
7 March 2013 - Case #268
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Ahmed Lazim, Al-Jumhori Teaching Hospital, Mosul (Iraq), for contributing this case.
Case #268
Clinical history:
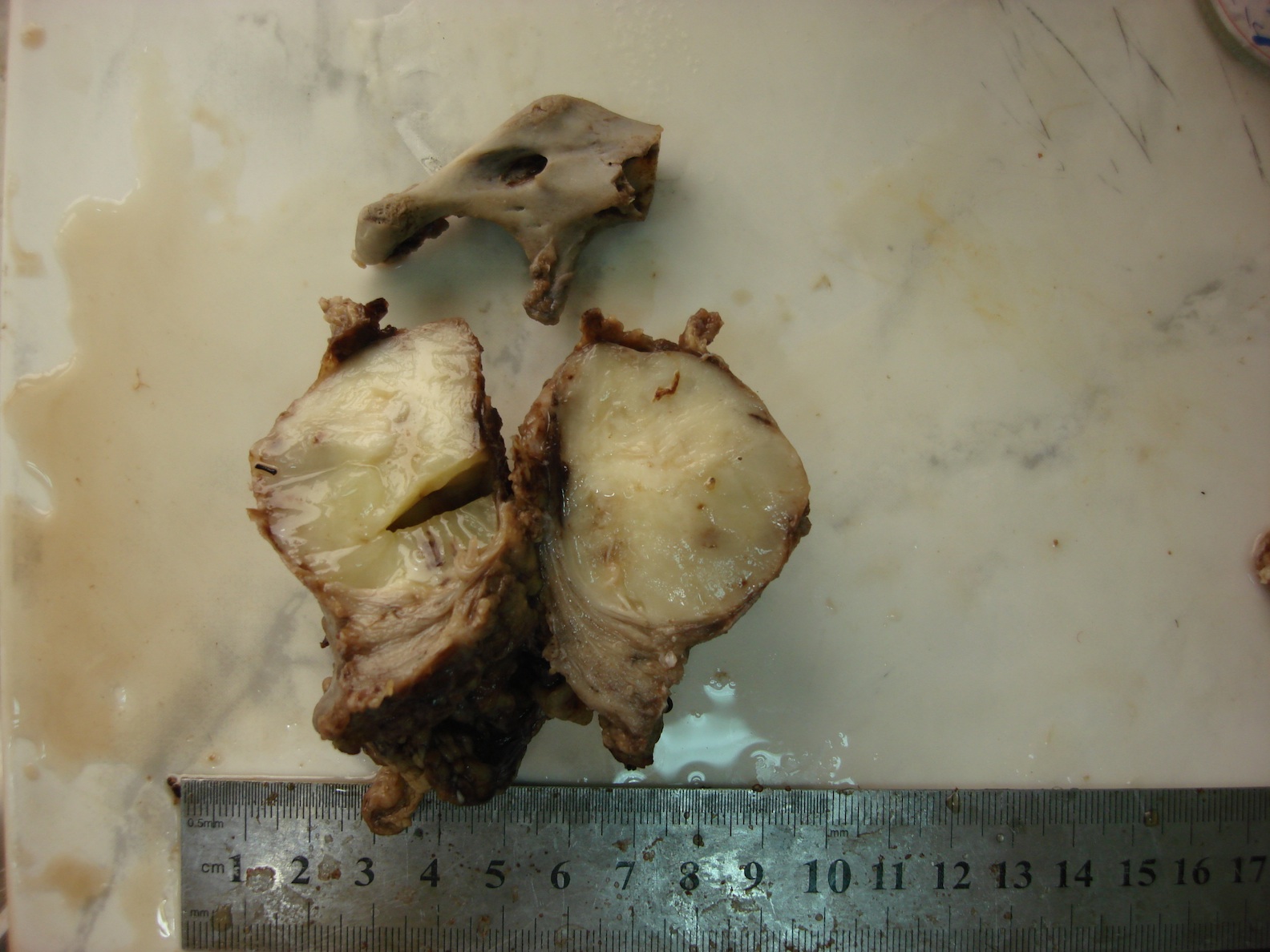
A 2 year old boy presented with a history of trauma 2 months previously. Ultrasound revealed a hematoma-like mass at the zygomatic bone, but one month later, the mass had enlarged to 7 cm. Excision revealed a 700 gram, 9 x 6 x 4.5 cm specimen of a nodular mass with parotid gland, 2 lymph nodes and a fragment of zygomatic bone.
Gross images:

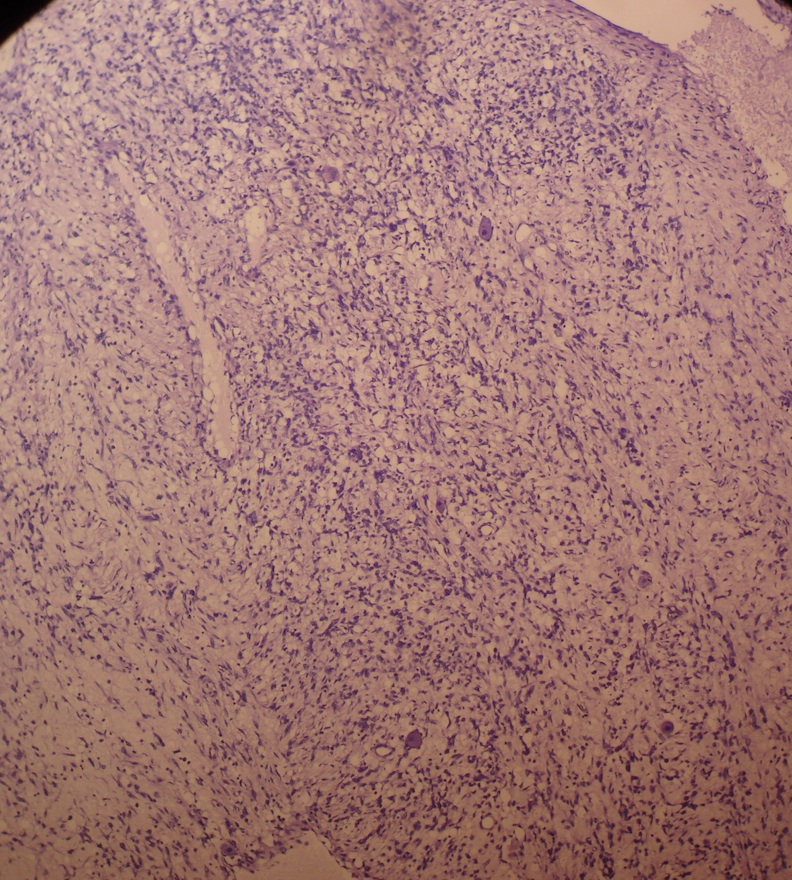
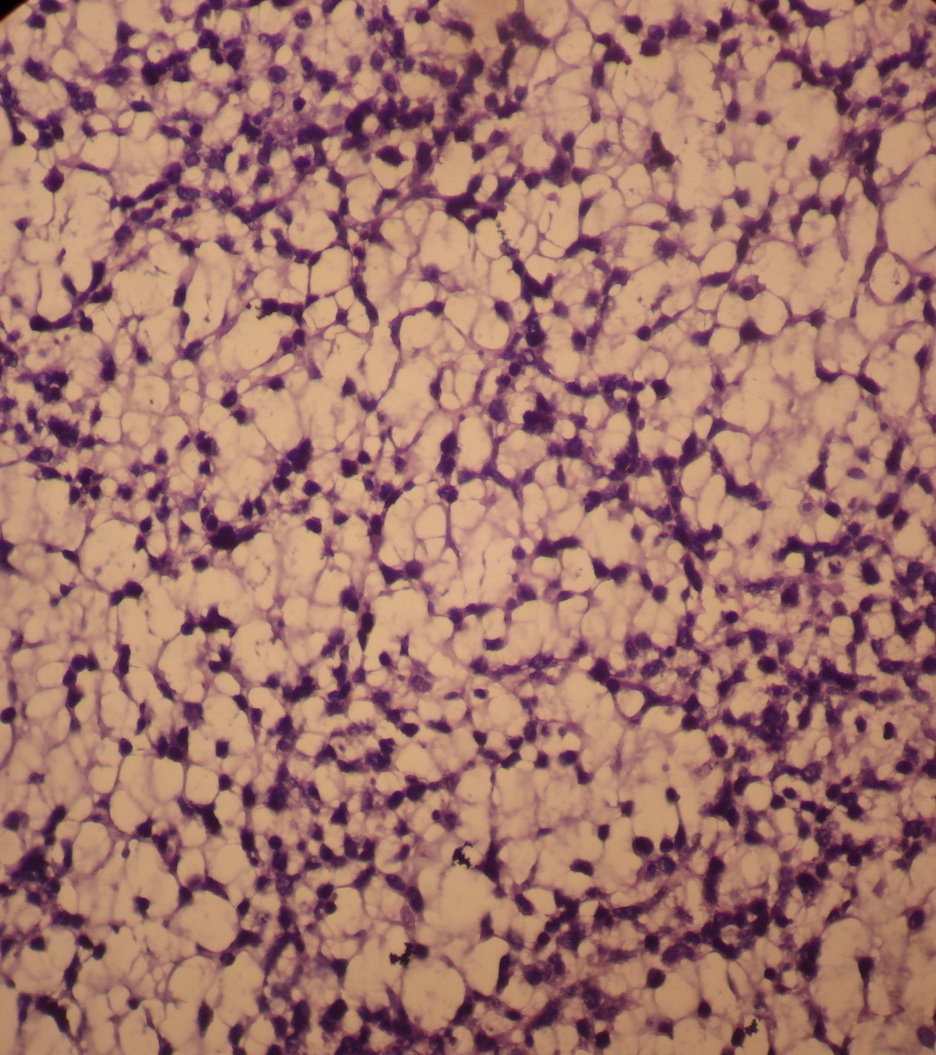
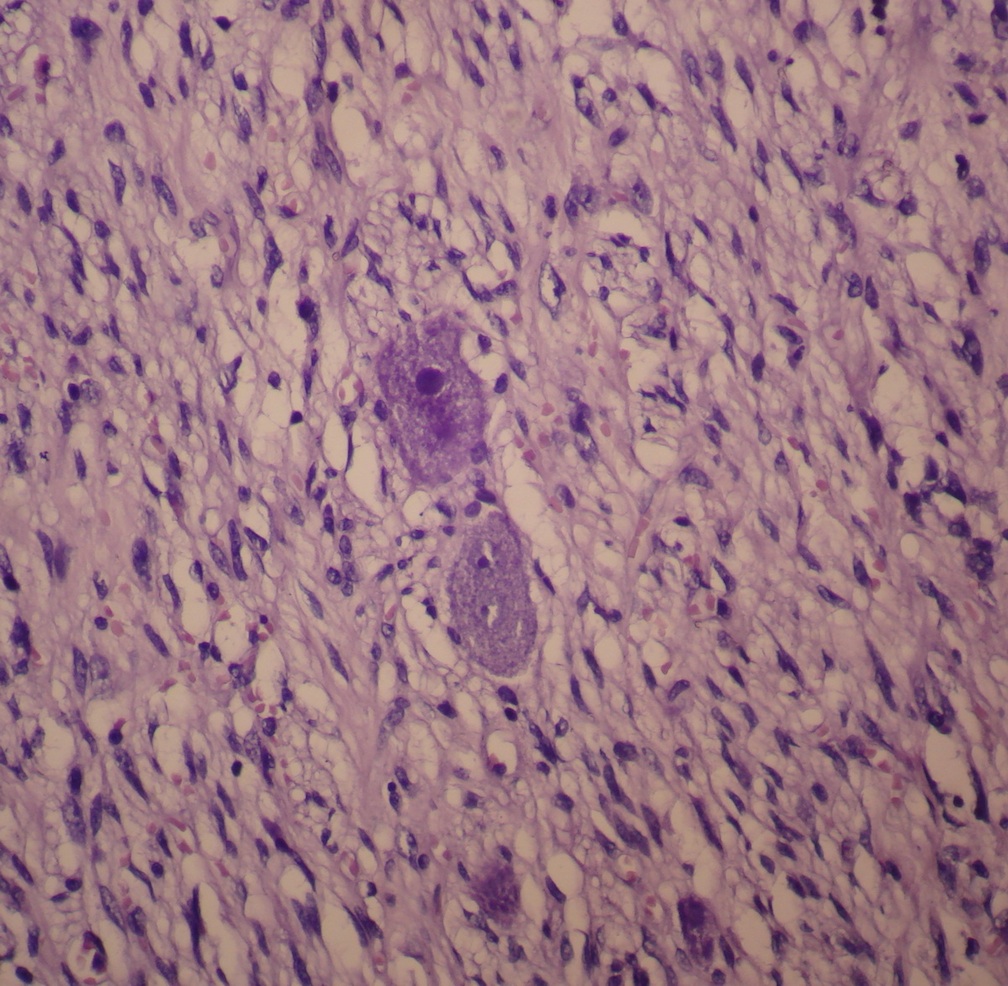
Microscopic images:


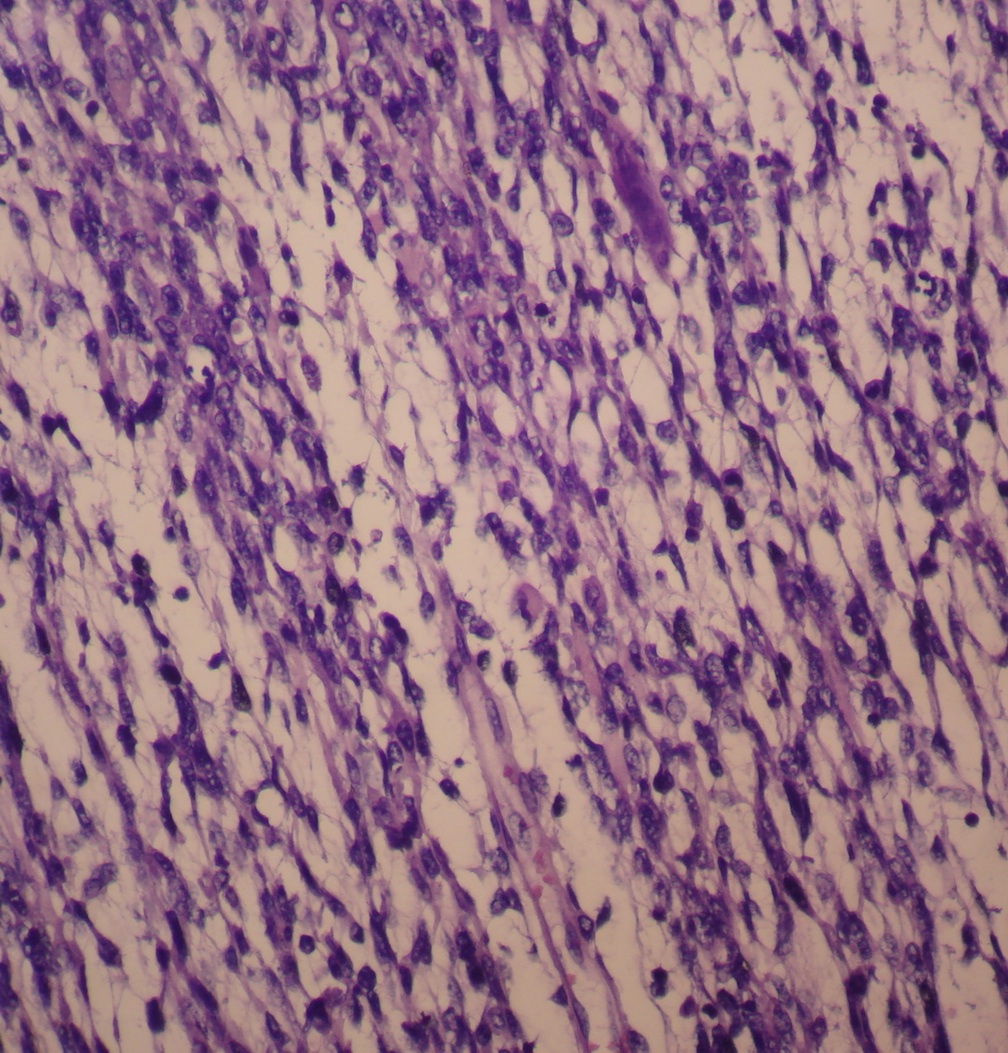
What is your diagnosis?
Diagnosis: Gangliorhabdomyosarcoma
Discussion:
Embryonal rhabdomyosarcoma is a primitive soft tissue sarcoma with small blue cells resembling embryonic skeletal muscle. It is the most common rhabdomyosarcoma (RMS) subtype (65% of RMS cases), and usually occurs in children ages 3-10 years in the head and neck (nasal and oral cavities, orbit, ear), prostate or paratesticular regions.
Gangliorhabdomyosarcoma is a rare variant of embryonal rhabdomyosarcoma which also has cells exhibiting neuronal differentiation (Histopathology 1986;10:181). A related entity is malignant ectomesenchymoma, composed of a malignant mesenchymal component (often but not exclusively rhabdomyosarcoma) and a neuroectodermal component (often ganglion cells or neuroblasts) (Cancer 1987;59:1791, J Cancer Res Ther 2012;8:465).
The differential diagnosis includes Triton tumor (rhabdomyosarcoma plus MPNST), Wilms tumor and teratoma.
Optimal treatment is not well defined for this rare tumor but most authors recommend a combination of surgery, radiotherapy and a chemotherapeutic protocol based on the RMS component (Indian J Med Paediatr Oncol 2011;32:242).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Ahmed Lazim, Al-Jumhori Teaching Hospital, Mosul (Iraq), for contributing this case.
Website news:
(1) Thanks to all who stopped by our booth at the USCAP meeting in Baltimore. We received many suggestions and signed up many reviewers, which we hope will make the website even more valuable to the Pathology community. If you have any comments or suggestions on making PathologyOutlines.com more useful to you, please let us know.
(2) Many of the Modern Pathology links are not working, due to an IT problem apparently on their end - we have contacted them and are working on the problem.
Visit and follow our Blog to see recent updates to the website.
(1) Thanks to all who stopped by our booth at the USCAP meeting in Baltimore. We received many suggestions and signed up many reviewers, which we hope will make the website even more valuable to the Pathology community. If you have any comments or suggestions on making PathologyOutlines.com more useful to you, please let us know.
(2) Many of the Modern Pathology links are not working, due to an IT problem apparently on their end - we have contacted them and are working on the problem.
Visit and follow our Blog to see recent updates to the website.
Case #268
Clinical history:
A 2 year old boy presented with a history of trauma 2 months previously. Ultrasound revealed a hematoma-like mass at the zygomatic bone, but one month later, the mass had enlarged to 7 cm. Excision revealed a 700 gram, 9 x 6 x 4.5 cm specimen of a nodular mass with parotid gland, 2 lymph nodes and a fragment of zygomatic bone.
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Gangliorhabdomyosarcoma
Discussion:
Embryonal rhabdomyosarcoma is a primitive soft tissue sarcoma with small blue cells resembling embryonic skeletal muscle. It is the most common rhabdomyosarcoma (RMS) subtype (65% of RMS cases), and usually occurs in children ages 3-10 years in the head and neck (nasal and oral cavities, orbit, ear), prostate or paratesticular regions.
Gangliorhabdomyosarcoma is a rare variant of embryonal rhabdomyosarcoma which also has cells exhibiting neuronal differentiation (Histopathology 1986;10:181). A related entity is malignant ectomesenchymoma, composed of a malignant mesenchymal component (often but not exclusively rhabdomyosarcoma) and a neuroectodermal component (often ganglion cells or neuroblasts) (Cancer 1987;59:1791, J Cancer Res Ther 2012;8:465).
The differential diagnosis includes Triton tumor (rhabdomyosarcoma plus MPNST), Wilms tumor and teratoma.
Optimal treatment is not well defined for this rare tumor but most authors recommend a combination of surgery, radiotherapy and a chemotherapeutic protocol based on the RMS component (Indian J Med Paediatr Oncol 2011;32:242).
