
14 February 2013 - Case #266
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Saroona Haroon, The Aga Khan University Hospital (Pakistan), for contributing this case and the discussion.
Case #266
Clinical history:
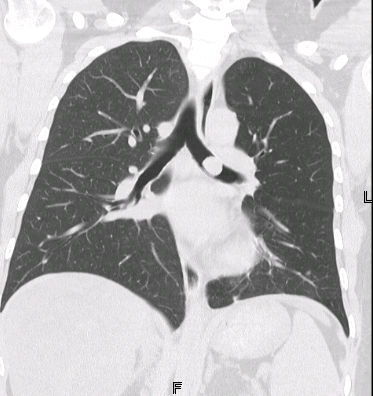
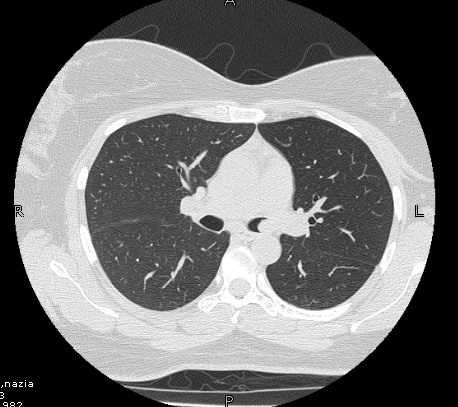
A 30 year old woman presented with hemoptysis and fever for 1 week. High resolution CT showed a well defined, rounded, high attenuation endobronchial lesion arising from the posterosuperior wall of the left main bronchus. A biopsy was performed.
Radiology images:
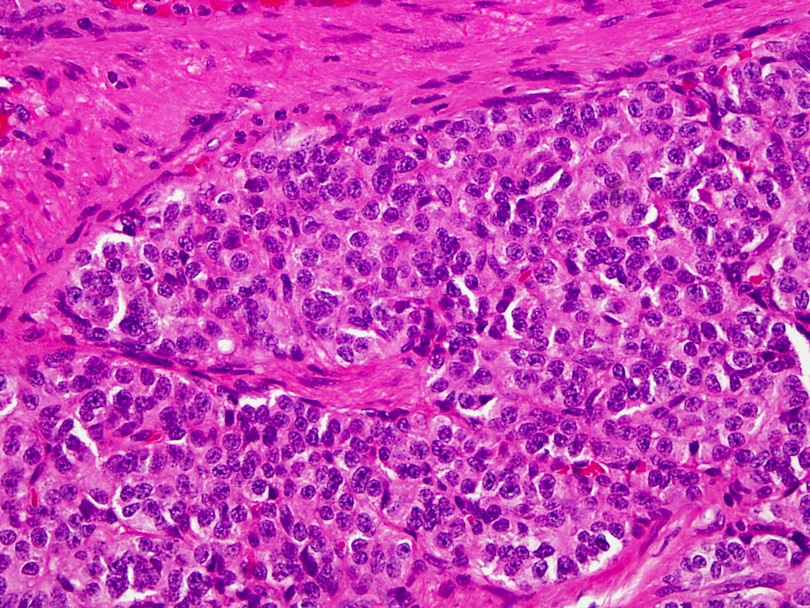
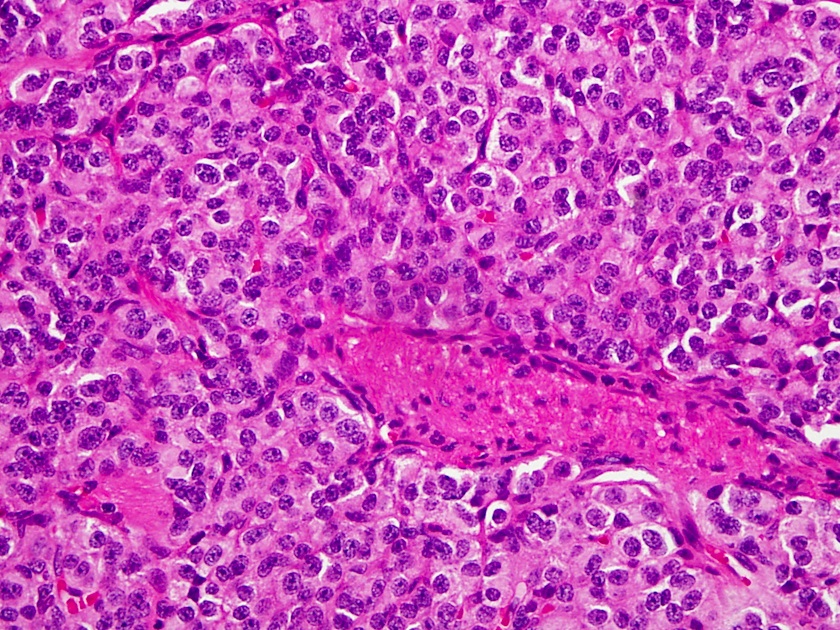
Microscopic images:

What is your diagnosis?
Diagnosis: Endobronchial carcinoid
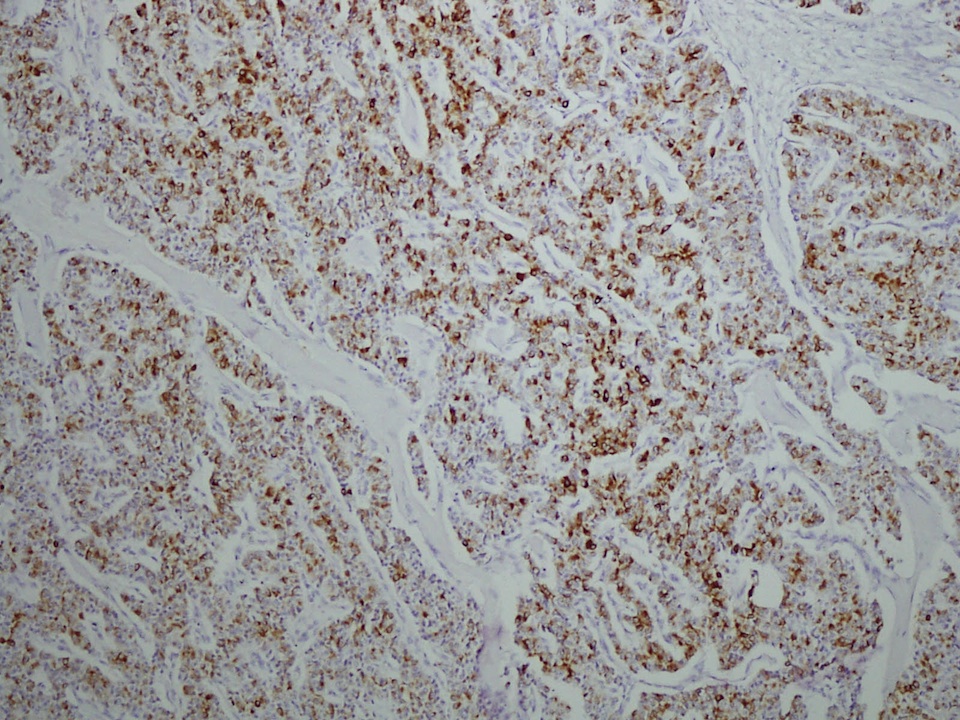
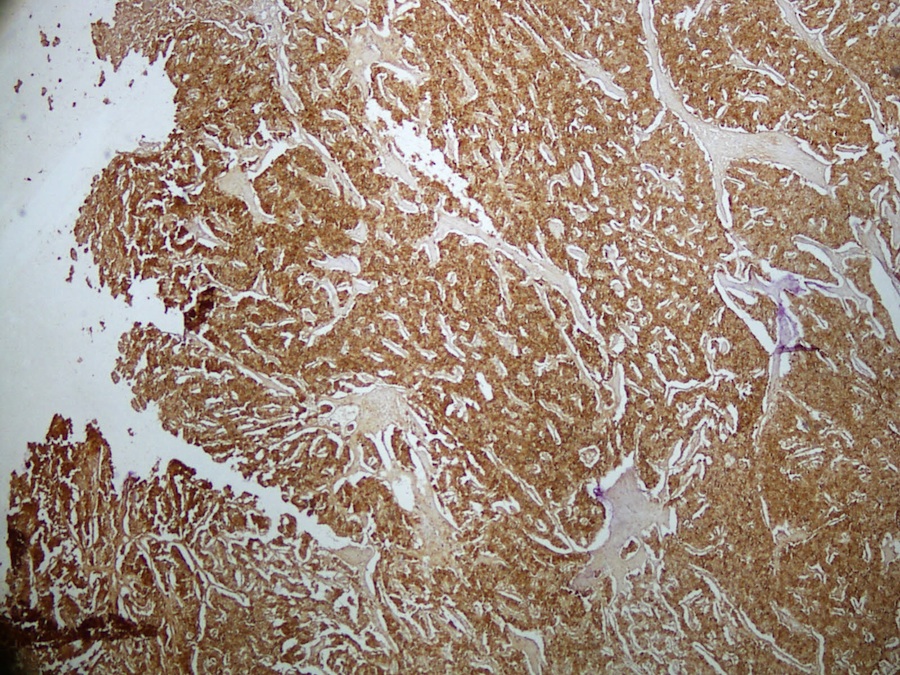
Immunostains:

Discussion:
The World Health Organization classification recognizes four histologic subtypes of pulmonary neuroendocrine carcinomas: typical carcinoid, atypical carcinoid, small cell carcinoma and large cell neuroendocrine carcinoma (IARC: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart, 3rd Edition, 2004, Clin Chest Med 2011;32:669). Carcinoid tumors, also called well-differentiated neuroendocrine carcinoma, represent 1 - 2% of invasive lung tumors. They rarely are associated with the carcinoid syndrome of flushing, diarrhea and cyanosis.
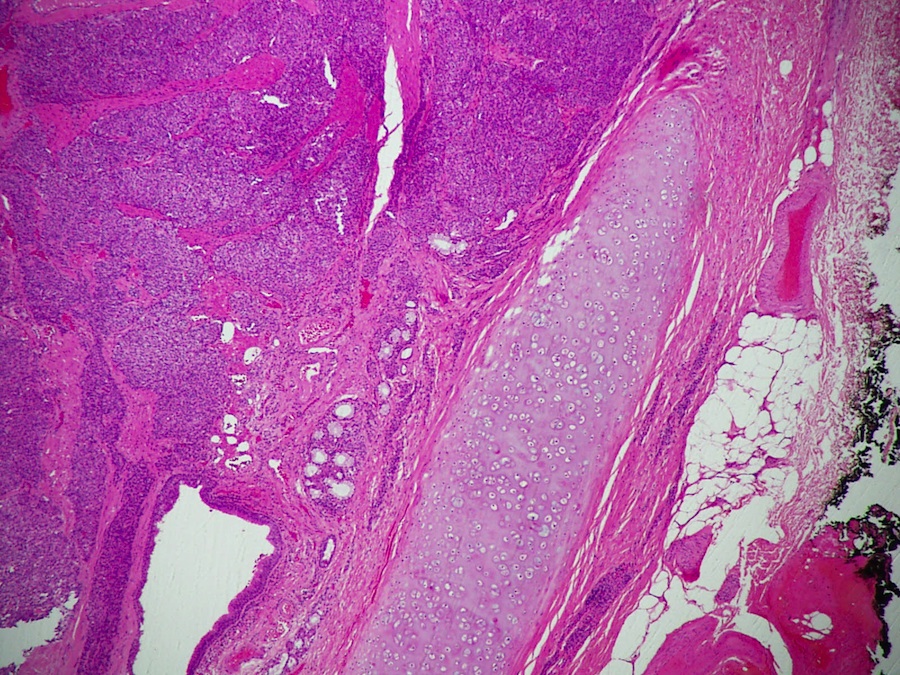
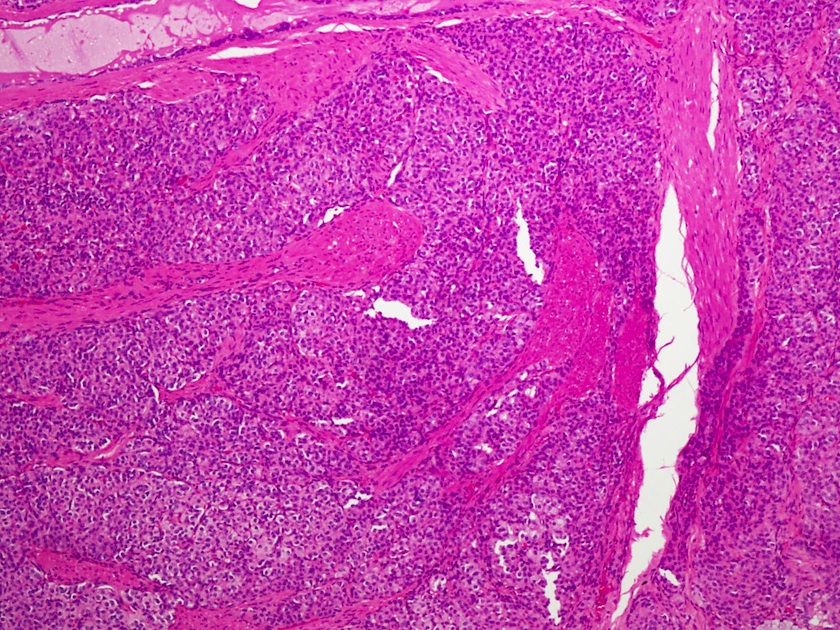
Pulmonary bronchial tumors either arise centrally (major bronchi) or peripherally (subpleural parenchyma) as well defined, smooth lesions without necrosis. They consist of nests or trabeculae of medium sized polygonal cells with lightly eosinophilic cytoplasm, low nuclear grade and round to oval finely granular nuclei. The vascular stroma is typically scant, but may contain amyloid or bone. Various patterns include spindle cell, palisading, papillary, glandular and follicular. Carcinoid tumors have no / minimal mitotic activity (< 2/10HPF) and no necrosis.
The differential diagnosis includes other neuroendocrine lung tumors, including tumorlet (< 5 mm), metastatic carcinoid from the GI tract or elsewhere, atypical carcinoid (2 - 10 mitotic figures/HPF, necrosis, often atypia or pleomorphism), large cell neuroendocrine carcinoma and small cell neuroendocrine carcinoma (atypia, pleomorphism, mitotic figures, necrosis). Tumors with a pseudoglandular pattern may resemble adenocarcinoma (marked atypia throughout).
Bronchial carcinoid tumors are locally invasive, but only rarely metastasize. The 10 year overall survival is 72% (Am Surg 2011;77:1669). In children, they may metastasize regardless of the histology (Arch Pathol Lab Med 2003;127:1200).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Saroona Haroon, The Aga Khan University Hospital (Pakistan), for contributing this case and the discussion.
Website news:
(1) We have updated the Trachea chapter based on reviews by Adriana Handra-Luca, M.D. We have added new topics to the Forensics chapter, written by Terrill L. Tops, M.D.
(2) Our Feature Page for February highlights Microscopes / Microscopy Products, and includes Celestron, Leica Microsystems and Optronics. We also have a new Mystery Case on the right side of the Home Page.
(3) The most popular book sold through our Books pages for 2012 was Montgomery: Biopsy Interpretation of the Gastrointestinal Tract Mucosa: Volume 1: Non-Neoplastic.
Visit and follow our Blog to see recent updates to the website.
(1) We have updated the Trachea chapter based on reviews by Adriana Handra-Luca, M.D. We have added new topics to the Forensics chapter, written by Terrill L. Tops, M.D.
(2) Our Feature Page for February highlights Microscopes / Microscopy Products, and includes Celestron, Leica Microsystems and Optronics. We also have a new Mystery Case on the right side of the Home Page.
(3) The most popular book sold through our Books pages for 2012 was Montgomery: Biopsy Interpretation of the Gastrointestinal Tract Mucosa: Volume 1: Non-Neoplastic.
Visit and follow our Blog to see recent updates to the website.
Case #266
Clinical history:
A 30 year old woman presented with hemoptysis and fever for 1 week. High resolution CT showed a well defined, rounded, high attenuation endobronchial lesion arising from the posterosuperior wall of the left main bronchus. A biopsy was performed.
Radiology images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Endobronchial carcinoid
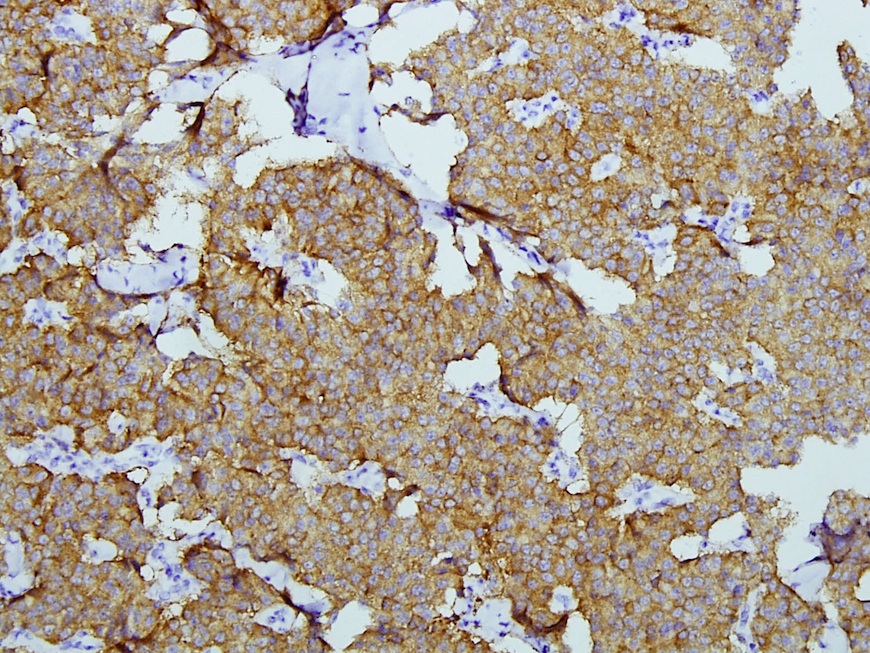
Immunostains:
Left to right: AE1 / AE3, chromogranin, synaptophysin, NSE
Discussion:
The World Health Organization classification recognizes four histologic subtypes of pulmonary neuroendocrine carcinomas: typical carcinoid, atypical carcinoid, small cell carcinoma and large cell neuroendocrine carcinoma (IARC: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart, 3rd Edition, 2004, Clin Chest Med 2011;32:669). Carcinoid tumors, also called well-differentiated neuroendocrine carcinoma, represent 1 - 2% of invasive lung tumors. They rarely are associated with the carcinoid syndrome of flushing, diarrhea and cyanosis.
Pulmonary bronchial tumors either arise centrally (major bronchi) or peripherally (subpleural parenchyma) as well defined, smooth lesions without necrosis. They consist of nests or trabeculae of medium sized polygonal cells with lightly eosinophilic cytoplasm, low nuclear grade and round to oval finely granular nuclei. The vascular stroma is typically scant, but may contain amyloid or bone. Various patterns include spindle cell, palisading, papillary, glandular and follicular. Carcinoid tumors have no / minimal mitotic activity (< 2/10HPF) and no necrosis.
The differential diagnosis includes other neuroendocrine lung tumors, including tumorlet (< 5 mm), metastatic carcinoid from the GI tract or elsewhere, atypical carcinoid (2 - 10 mitotic figures/HPF, necrosis, often atypia or pleomorphism), large cell neuroendocrine carcinoma and small cell neuroendocrine carcinoma (atypia, pleomorphism, mitotic figures, necrosis). Tumors with a pseudoglandular pattern may resemble adenocarcinoma (marked atypia throughout).
Bronchial carcinoid tumors are locally invasive, but only rarely metastasize. The 10 year overall survival is 72% (Am Surg 2011;77:1669). In children, they may metastasize regardless of the histology (Arch Pathol Lab Med 2003;127:1200).
