
1 August 2012 - Case #247
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. M. Rizwan Bashir, Aga Khan University Hospital, Karachi, Pakistan, for contributing this case.
Advertisement
Case #247
Clinical history:
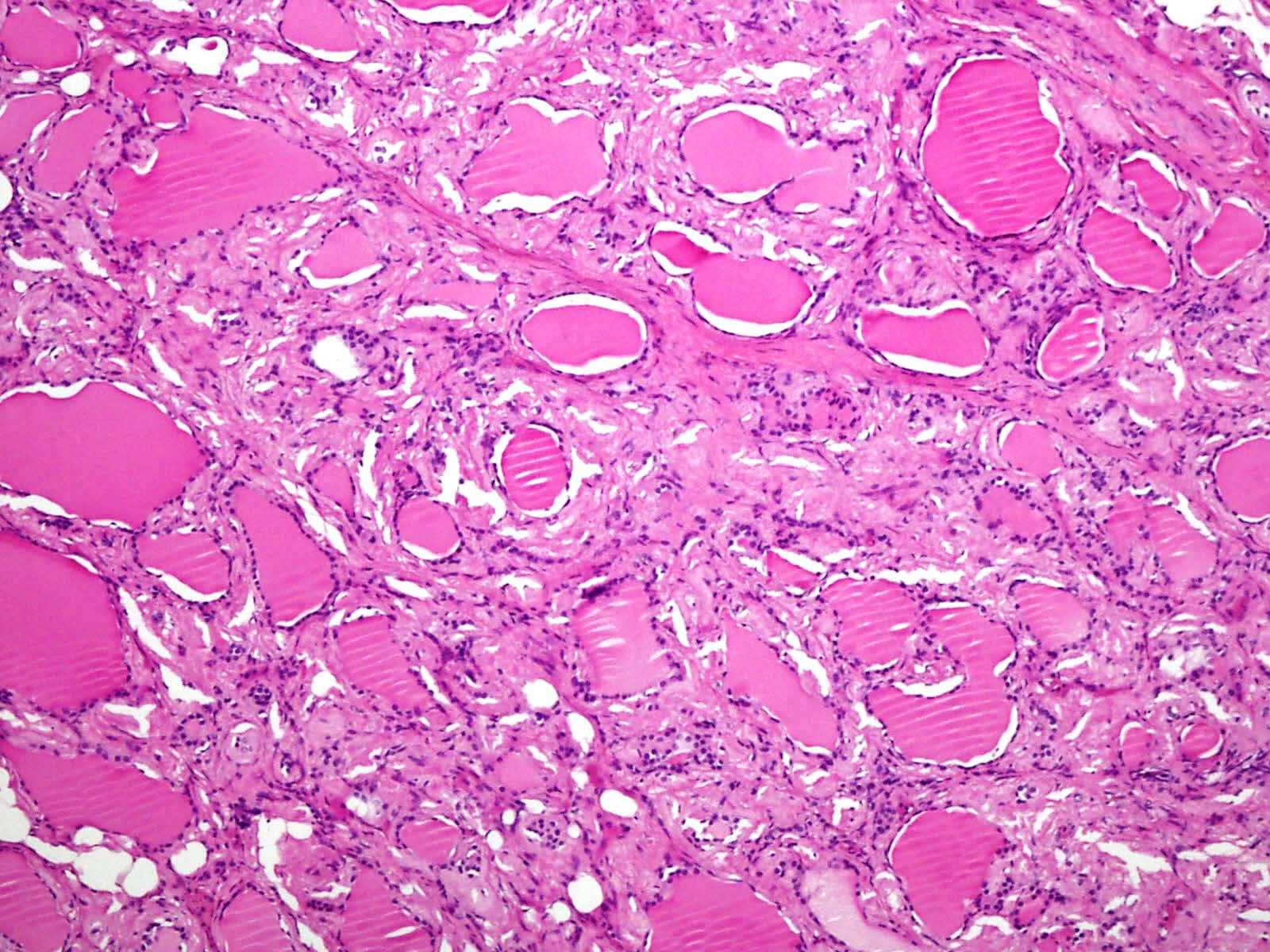
A 61 year old woman with hypertension had a diffusely enlarged thyroid gland with the clinical impression of a multinodular goiter. A complete thyroidectomy was performed.
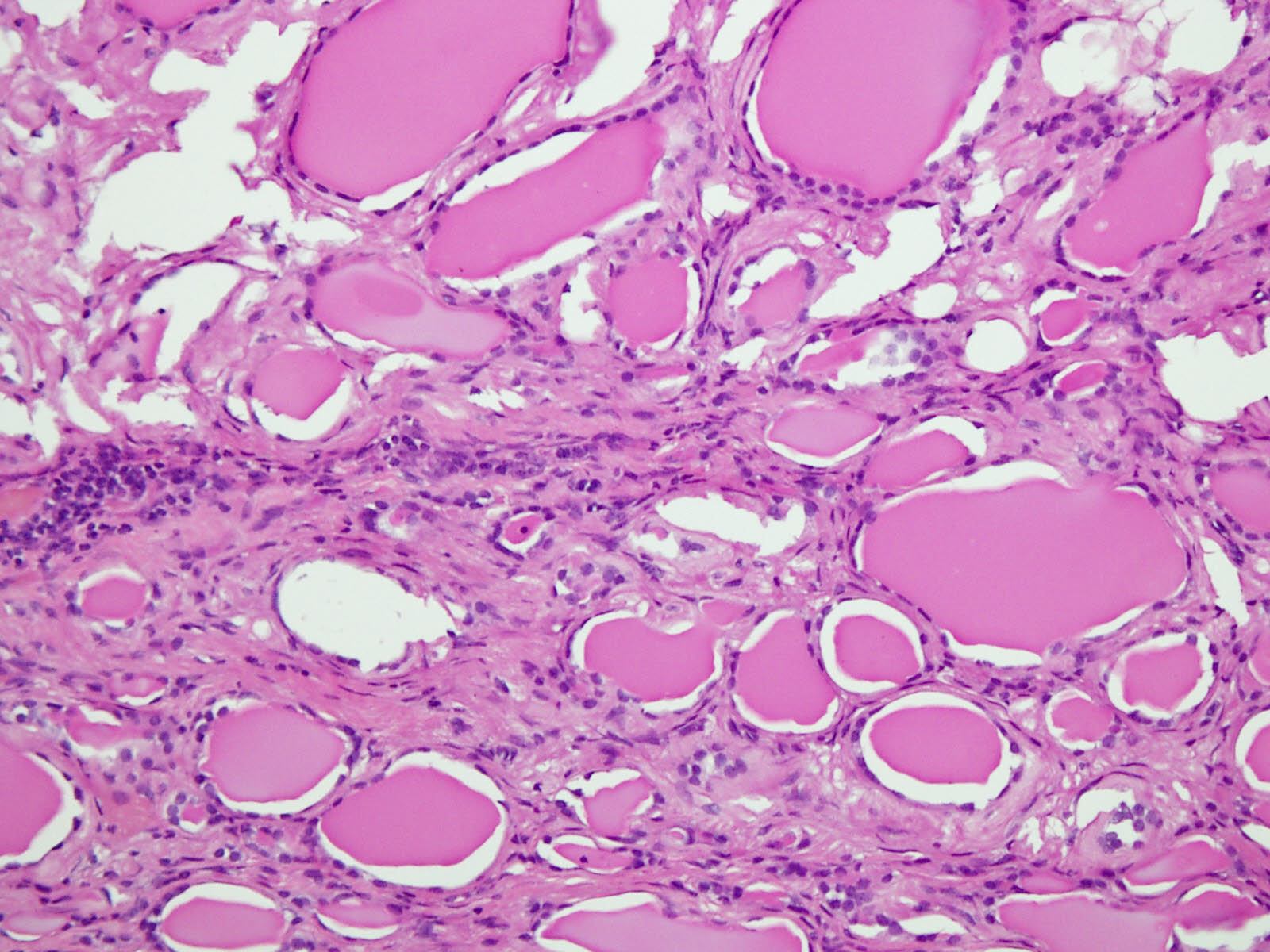
Microscopic images:

What is your diagnosis?
Diagnosis: Amyloid goiter
Immunostains:

Discussion:
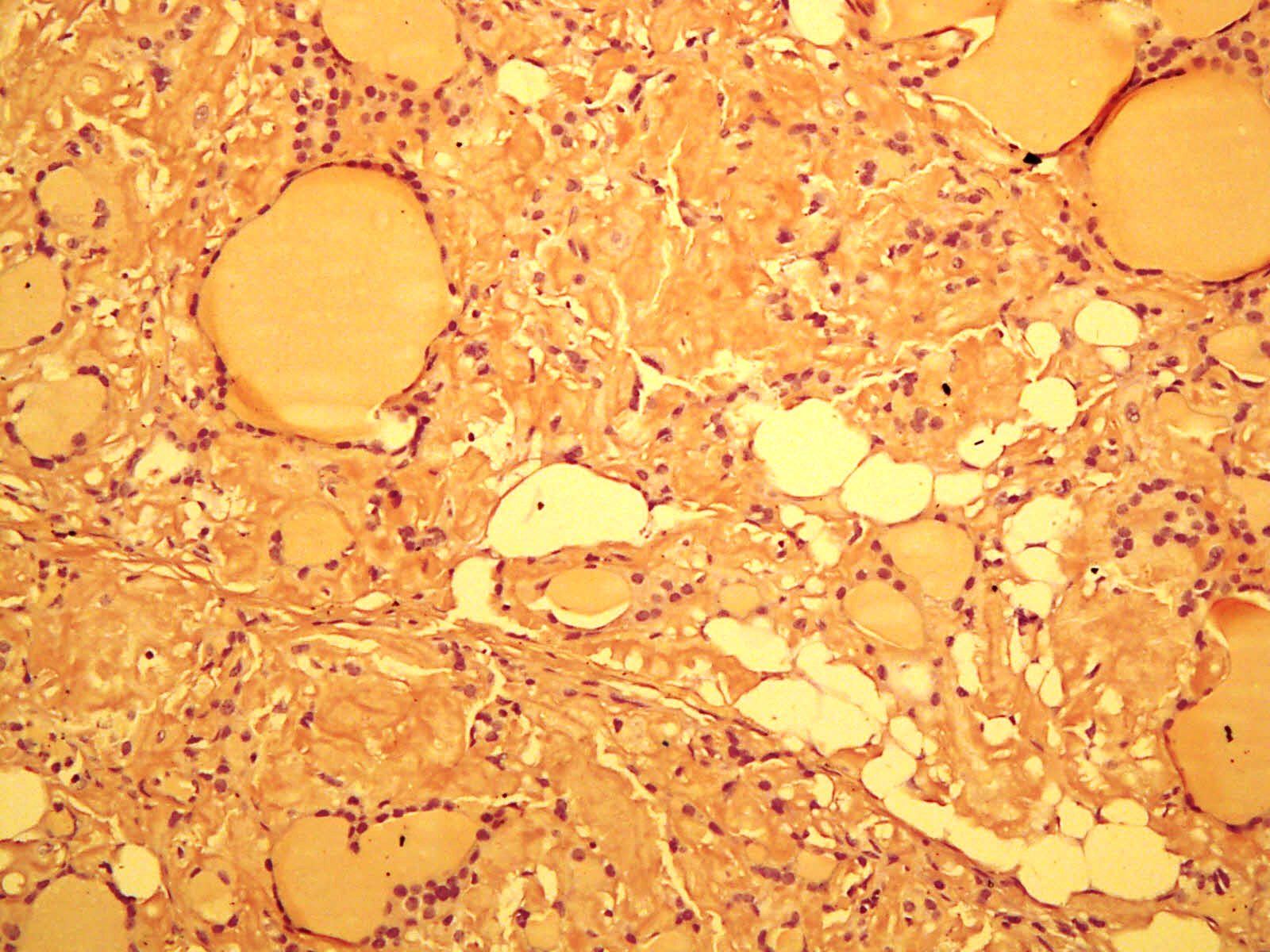
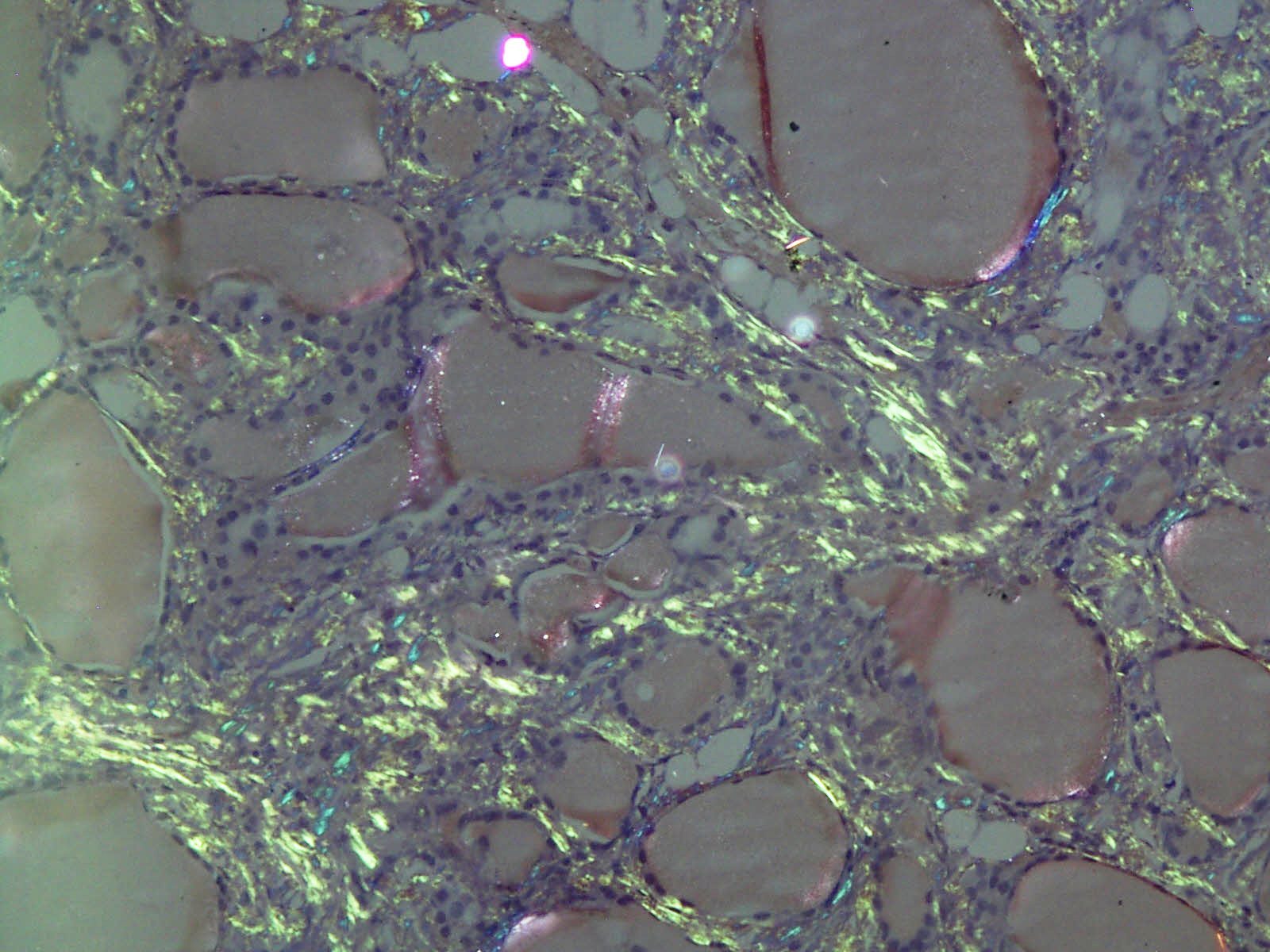
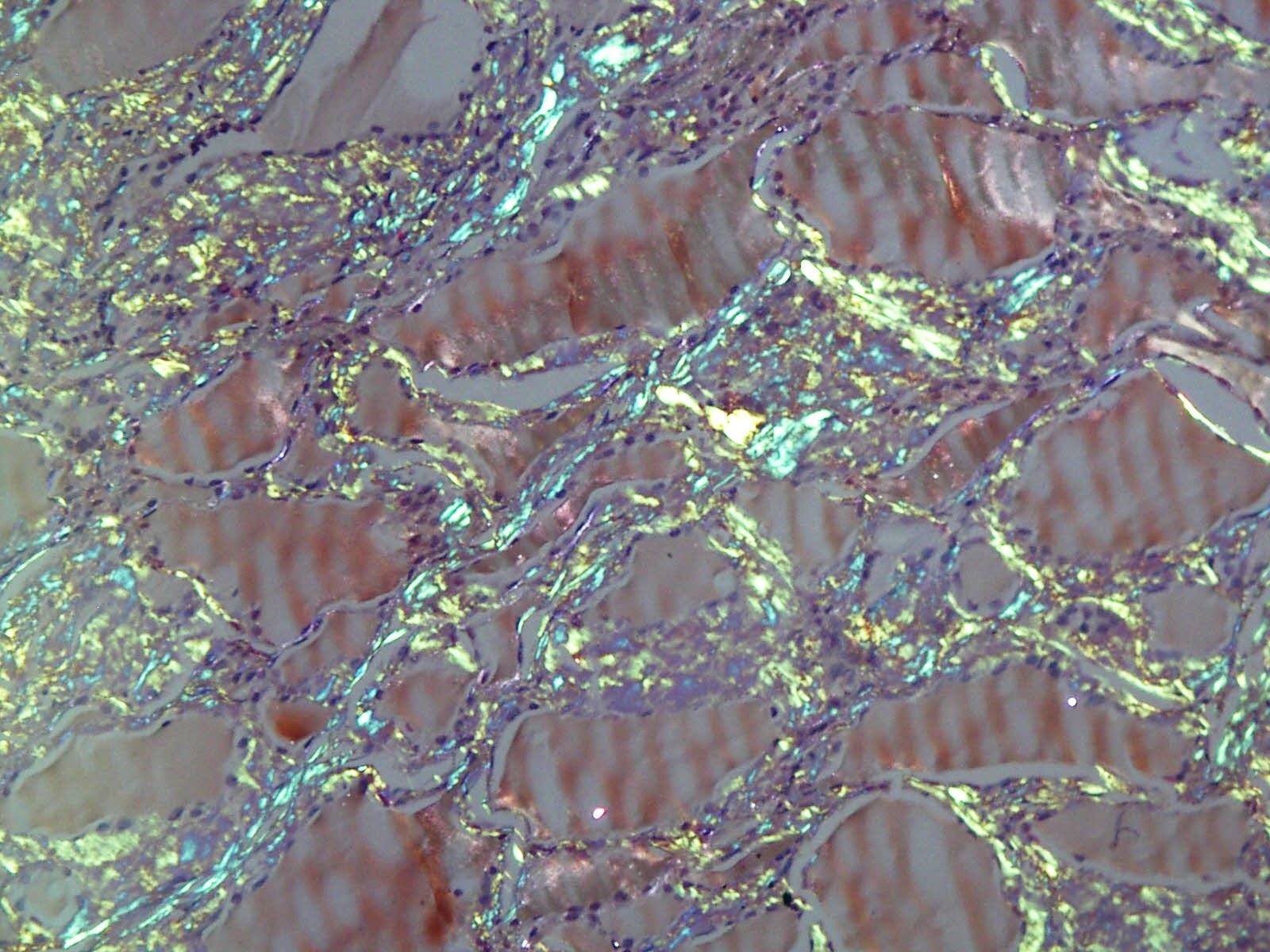
The amyloid stains with Congo red and Sirius red and showed apple-green birefringence under polarized microscopy.
Amyloid goiter is an uncommon disease of amyloid deposits in the thyroid gland associated with goiter. The median patient age is 54 years but all adults can be affected (Am J Clin Pathol 1995;104:306). It is usually due to primary or secondary AA type amyloidosis but other causes have been reported (Amyloid 2012;19:161). Clinically, there is enlargement of the thyroid over several months that may cause respiratory distress but thyroid function is usually normal. Diagnosis can often be made by fine needle aspiration (Cytopathology 2006;17:262). Occasionally, diagnosis is not made until autopsy.
Grossly, the thyroid is enlarged and white-tan. Histologically, there is diffuse amyloid deposition surrounding thyroid follicles, which may distort the thyroid architecture. Occasional features are foreign body giant cell reaction, fatty metaplasia, fatty infiltration, squamous metaplasia or focal lymphocytic thyroiditis. With the Congo red stain, the amyloid is salmon colored and demonstrates apple-green birefringence under polarized light.
The differential diagnosis includes medullary thyroid carcinoma, which has prominent amyloid but also calcitonin positive tumor cells.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. M. Rizwan Bashir, Aga Khan University Hospital, Karachi, Pakistan, for contributing this case.

Optimize your laboratory workflow with the
most powerful high-throughput slide scanner in anatomic pathology:
the VENTANA iScan HT scanner.
Transform your practice by delivering results faster with greater confidence:
Gain time each day
Improve workflow
Engage instant remote consultation
Enhanced slide scanning and viewing is only the beginning. The expanding
family of cutting-edge digital pathology solutions by Ventana empowers you to
deliver the right test, to the right patient, at the right time.
Don't lose another minute of productive time click here to
discover how the VENTANA iScan HT scanner can help you elevate the
standard of patient care.
Website news:
(1) Recent chapter updates:
(2) New Management Page articles include: Medicare Changes Enrollment Guidelines From 30 days to 60 days, by Leigh Polk, PSA, LLC and ACO's, Practice Buy-outs and Dj vu All over Again, by Mick Raich, Vachette Pathology.
Visit and follow our Blog to see recent updates to the website.
(1) Recent chapter updates:
- Prostate gland and seminal vesicles: by Ali Amin, M.D., Komal Arora, M.D., Gladell Paner, M.D. and Monika Roychowdhury, M.D.
- Kidney Tumor (adult malignant): by Sean Williamson, M.D.
- Liver and intrahepatic bile ducts-nontumor: by Komal Arora, M.D.
- Ovary-nontumor: by Mohiedean Ghofrani, M.D. and Shahidul Islam, M.D.
(2) New Management Page articles include: Medicare Changes Enrollment Guidelines From 30 days to 60 days, by Leigh Polk, PSA, LLC and ACO's, Practice Buy-outs and Dj vu All over Again, by Mick Raich, Vachette Pathology.
Visit and follow our Blog to see recent updates to the website.
Case #247
Clinical history:
A 61 year old woman with hypertension had a diffusely enlarged thyroid gland with the clinical impression of a multinodular goiter. A complete thyroidectomy was performed.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Amyloid goiter
Immunostains:
Discussion:
The amyloid stains with Congo red and Sirius red and showed apple-green birefringence under polarized microscopy.
Amyloid goiter is an uncommon disease of amyloid deposits in the thyroid gland associated with goiter. The median patient age is 54 years but all adults can be affected (Am J Clin Pathol 1995;104:306). It is usually due to primary or secondary AA type amyloidosis but other causes have been reported (Amyloid 2012;19:161). Clinically, there is enlargement of the thyroid over several months that may cause respiratory distress but thyroid function is usually normal. Diagnosis can often be made by fine needle aspiration (Cytopathology 2006;17:262). Occasionally, diagnosis is not made until autopsy.
Grossly, the thyroid is enlarged and white-tan. Histologically, there is diffuse amyloid deposition surrounding thyroid follicles, which may distort the thyroid architecture. Occasional features are foreign body giant cell reaction, fatty metaplasia, fatty infiltration, squamous metaplasia or focal lymphocytic thyroiditis. With the Congo red stain, the amyloid is salmon colored and demonstrates apple-green birefringence under polarized light.
The differential diagnosis includes medullary thyroid carcinoma, which has prominent amyloid but also calcitonin positive tumor cells.
