
8 May 2013 - Case #272
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jordan Roberts, Texas (USA) for contributing this case.
Advertisement
Case #272
Clinical history:
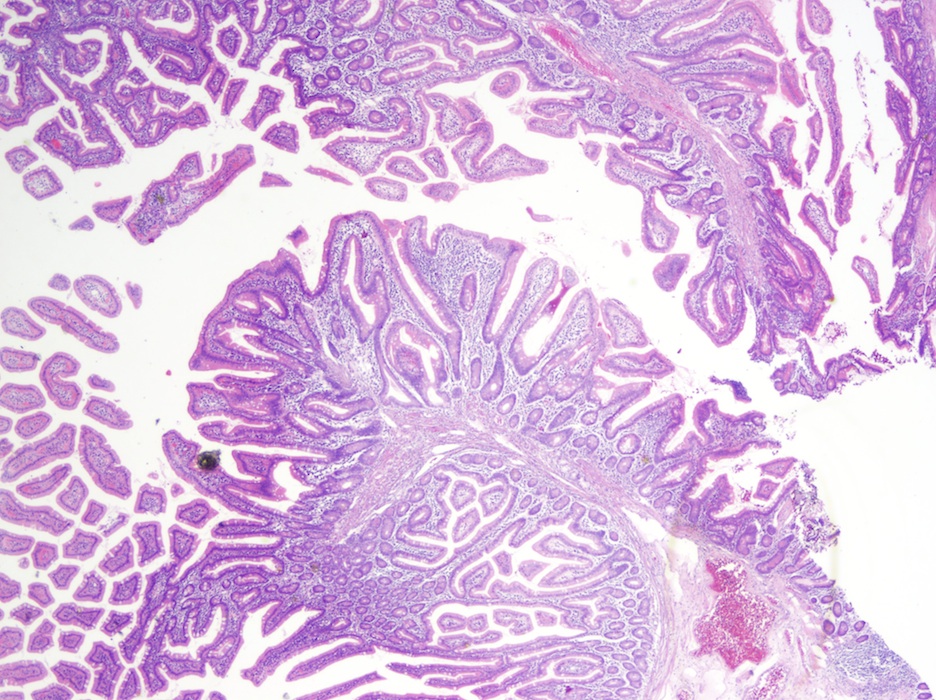
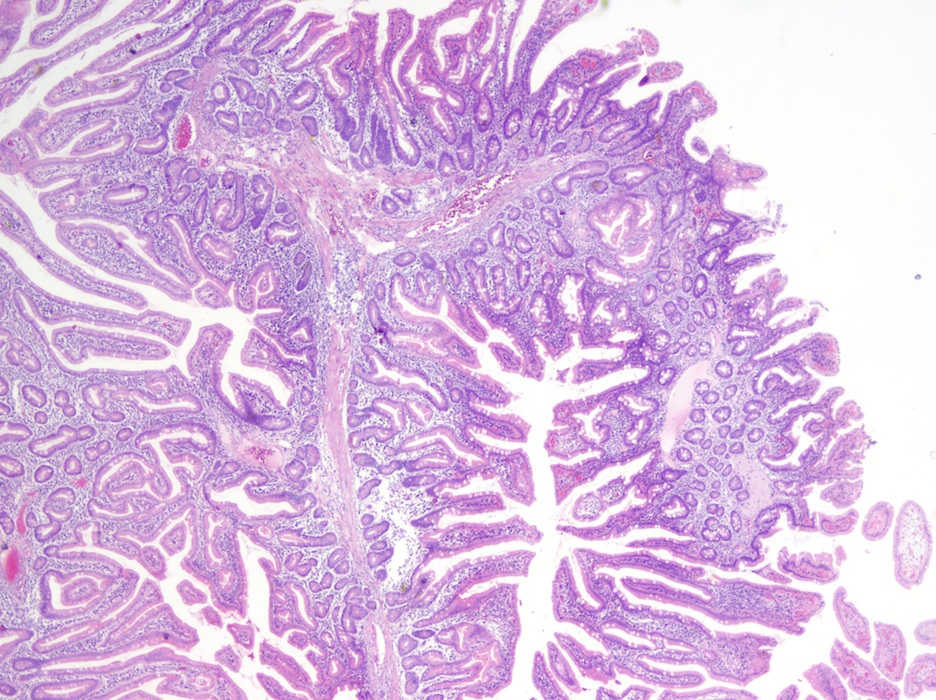
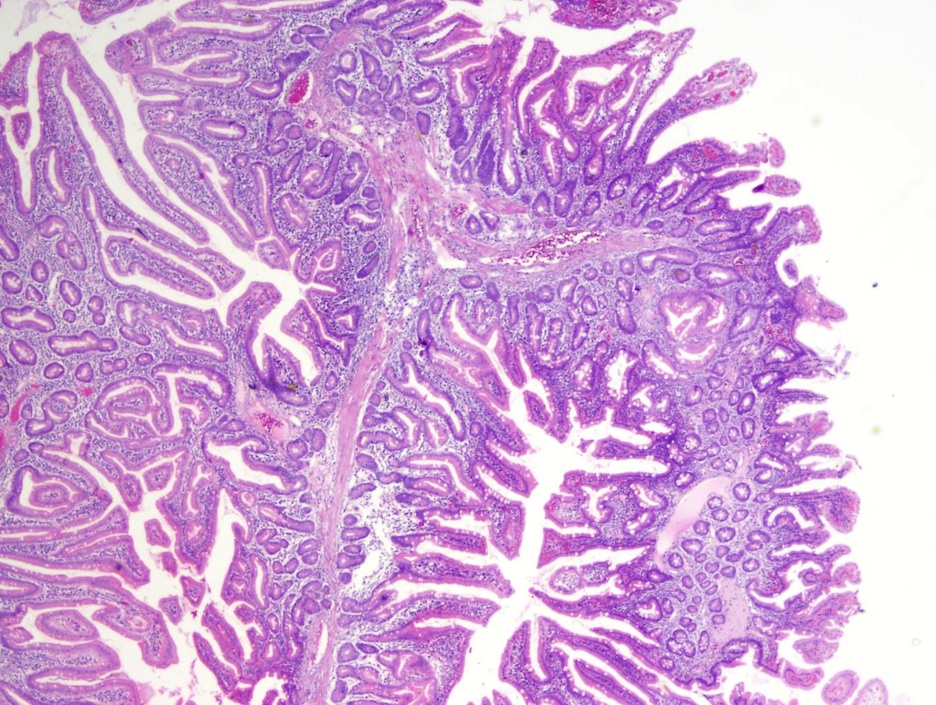
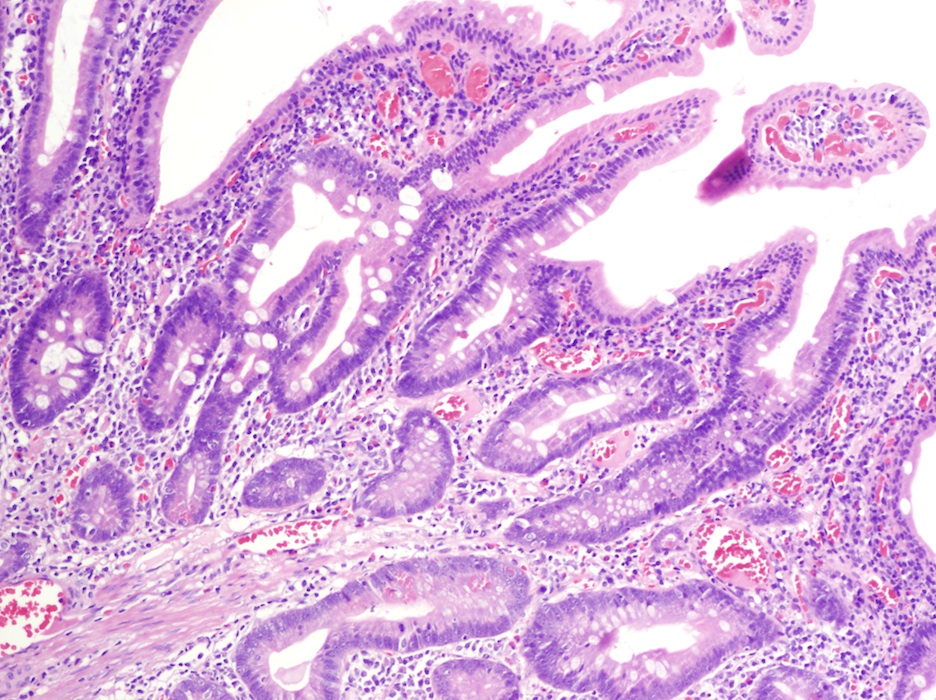
A 50 year old man had multiple polyps in the jejunum, which were biopsied.
Clinical images:

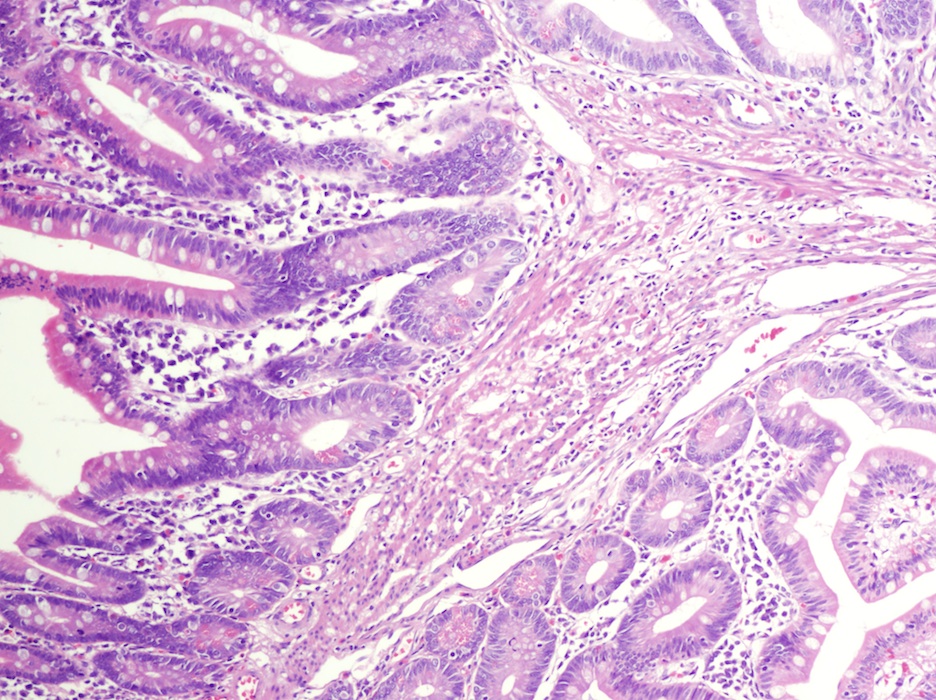
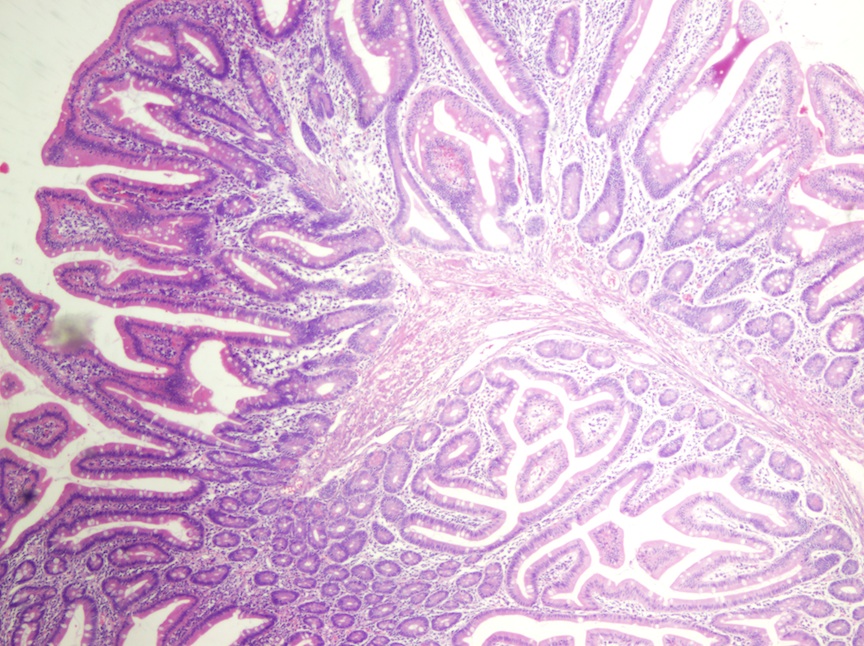
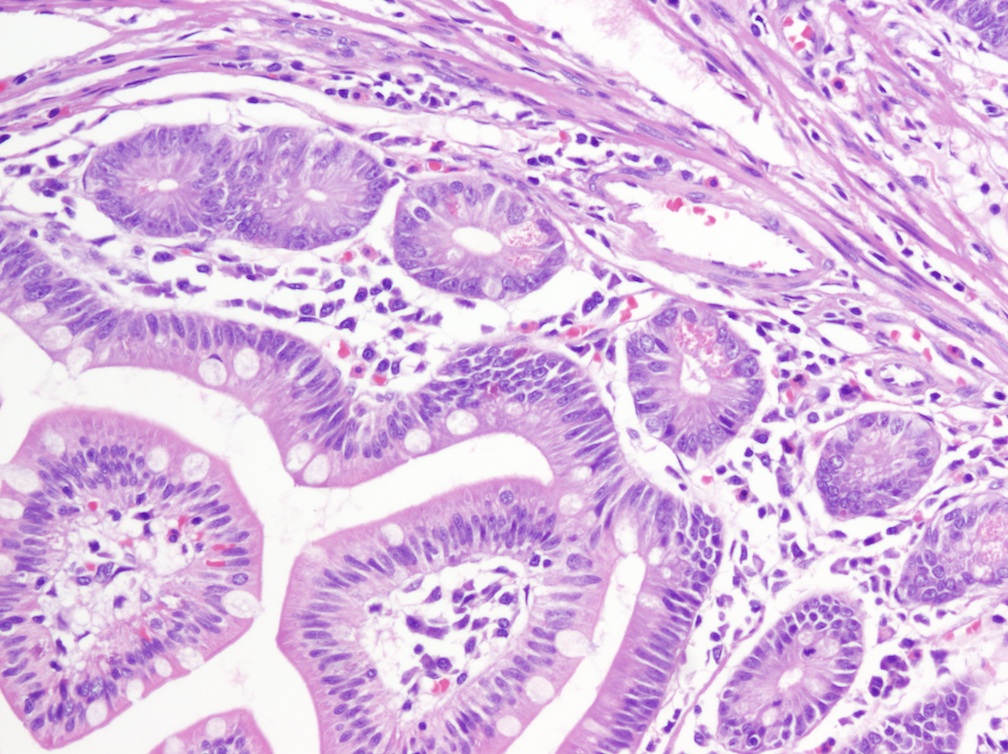
Microscopic images:


What is your diagnosis?
Diagnosis: Hamartomatous (Peutz-Jeghers) polyp
Discussion:
Peutz-Jeghers polyps (hamartomatous polyps) are supported by broad bands of muscularis mucosa smooth muscle, which is thicker centrally, and resembles a Christmas tree at low power. The polyp has superficial columnar and goblet cells, but Paneth and endocrine cells at its base.
Peutz-Jeghers polyps are large, pedunculated polyps of the gut almost always seen in association with Peutz-Jeghers syndrome (Am J Surg Pathol 2007;31:1209). This rare autosomal dominant disorder is usually diagnosed at ages 20 - 30, with hamartomatous polyps in the small bowel (100%), stomach and colon (25%), and associated adenomatous lesions that may give rise to adenocarcinoma of the stomach, large or small bowel; adenoma malignum of the cervix, ovarian mucinous tumors and carcinoma of the breast, lung and pancreas. The syndrome is also associated with sex cord tumor with annular tubules (almost all patients) and melanotic pigmentation of the digits, genitalia, lips, oral mucosa, palms and soles.
Peutz-Jeghers syndrome is caused by mutations in STK11 / LKB1, a novel serine threonine kinase, which may play a role in cell polarity (Nat Genet 1998;18:38, Nature 1998;391:184, Genes Cells 2012;17:737).
The differential diagnosis includes invasive carcinoma, because polypoid epithelial misplacement, present in 10%, may resemble malignancy (Am J Surg Pathol 2000;24:34). Recommended treatment is screening and polypectomy of the entire small bowel, plus lifelong cancer screening of the GI tract, breast, lung, ovaries, pancreas and testis, due to the markedly elevated cancer risk, mainly for pancreatic and cervical cancers (World J Gastroenterol 2009;15:5397, Dig Liver Dis 2013;45:606).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jordan Roberts, Texas (USA) for contributing this case.

For a limited time, Epitomics, an Abcam Company, invites you to evaluate rabbit monoclonal antibodies for FREE.
How does it work?
1) Login or create a new Epitomics account
2) Select up to three EP Clones (0.1 mL size), and well ship them out for your evaluation.
Its that easy! Plus, by evaluating, you can earn discounts on other products.
Click
here to find out more.
Website news:
(1) In April 2013, we again had record traffic, with 384,599 visits and an average daily traffic of 12,819 visits (324,000 hits).
(2) For topics with a large number of images, we have started putting them in a scrolling frame to make the space more efficient. For an example, please view CD31 and let us know what you think.
Visit and follow our Blog to see recent updates to the website.
(1) In April 2013, we again had record traffic, with 384,599 visits and an average daily traffic of 12,819 visits (324,000 hits).
(2) For topics with a large number of images, we have started putting them in a scrolling frame to make the space more efficient. For an example, please view CD31 and let us know what you think.
Visit and follow our Blog to see recent updates to the website.
Case #272
Clinical history:
A 50 year old man had multiple polyps in the jejunum, which were biopsied.
Clinical images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Hamartomatous (Peutz-Jeghers) polyp
Discussion:
Peutz-Jeghers polyps (hamartomatous polyps) are supported by broad bands of muscularis mucosa smooth muscle, which is thicker centrally, and resembles a Christmas tree at low power. The polyp has superficial columnar and goblet cells, but Paneth and endocrine cells at its base.
Peutz-Jeghers polyps are large, pedunculated polyps of the gut almost always seen in association with Peutz-Jeghers syndrome (Am J Surg Pathol 2007;31:1209). This rare autosomal dominant disorder is usually diagnosed at ages 20 - 30, with hamartomatous polyps in the small bowel (100%), stomach and colon (25%), and associated adenomatous lesions that may give rise to adenocarcinoma of the stomach, large or small bowel; adenoma malignum of the cervix, ovarian mucinous tumors and carcinoma of the breast, lung and pancreas. The syndrome is also associated with sex cord tumor with annular tubules (almost all patients) and melanotic pigmentation of the digits, genitalia, lips, oral mucosa, palms and soles.
Peutz-Jeghers syndrome is caused by mutations in STK11 / LKB1, a novel serine threonine kinase, which may play a role in cell polarity (Nat Genet 1998;18:38, Nature 1998;391:184, Genes Cells 2012;17:737).
The differential diagnosis includes invasive carcinoma, because polypoid epithelial misplacement, present in 10%, may resemble malignancy (Am J Surg Pathol 2000;24:34). Recommended treatment is screening and polypectomy of the entire small bowel, plus lifelong cancer screening of the GI tract, breast, lung, ovaries, pancreas and testis, due to the markedly elevated cancer risk, mainly for pancreatic and cervical cancers (World J Gastroenterol 2009;15:5397, Dig Liver Dis 2013;45:606).
