
10 April 2013 - Case #271
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jessica Kozel, University of Nebraska Medical Center, for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case #271
Clinical history:
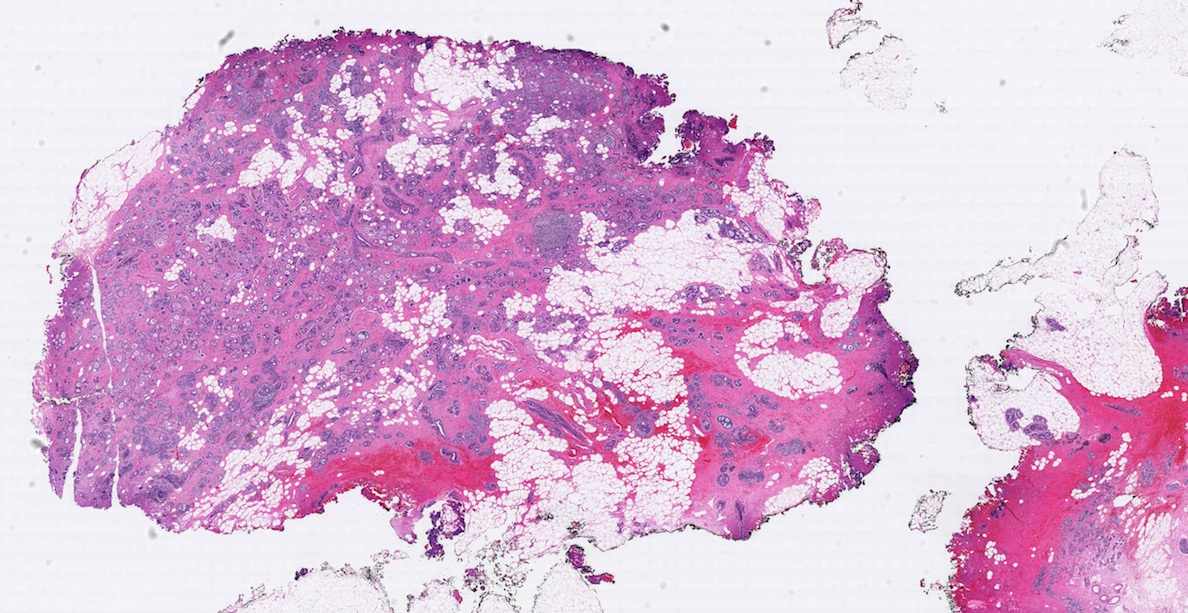
A 61 year old woman presented with a mammographic left breast mass. An incisional biopsy was performed.
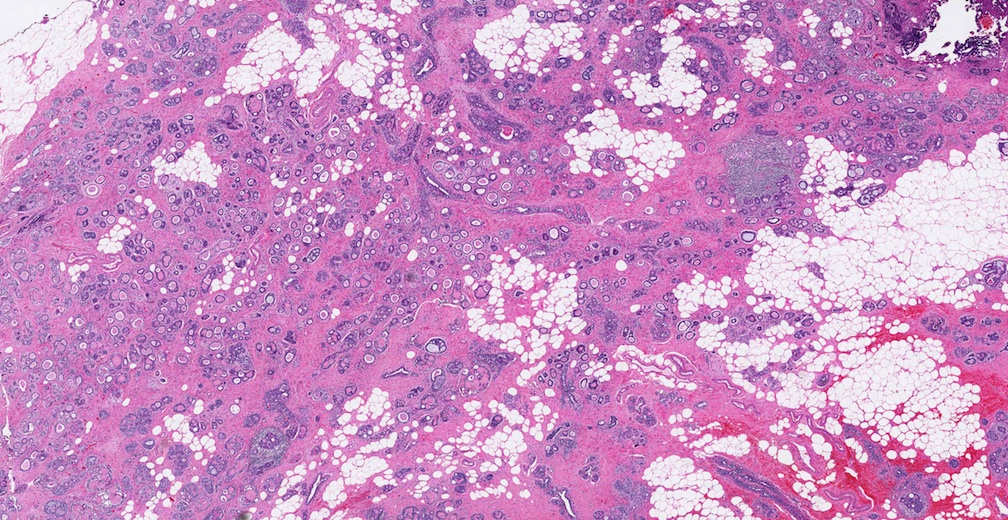
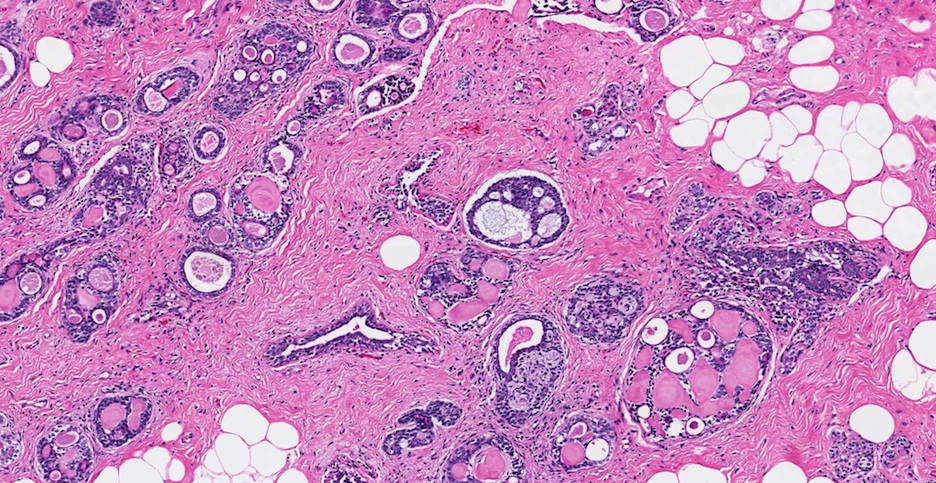
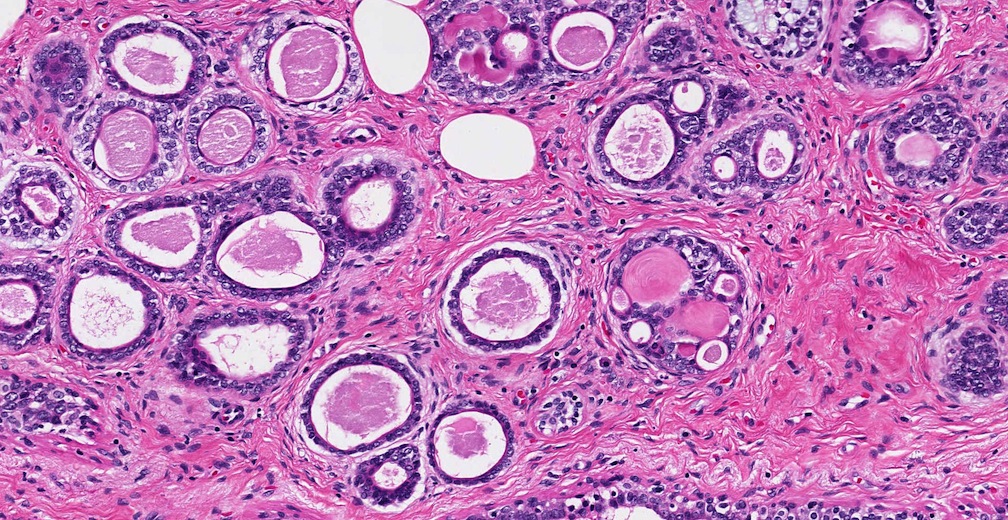
Microscopic images:

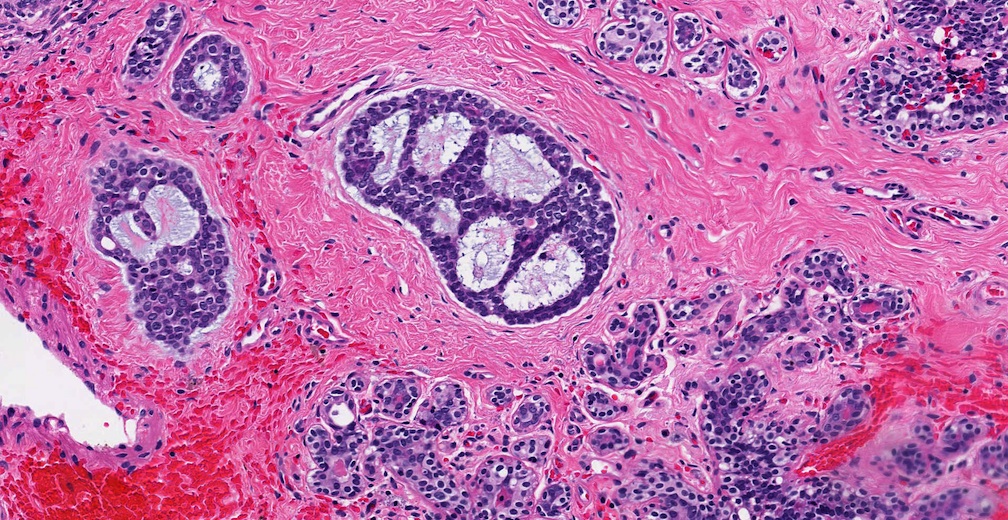
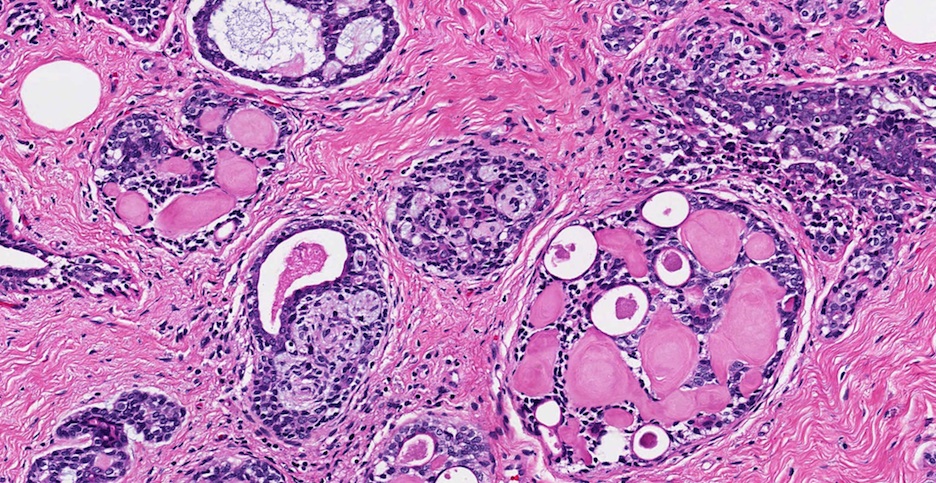
What is your diagnosis?
Diagnosis: Adenoid cystic carcinoma of the breast
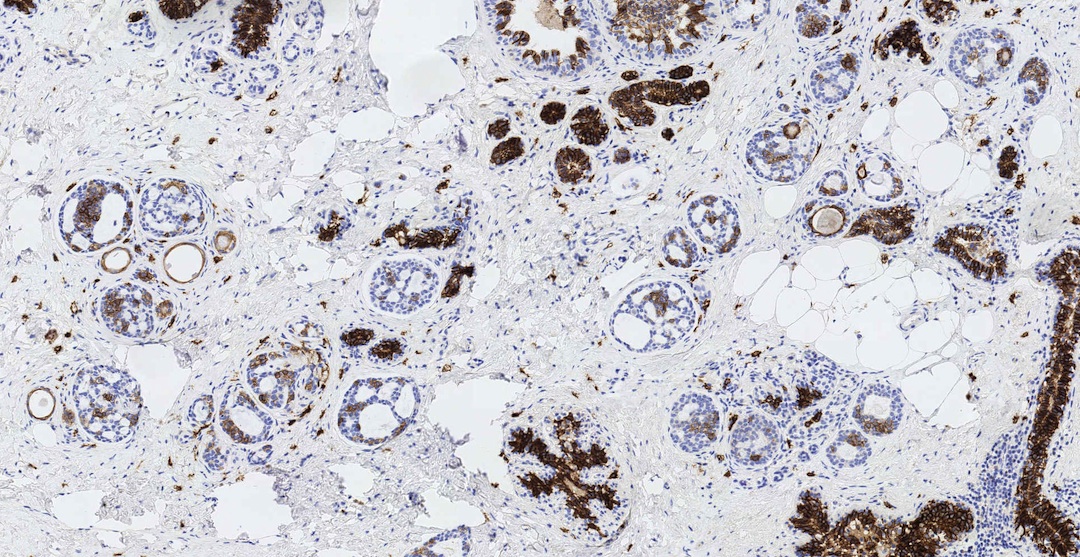
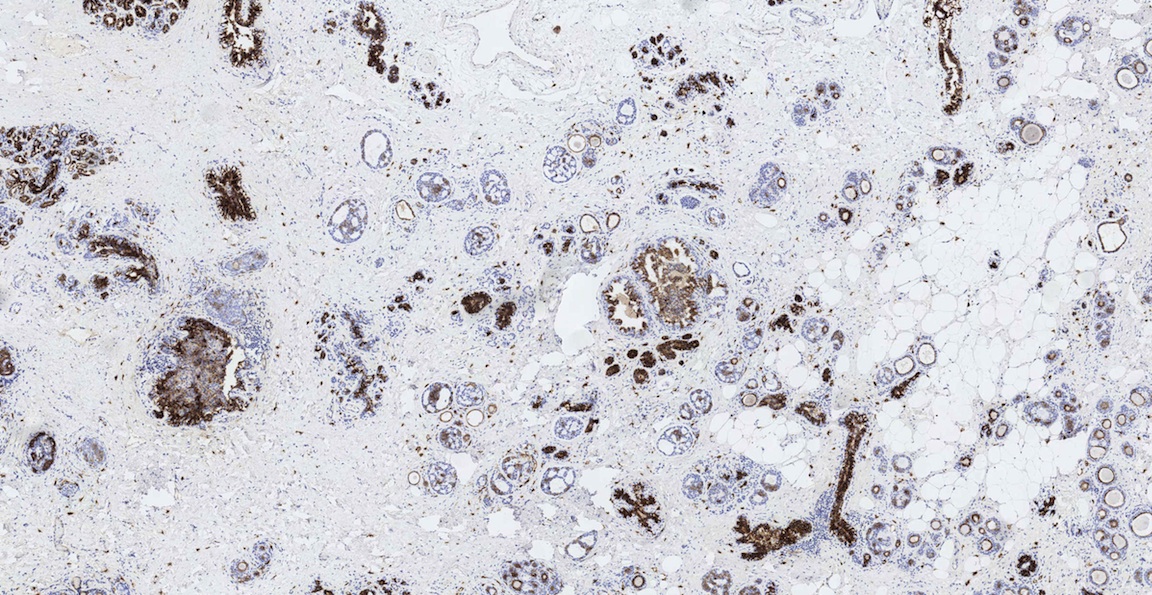
Immunostains:
Discussion:
Adenoid cystic carcinoma is a rare breast tumor (0.1% of breast carcinomas) and identical to its salivary gland counterpart (Ann Surg Oncol 2013;20:2236). Other salivary gland-like tumors of the breast include mucoepidermoid carcinoma and acinic cell carcinoma.
Adenoid cystic carcinoma has cribriform, solid, trabecular and basaloid patterns, 2 types of cavities and 2 types of cells. True glandular lumina are lined by ductal epithelium (EMA+, keratin+, CD117+) and eosinophilic cylinders with basement membrane material are lined by basal / myoepithelial type cells (p63+, S100+, smooth muscle actin+, vimentin+) (Mod Pathol 2005;18:1623). Secretions in the true lumina are PAS+ diastase resistant and cribriform spaces are Alcian blue+. All salivary gland tumors of the breast, including adenoid cystic carcinoma, are characteristically negative for ER, PR and HER2 (triple negative), and express basal cell markers CK5/6, P-cadherin and p63 (Appl Immunohistochem Mol Morphol 2013;21:283). The MYB::NFIB fusion gene [t(6;9)(q22-23;p23-24)] has been found in some breast adenoid cystic carcinomas (J Pathol 2012;226:84).
CD117+ staining in this case is indicated above.
The differential diagnosis includes collagenous spherulosis, a rare, benign disorder of intraluminal clusters of eosinophilic or rarely basophilic collagen rich spherules within spaces, surrounded by flattened myoepithelial cells. Collagenous spherulosis typically occurs in proliferative lesions, and is usually incidental, unlike the present case which presented as a mass.
Cribriform carcinoma, either in situ or invasive may have similar morphology, but only has one cell type. In contrast to adenoid cystic carcinoma, it is ER+, PR+, p63- and CD117-.
Treatment of adenoid cystic carcinoma of the breast is excision with clear margins, and possibly radiation. Axillary nodal metastases are rare, so axillary dissection may not be necessary. It has a good to excellent prognosis, better than at other locations, with high rates of positive margins but less recurrence or metastases than usual ductal carcinoma.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jessica Kozel, University of Nebraska Medical Center, for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.

Rabbit Monoclonals to Novel Targets & Evaluate a RabMAb
Interested in trying an EP Clone RabMAb? You can now Evaluate EP Clones for FREE. Learn how at epitomics.com/diagnostics.
EP Clones are a line of high quality rabbit antibodies for anatomic pathology. Our collection now includes antibodies to novel targets including: Aurora B,
ERCC1,
Cadherin-6, MSH2, RRM1, and S100P among others. We now have over 200 EP Clone antibodies, fully validated for use in IHC with FFPE tissues.
Website news:
(1) Thanks to Dr. Grace C. Yang for contributing images of papillary thyroid microcarcinoma and Hurthle cell tumors.
(2) In March 2013, we again had record traffic, with 373,735 visits (9,305,497 "hits").
Visit and follow our Blog to see recent updates to the website.
(1) Thanks to Dr. Grace C. Yang for contributing images of papillary thyroid microcarcinoma and Hurthle cell tumors.
(2) In March 2013, we again had record traffic, with 373,735 visits (9,305,497 "hits").
Visit and follow our Blog to see recent updates to the website.
Case #271
Clinical history:
A 61 year old woman presented with a mammographic left breast mass. An incisional biopsy was performed.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Adenoid cystic carcinoma of the breast
Immunostains:
Discussion:
Adenoid cystic carcinoma is a rare breast tumor (0.1% of breast carcinomas) and identical to its salivary gland counterpart (Ann Surg Oncol 2013;20:2236). Other salivary gland-like tumors of the breast include mucoepidermoid carcinoma and acinic cell carcinoma.
Adenoid cystic carcinoma has cribriform, solid, trabecular and basaloid patterns, 2 types of cavities and 2 types of cells. True glandular lumina are lined by ductal epithelium (EMA+, keratin+, CD117+) and eosinophilic cylinders with basement membrane material are lined by basal / myoepithelial type cells (p63+, S100+, smooth muscle actin+, vimentin+) (Mod Pathol 2005;18:1623). Secretions in the true lumina are PAS+ diastase resistant and cribriform spaces are Alcian blue+. All salivary gland tumors of the breast, including adenoid cystic carcinoma, are characteristically negative for ER, PR and HER2 (triple negative), and express basal cell markers CK5/6, P-cadherin and p63 (Appl Immunohistochem Mol Morphol 2013;21:283). The MYB::NFIB fusion gene [t(6;9)(q22-23;p23-24)] has been found in some breast adenoid cystic carcinomas (J Pathol 2012;226:84).
CD117+ staining in this case is indicated above.
The differential diagnosis includes collagenous spherulosis, a rare, benign disorder of intraluminal clusters of eosinophilic or rarely basophilic collagen rich spherules within spaces, surrounded by flattened myoepithelial cells. Collagenous spherulosis typically occurs in proliferative lesions, and is usually incidental, unlike the present case which presented as a mass.
Cribriform carcinoma, either in situ or invasive may have similar morphology, but only has one cell type. In contrast to adenoid cystic carcinoma, it is ER+, PR+, p63- and CD117-.
Treatment of adenoid cystic carcinoma of the breast is excision with clear margins, and possibly radiation. Axillary nodal metastases are rare, so axillary dissection may not be necessary. It has a good to excellent prognosis, better than at other locations, with high rates of positive margins but less recurrence or metastases than usual ductal carcinoma.
