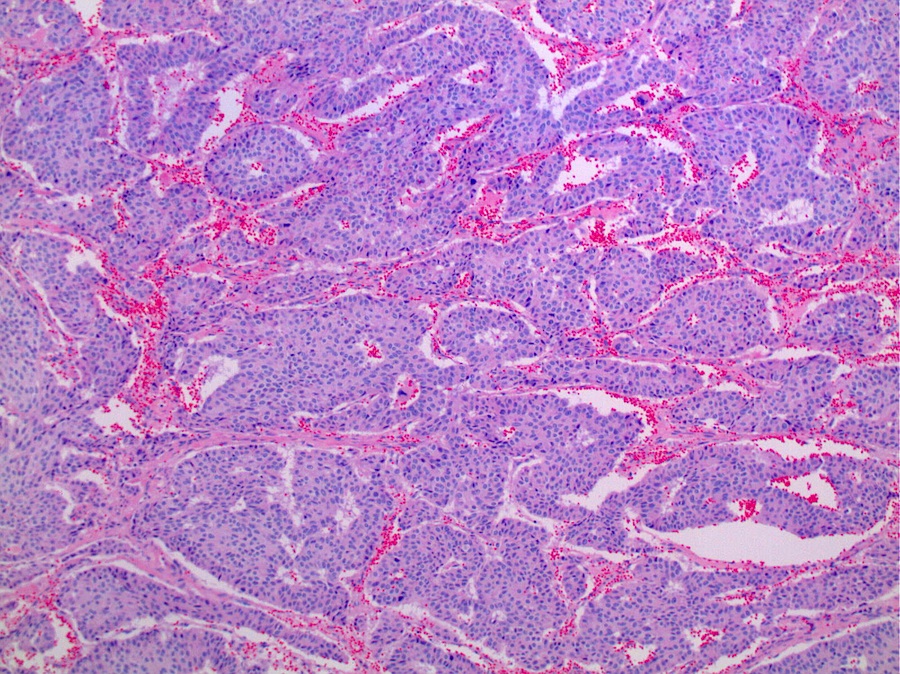
A 62 year old man with COPD and myelofibrosis presented with shortness of breath. Chest CT showed an anterior mediastinal mass, accompanied by enlarged regional lymph nodes. The mass was excised, and a lymph node dissection was performed.
Gross examination revealed a 3.2 cm nodular mass with a tan white cut surface.
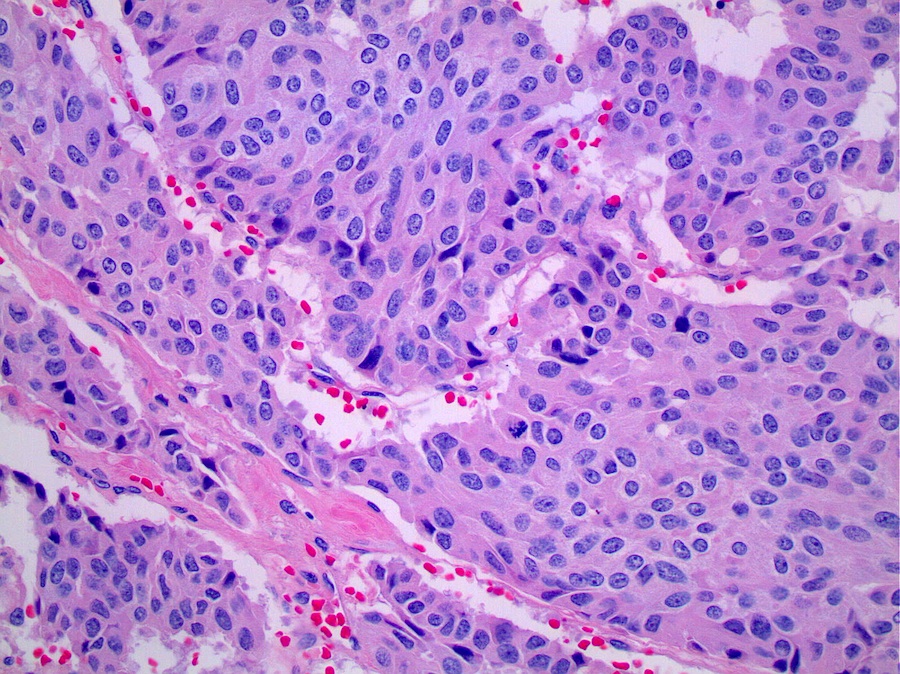
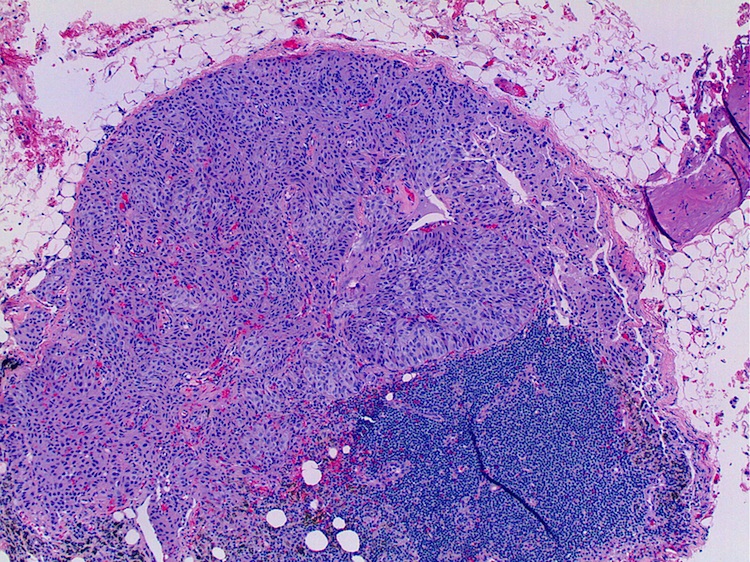
Microscopic images:
From mass
From regional lymph node
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Well differentiated neuroendocrine carcinoma / atypical carcinoid of the thymus gland
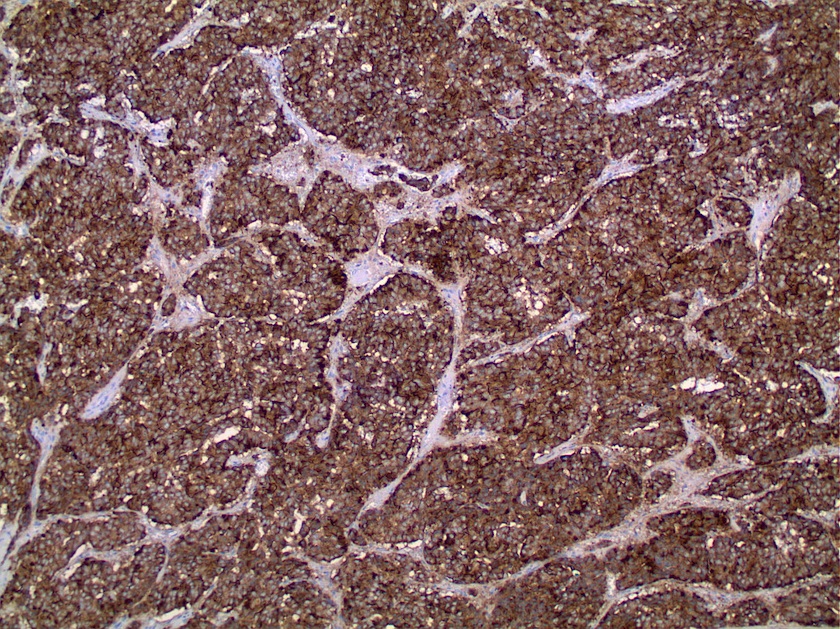
Immunostains:
Left: AE1 / AE3, right: synaptophysin
Discussion:
The tumor infiltrates into adjacent adipose tissue. Metastatic carcinoma was identified in 2 of 3 lymph nodes.
According to the World Health Organization (WHO), thymic epithelial tumors with predominant neuroendocrine differentiation are classified as neuroendocrine carcinomas (NEC) of the thymus (IARC: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart, 1st Edition, 2004). Thymic neuroendocrine carcinomas are classified as well differentiated NEC and poorly differentiated NEC.
Classification
A. Well differentiated NEC
a. Typical carcinoid: no necrosis and <2 mitoses per 2 mm2 (10 hpf)
b. Atypical carcinoid: necrosis present and 2-10 mitoses per 2 mm2(10 hpf)
B. Poorly differentiated NEC:
a. Large cell NEC: non-small cell NEC with > 10 mitoses per 10 hpf
b. Small cell NEC: small cell cytology
Neuroendocrine differentiation can be demonstrated by immunohistochemistry (synaptophysin, chromogranin and CD56 positive) or by identification of neurosecretory granules by electron microscopy.
The main differential diagnosis includes:
- Metastatic pulmonary NEC: (TTF1+ may be helpful) (Mod Pathol 2013;26:1554)
- Thymic carcinoma with focal neuroendocrine differentiation
- Nerve sheath tumor: cytokeratin-, chromogranin-, synaptophysin-
- Paraganglioma: cytokeratin-
Tumor stage has been found to be an important prognostic factor. Due to the rarity of the tumor, well defined guidelines for management are not yet published. However, most studies show that atypical carcinoids of the thymus are aggressive (Semin Diagn Pathol 2005;22:223, Korean J Pathol 2012;46:221). Radical resection of the primary tumor with local lymph nodes is the standard of care.
