
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. David Cohen, Herzliya Medical Center (Israel) and Dr. Vincent Graffeo, Marshall University, West Virginia (USA), for contributing these cases.

Epitomics Rabbit Monoclonal Antibodies Show Optimal Staining in Third Party Assessments
In a series of independent assessments
, Epitomics antibodies to MSH6, Her2, CD99, CD20, CK8, and CK19 were rated as "optimally" staining. With our proprietary RabMAb technology, Epitomics continues to develop high quality antibodies and IHC kits for anatomical pathology use. See our full antibody listing and comparisons here
.
EP Clones™ are a line of high quality antibodies for anatomical pathology. Each antibody was generated using Epitomics patented Rabbit Monoclonal Antibody (RabMAb®) technology offering superior binding affinity and specificity. We now have over 150 antibodies, fully validated, ideal for FFPE tissues.
(1) In 2012, we reached another milestone, with 4 million visits (about 100 million "hits"), and on 12 December 2012, we had record traffic of 16,994 visits (416,813 "hits"), surpassing the prior record from almost exactly one year prior (on 13 December 2011). Thanks for your support.
(2) We are now hosted on a faster, more reliable server. Our host indicated that all 10,000+ files were transferred to the new server, but if you come across a "file not found" error that seems to refer to our website, please let us know.
(3) We have now converted about 50% of our 6600 topics to a new format with a separate page per topic, thumbnails of most images and an easier to read format. For some images, we use a "standard" thumbnail if we cannot legally or technically obtain a thumbnail.
(4) We have started to add Superpages to chapters as they are updated. It may take 2 weeks to add the superpages after the chapter update is completed. The Superpages links are at the end of the topical Table of Contents. The Superpages combine all topics in part of the Chapter (usually in 1-3 parts), to make it easier to search between related topics. For example, the in situ carcinoma Superpage contains all the in situ topics in one document. We keep each Superpage to a manageable size (< 1 MB) so it loads quickly.
Visit and follow our Blog to see recent updates to the website.
Case #262
Case #1 (contributed by Dr. David Cohen)
Clinical history:
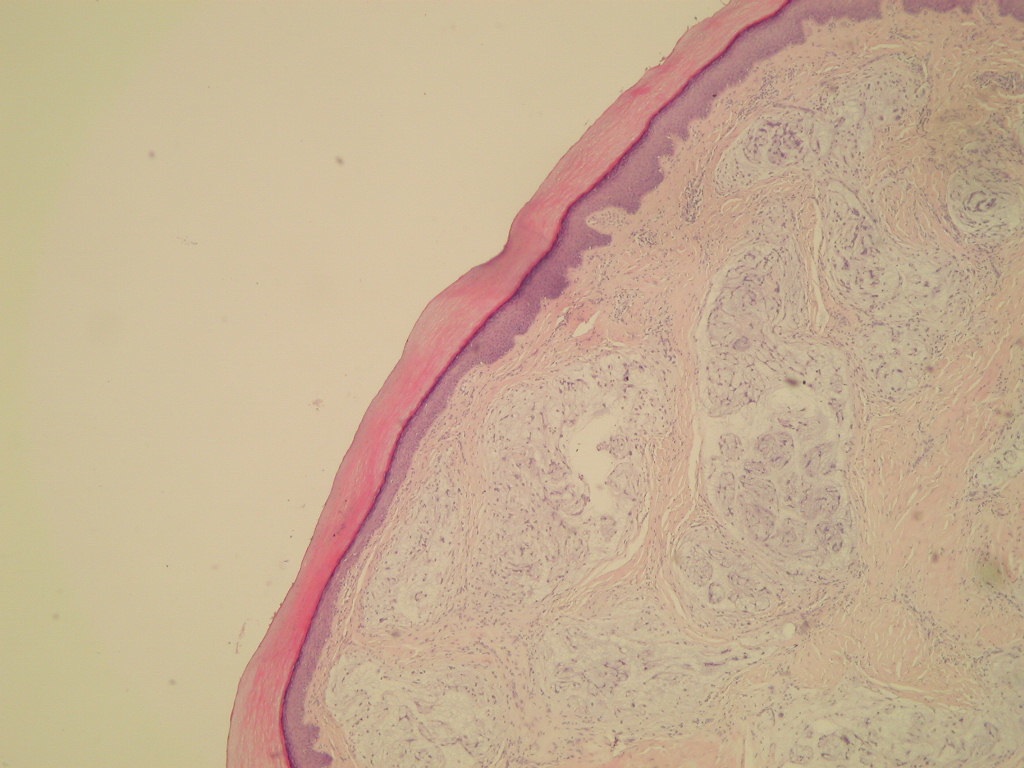
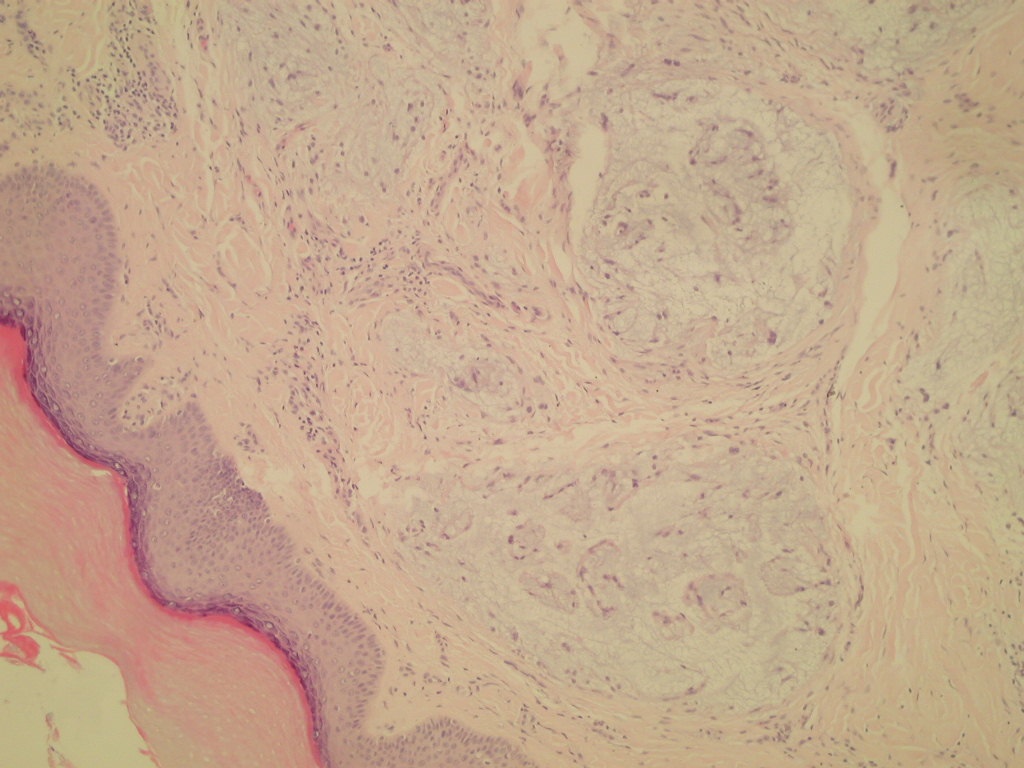
A 26 year old woman presented with a soft tissue tumor of her right thumb, which was excised, revealing a 2 cm nodular gray-white firm mass, covered by epithelium.
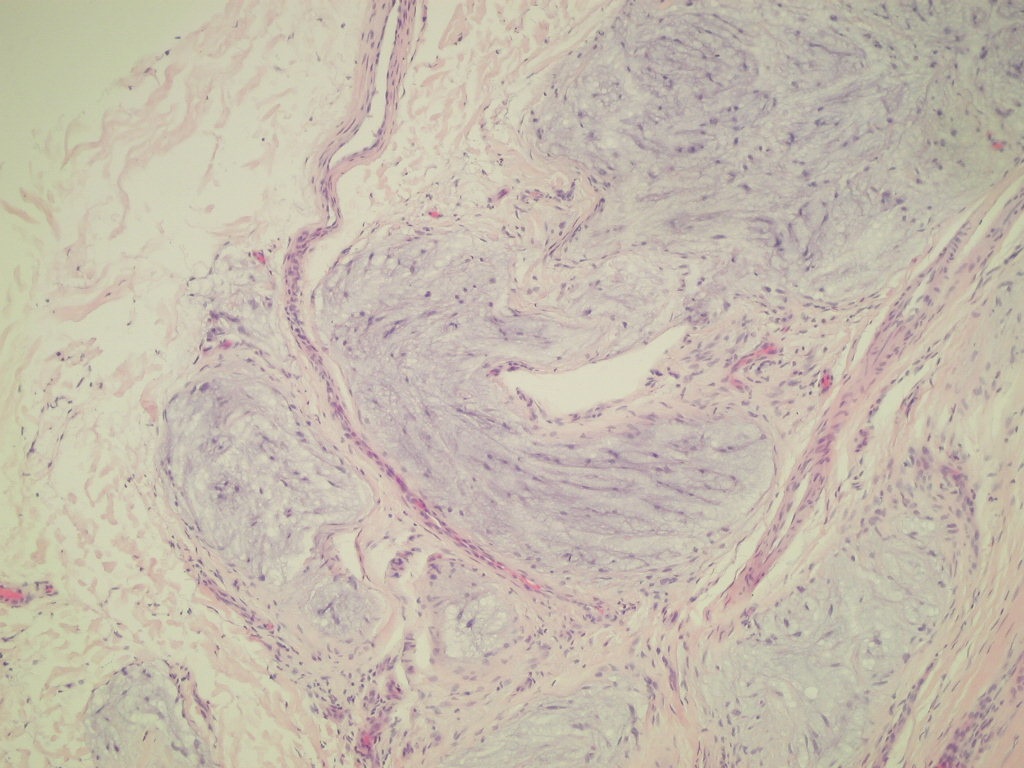
Microscopic images:
Case #2 (Contributed by Dr. Vincent Graffeo)
Clinical history:
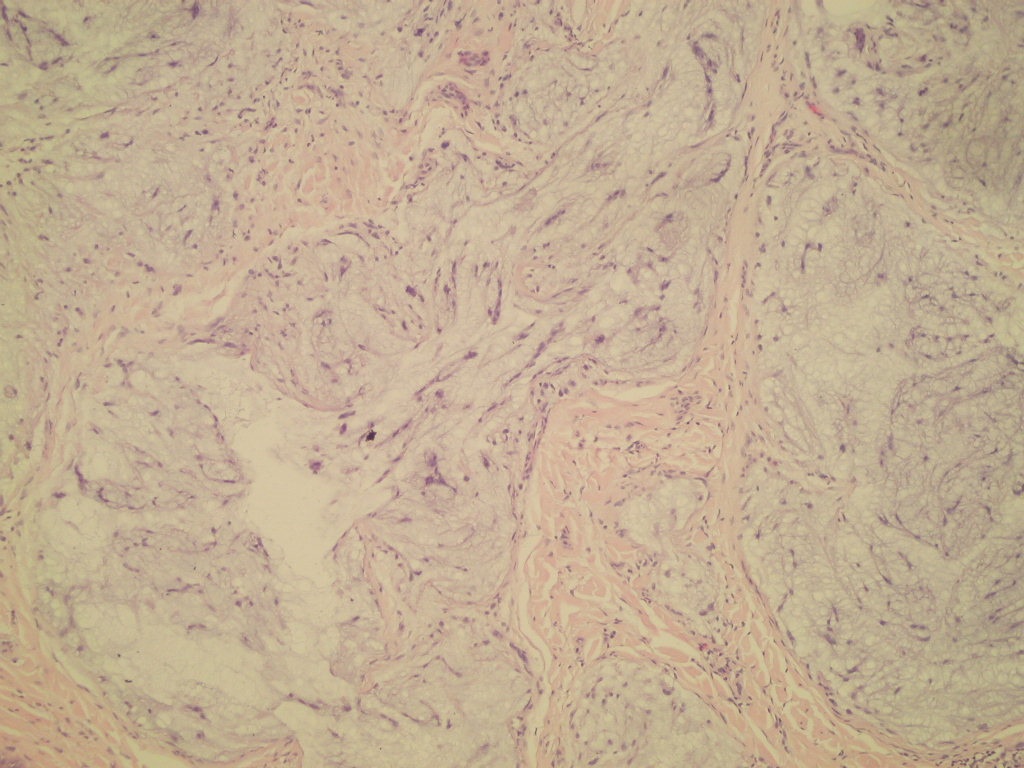
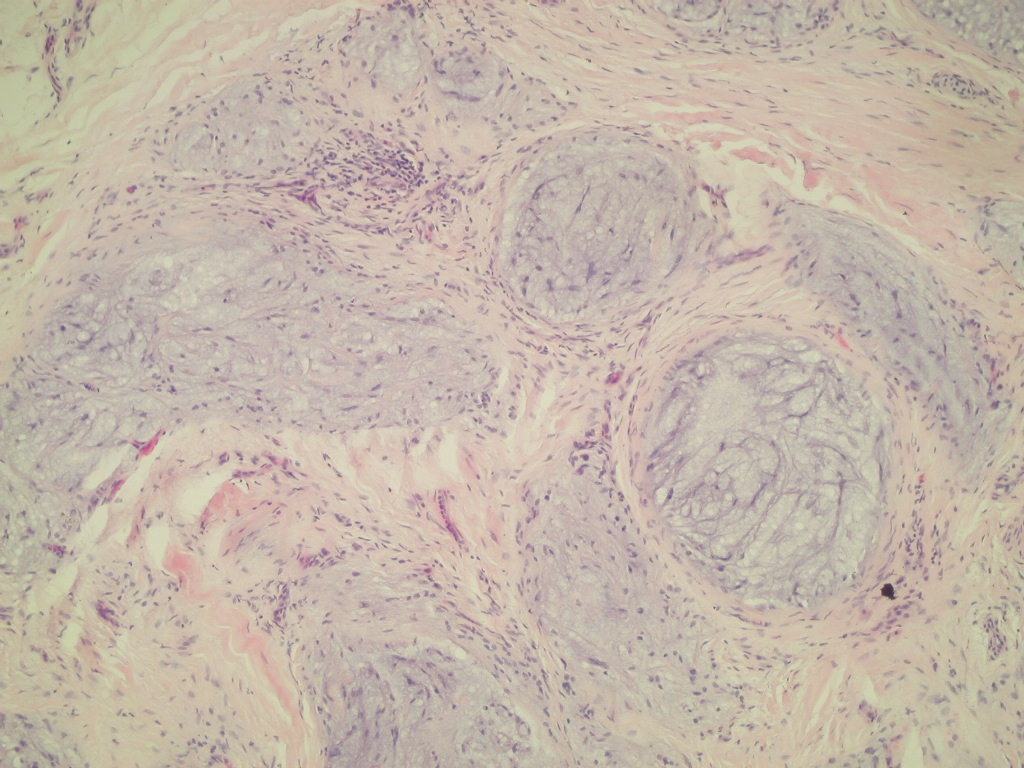
A 37 year old woman presented with a cyst on the right index finger, which was excised, revealing a 1.8 cm tan, solid nodule with a solid/slightly gelatinous cut surface.
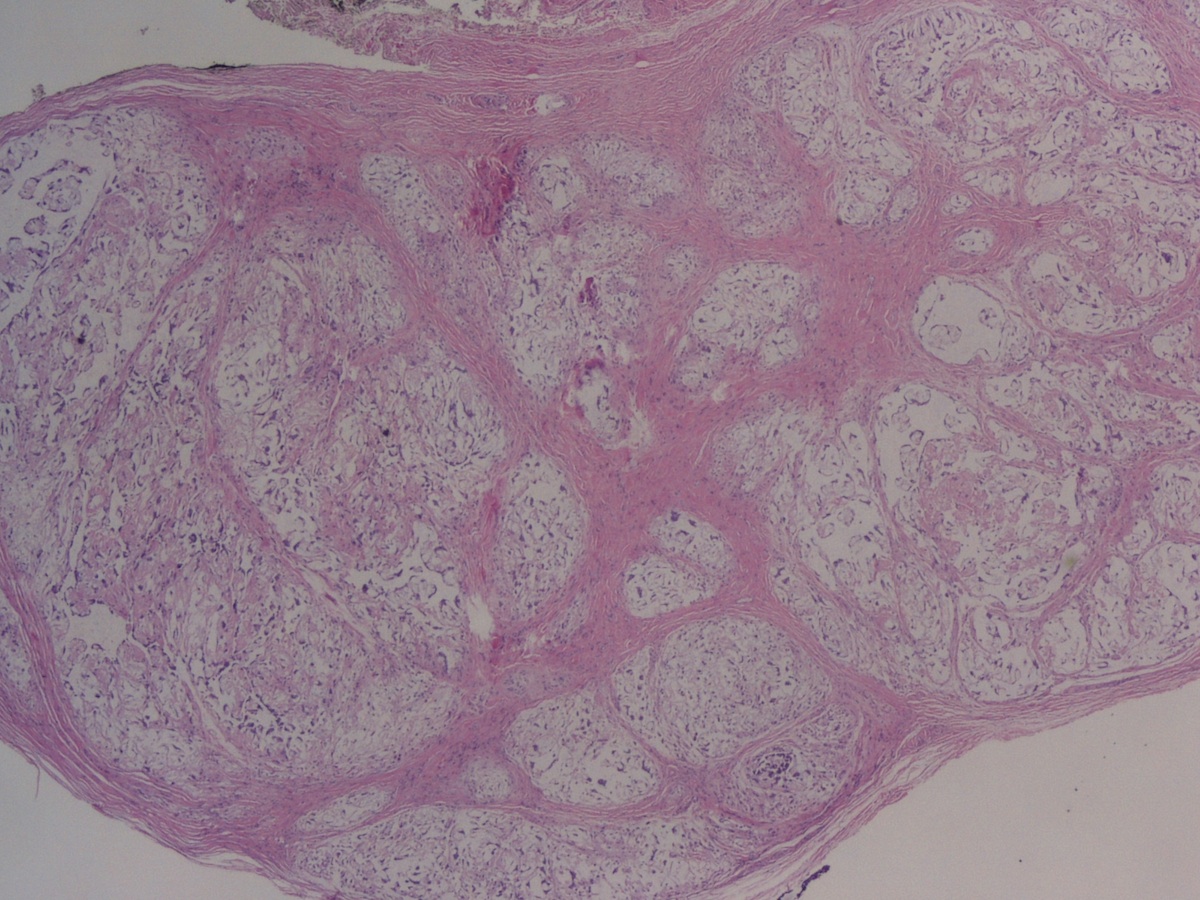
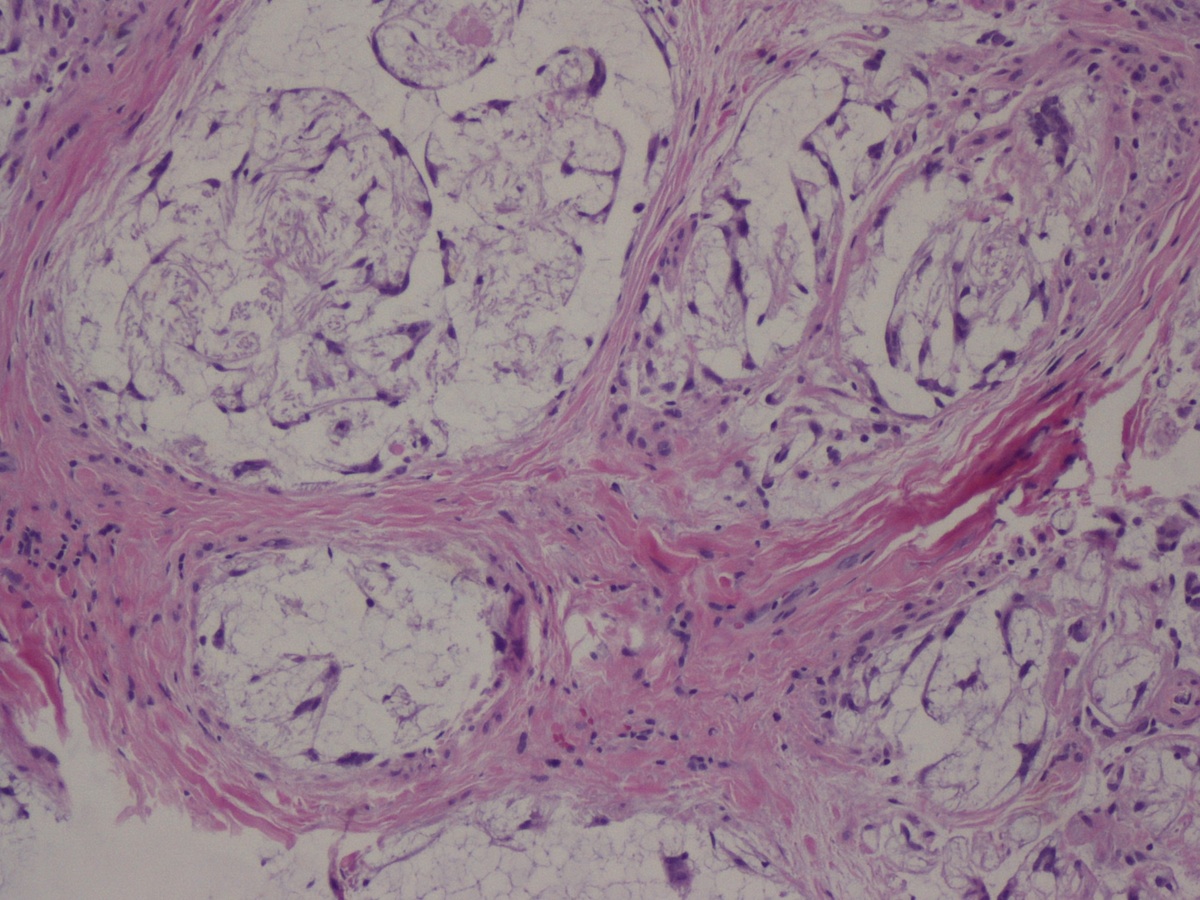
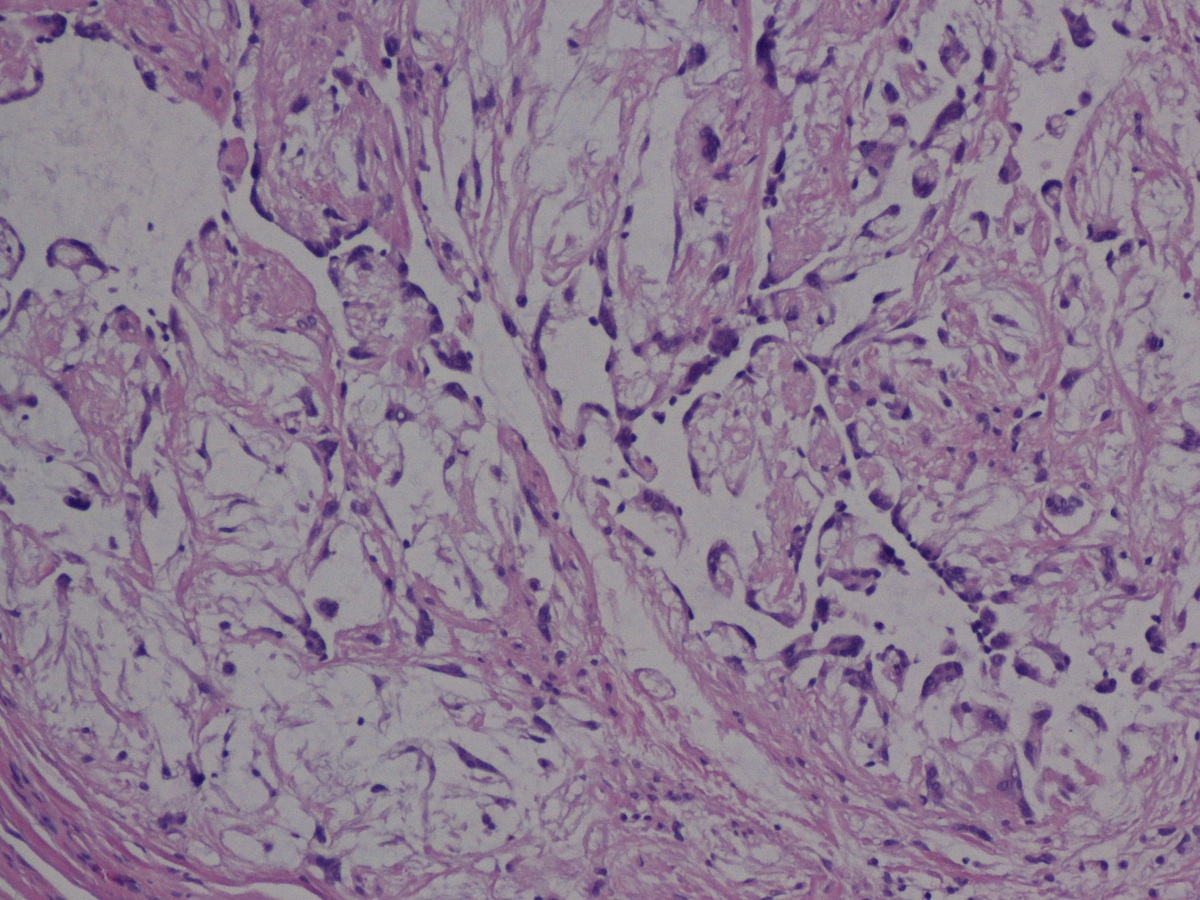
Microscopic images:

What is your diagnosis?
Diagnosis: Nerve sheath myxoma (both cases)
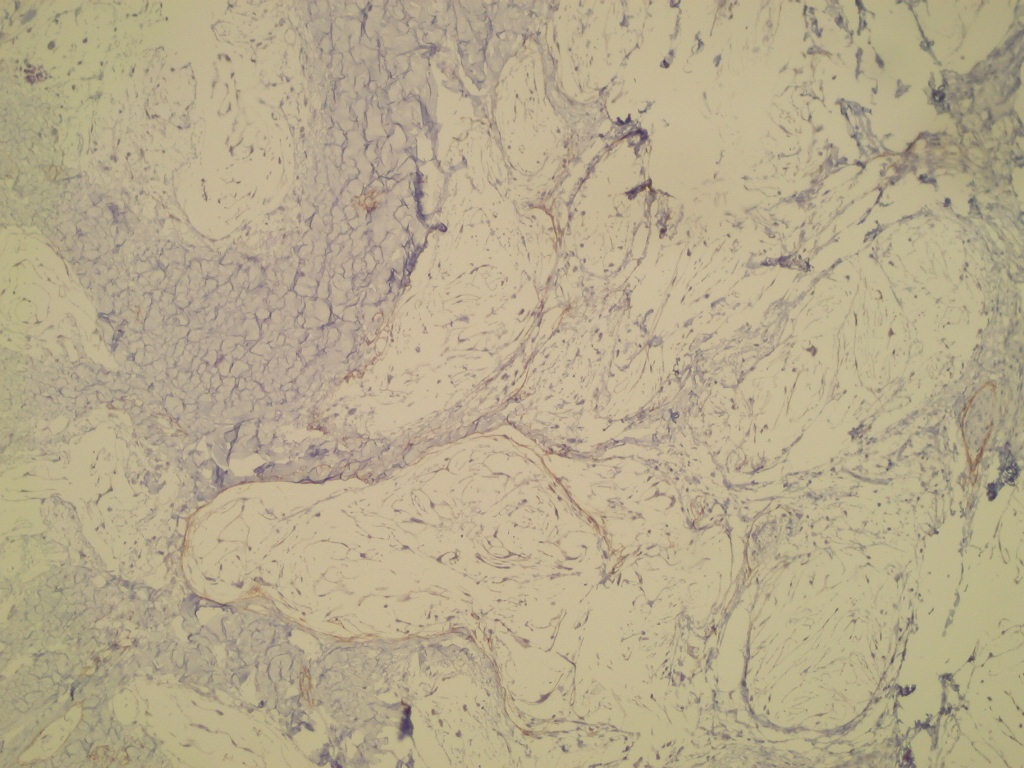
Immunostains:
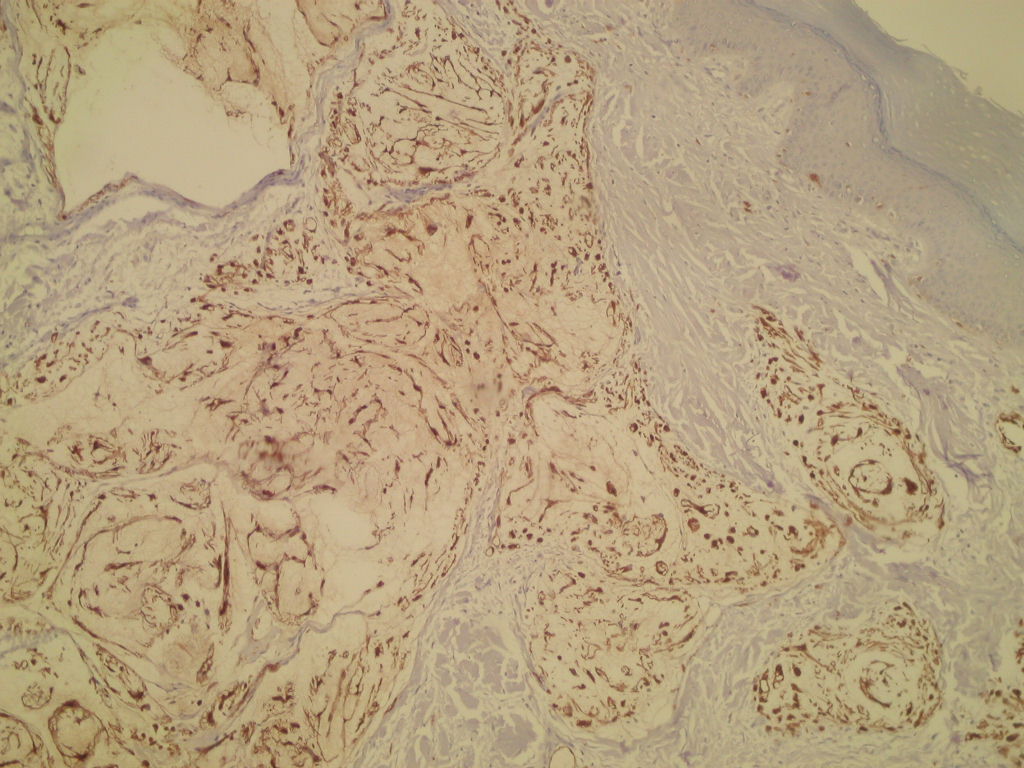
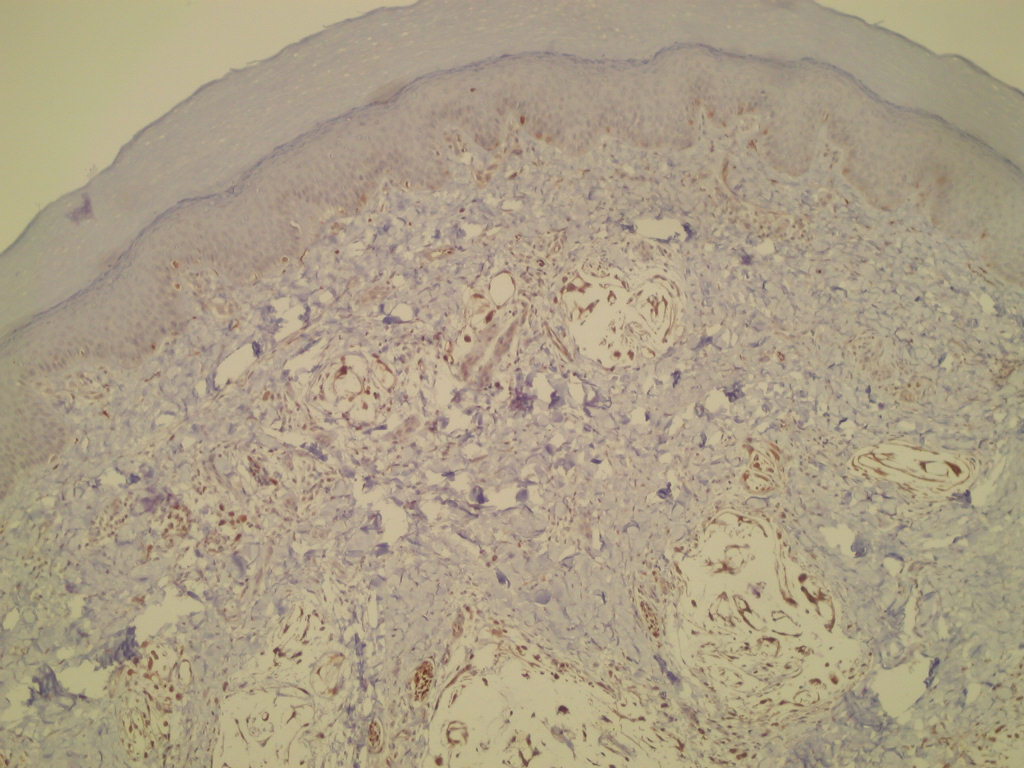
Left to right: S100, NSE, EMA
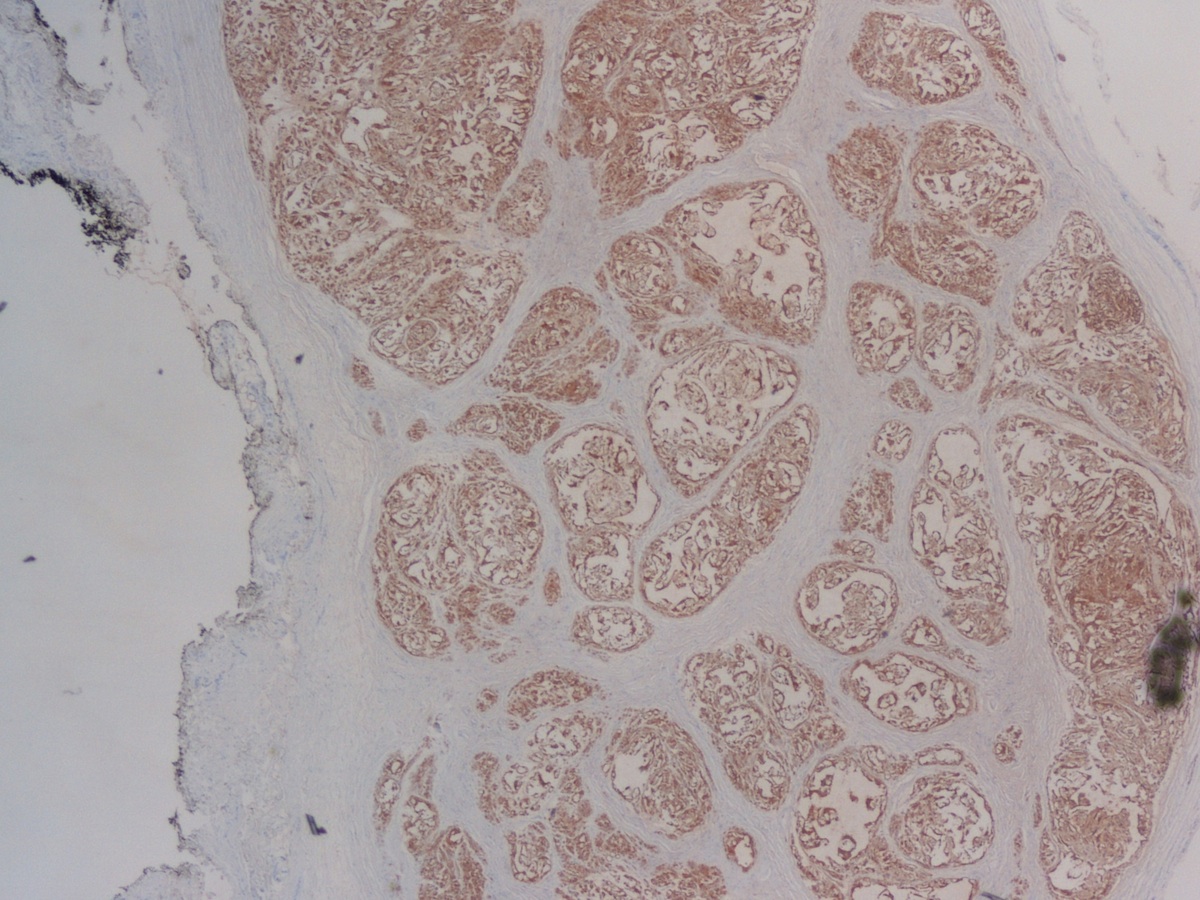
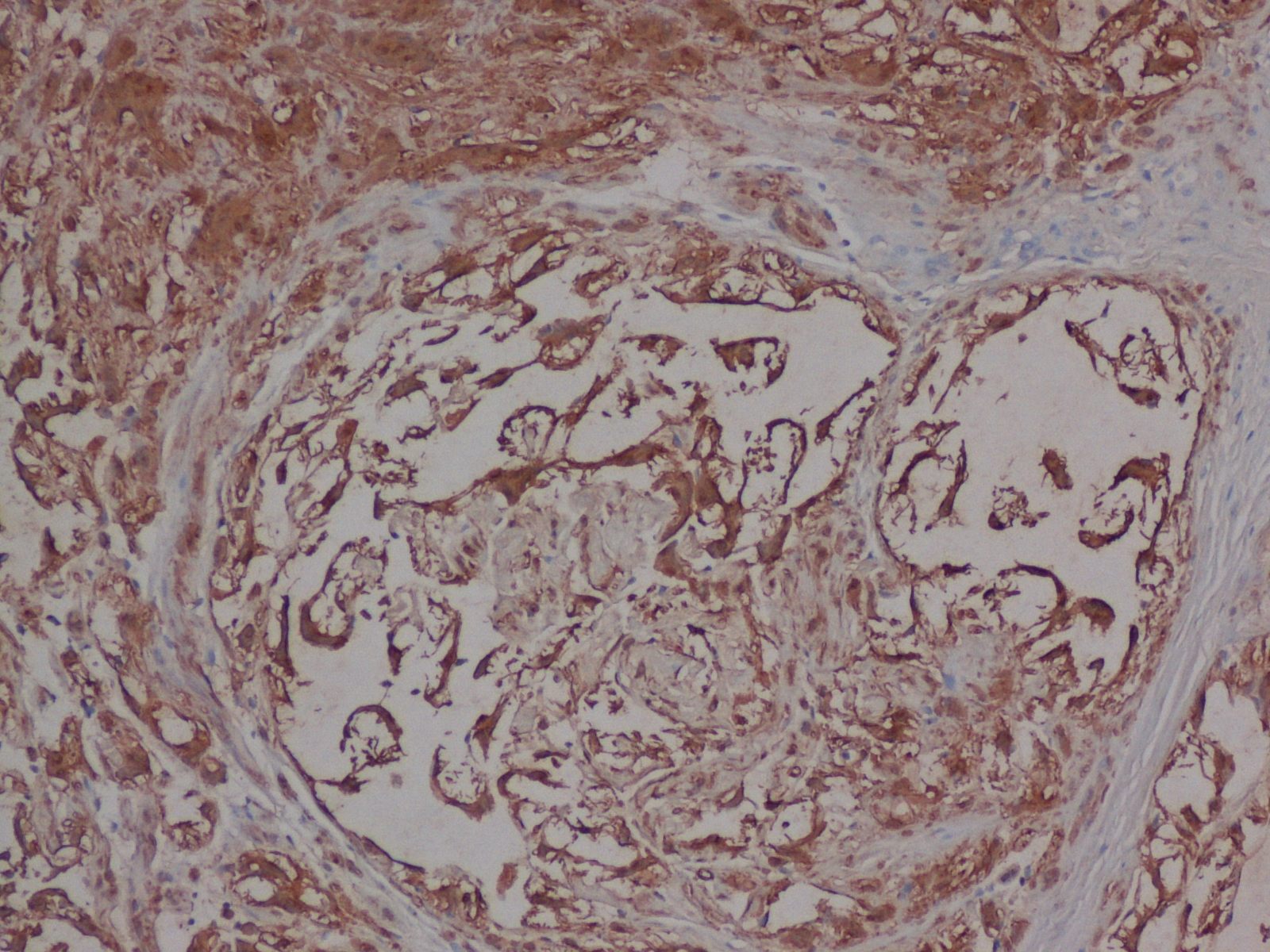
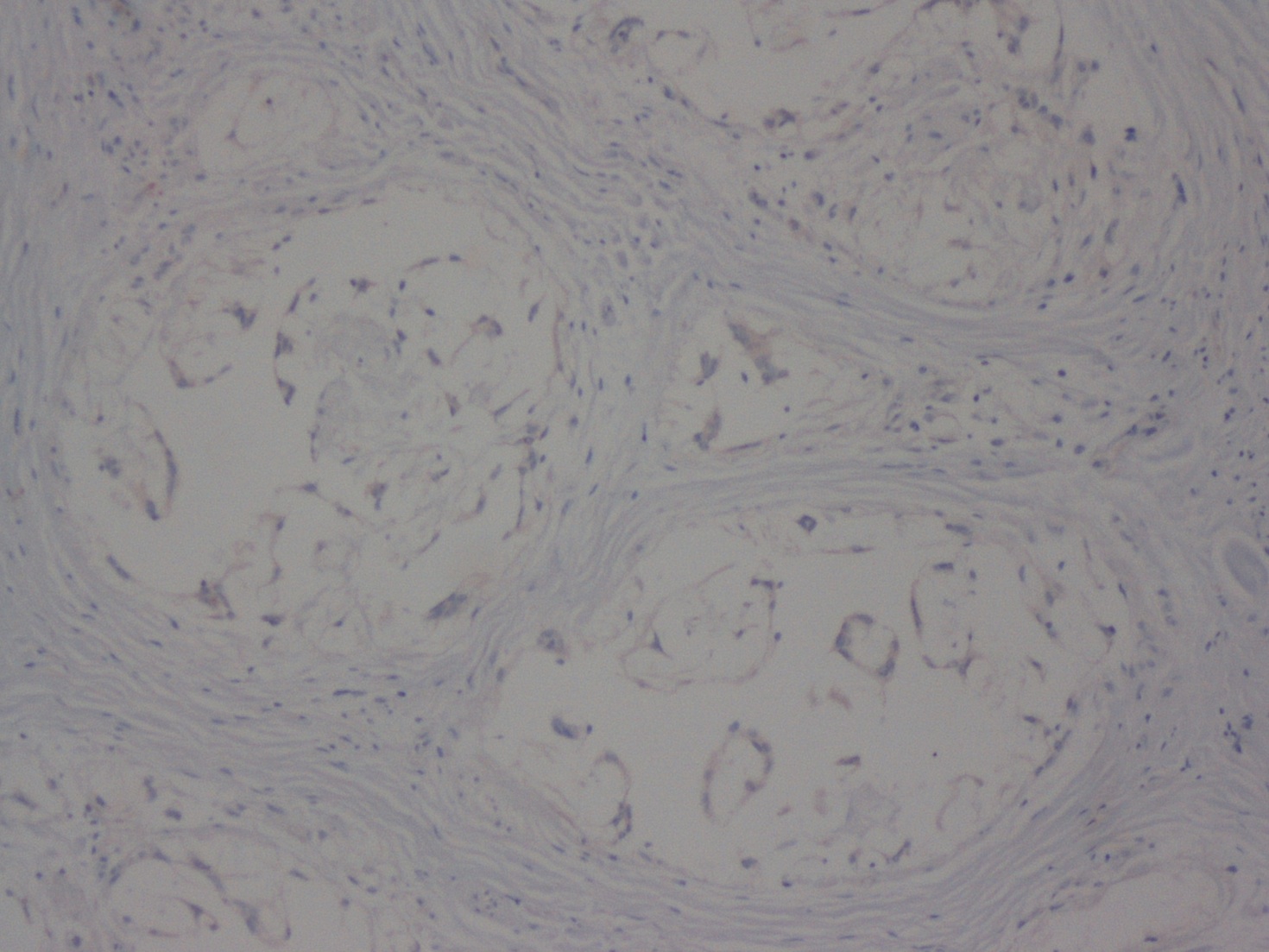
Left to right: S100, S100 high power, AE1 / AE3
Discussion:
In Case #1, the lesion is poorly circumscribed and composed of benign squamous epithelium overlying multiple lobules of spindled cells embedded in a basophilic myxoid stroma. Occasional syncytial-like aggregates are present. The spindle cells are present at the deep margins. They are strongly S100+, positive for NSE and weakly positive for EMA in the perineural cells.
Case #2 shows a circumscribed tumor composed also of multiple lobules of myxoid material with a collagenous septa. The tumor cells are spindled and strongly positive for S100 and negative for cytokeratin AE1 / AE3.
Nerve sheath myxomas are rare, distinct tumors of the peripheral nerve sheath, with a peak incidence in the 30's (Am J Surg Pathol 2005;29:1615). Patients present with solitary, superficial, multinodular, painless masses up to 2.5 cm, usually in the extremities. Tumors are typically slow growing and often were present for years before being resected. They typically involve the dermis or subcutis, forming multinodular, avascular masses with abundant myxoid matrix and a peripheral fibrous border. Epithelioid Schwann cells are present in corded, nested or syncytial-like aggregates. Stellate Schwann cells with cytoplasmic nuclear invaginations are also present.
The Schwann cells are strongly immunoreactive for S100 protein, GFAP, NSE and CD57. Occasional EMA+ perineurial cells are usually present, primarily in fibrous tissue. There are few / no mitotic figures.
The differential diagnosis includes low grade myxofibrosarcoma, which typically occurs in the elderly, has MFH-like areas, curvilinear vessels (thick walled with a broad arc) with condensation of cells around the vessels and often nonspecific cytogenetic aberrations. Neurothekeomas may have a myxoid stroma, but are distinct lesions by differential gene expression profiles and immunohistochemistry and thought to be a variant of fibrous histiocytoma (Mod Pathol 2011;24:343).
Complete excision is adequate treatment and even cellular cases have an indolent behavior with complete excision. However, most nerve sheath myxomas are managed by simple excision, leading to positive margins and frequent local recurrence.
