
17 May 2012 - Case #242
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Eman Abdelzaher, Alexandria Faculty of Medicine (Egypt), for contributing this case and the discussion.
Advertisement
Case #242
Clinical history:
A 39 year old woman presented with headache. CT showed a 6.5 x 6 x 4 cm extra-axial dural-based lesion at the right temporoparietal region. Intense homogenous postcontrast enhancement was noted. The lesion exerted mass effects on the surrounding structures. Underlying bone showed mild hyperostosis. Gross total removal was performed.
Macroscopic examination showed multiple soft tissue fragments (10 x 8 x 3 cm in aggregate) were bluish with a gelatinous appearance.
Microscopic images:
What is your diagnosis?
Diagnosis: Chordoid meningioma, WHO grade II
Immunostains:
Discussion:
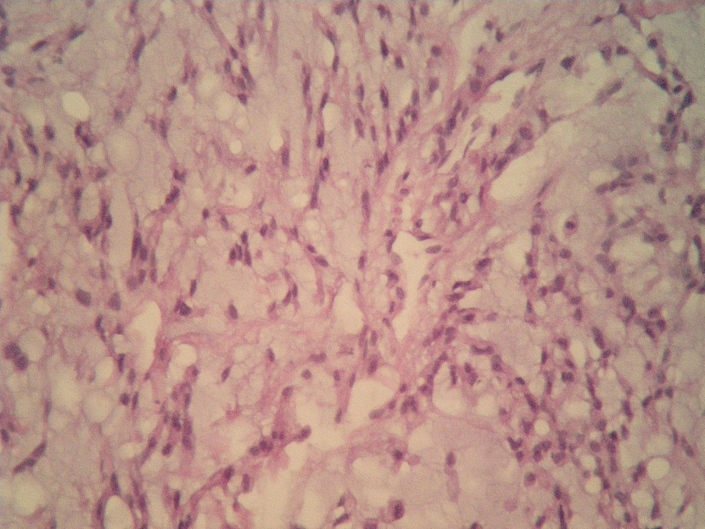
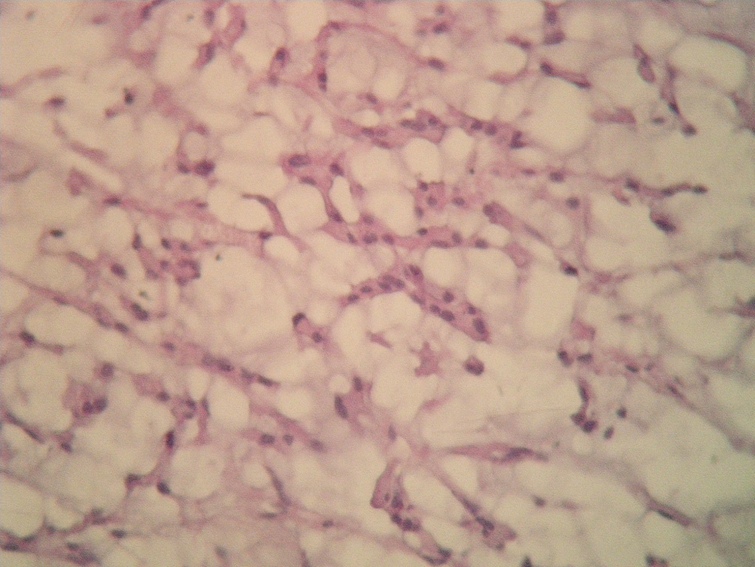
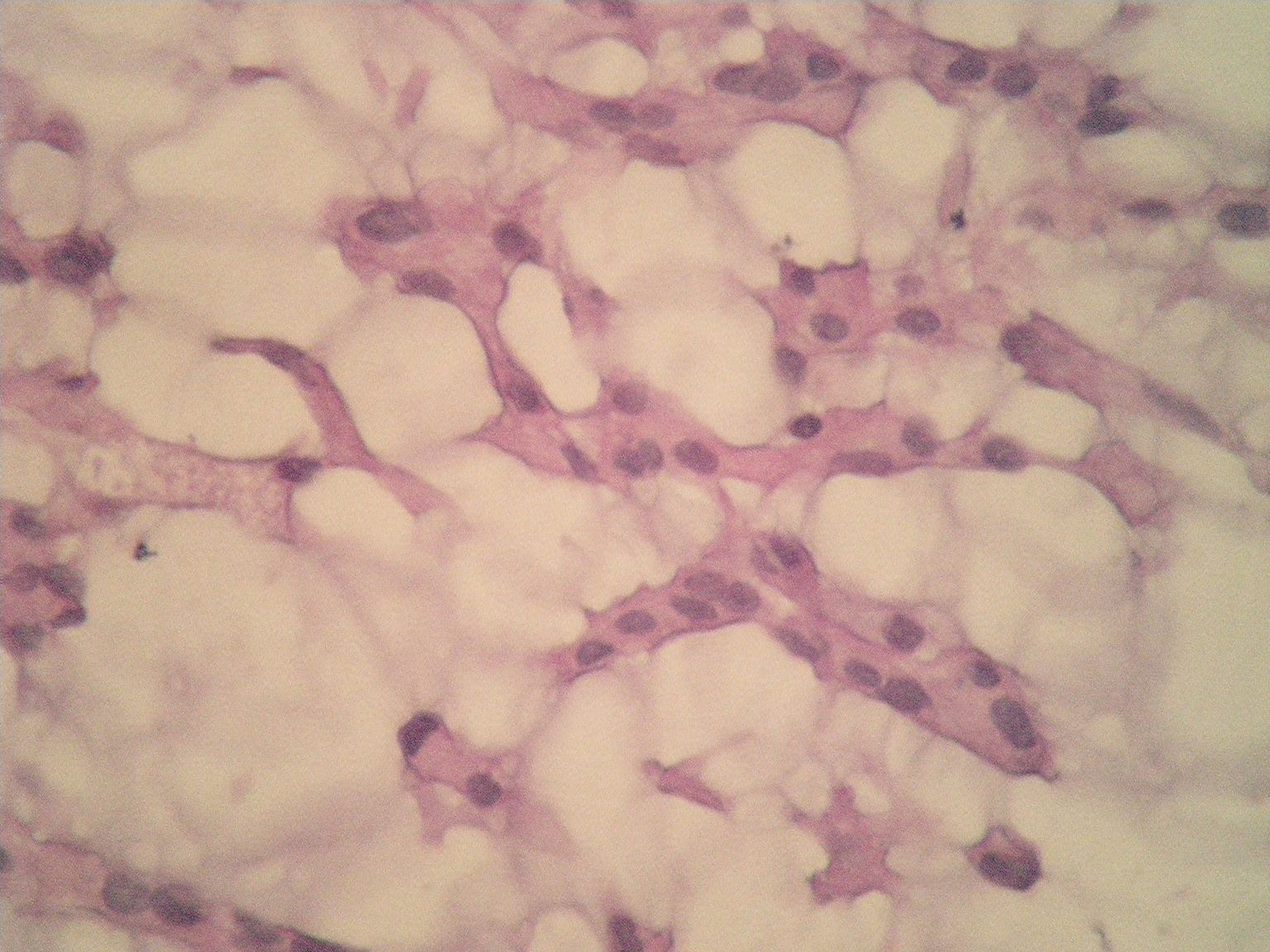
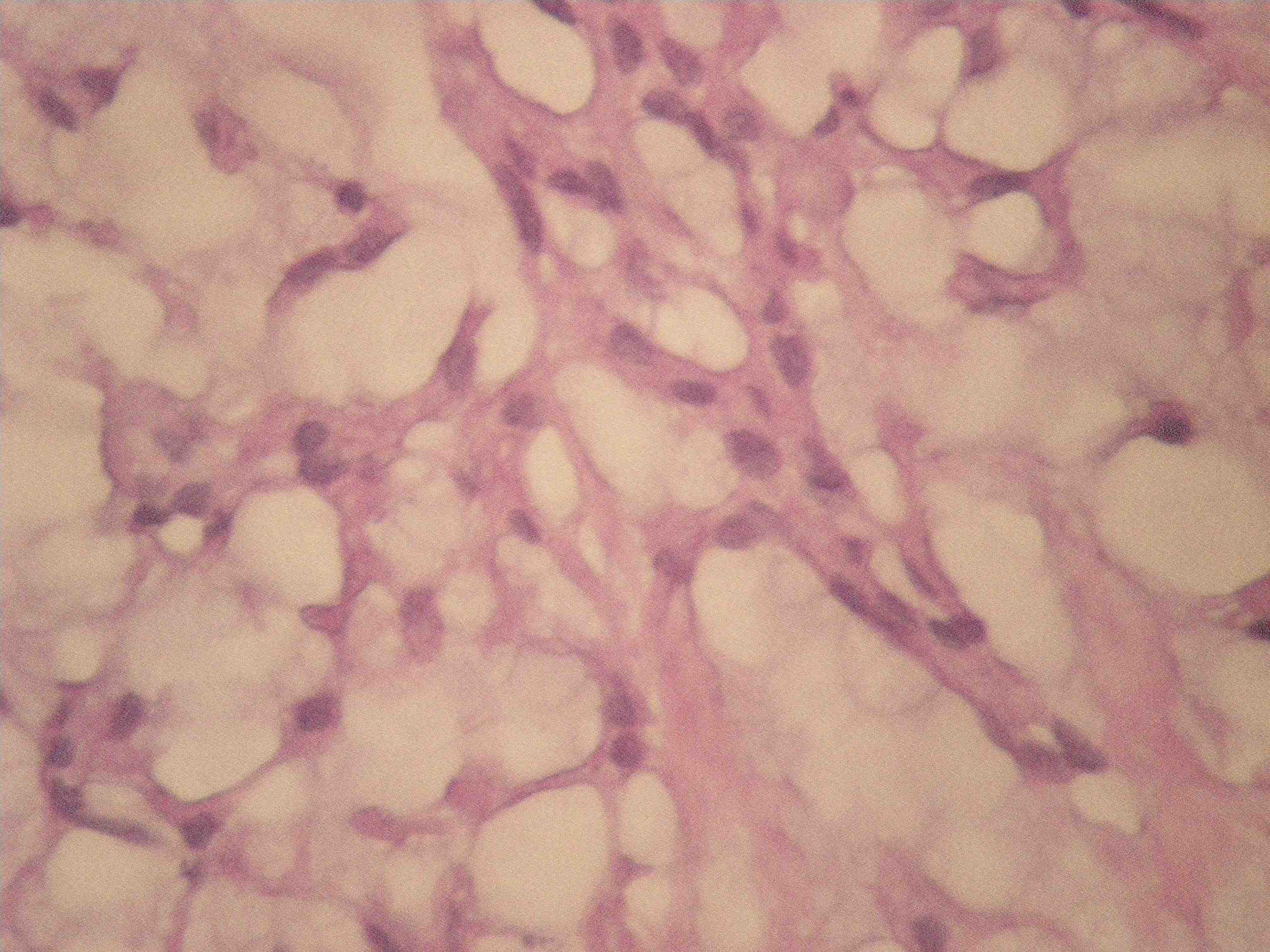
Histology revealed cords of epithelioid cells surrounded by abundant blue mucoid stroma. The cells had eosinophilic cytoplasm and small hyperchromatic nuclei without prominent nucleoli. There was no brain invasion, no lymphoplasmacytic infiltrate, no mitotic activity and no necrosis. Immunohistochemistry showed membranous staining for EMA, negative staining for S100 and rare positive CK staining.
This case is an extra-axial dural-based enhancing supratentorial lesion in a 39 year old woman associated with hyperostosis. These features raise the possibility of meningioma but the tumor had chordoid features and did not look like a classic meningioma at macroscopic or microscopic examination.
The differential diagnosis of CNS lesions with chordoid features includes:
Achieving the correct diagnosis requires correlation with clinicoradiological data and adequate sampling. Immunohistochemistry is also helpful.
In this case, the supratentorial extra-axial location, bone hyperostosis and immunohistochemical results were all in favor of chordoid meningioma. According to the WHO classification of CNS tumors (2007), chordoid meningiomas are assigned to grade II.
Chordoid meningioma was first described by Kepes et al. in 1988. In their study, all 7 patients were < 20 years of age and the tumors were associated with a dense lymphoplasmacytic infiltrate. These patients had preoperative manifestations of Castleman disease and their hematologic abnormalities normalized following excision. Subsequent studies did not confirm the association with Castleman disease nor its preferred occurrence in young patients. Our case did not present with any hematological abnormality. An unbalanced translocation t(1;3)(p12-13;q11) has been reported in chordoid meningiomas and may serve as a potential diagnostic aid in the future.
Histologically, chordoid meningiomas resemble chordoma. They uncommonly occur in a pure form. More frequently, they have predominant chordoma-like areas coexisting with areas of typical meningioma.
In conclusion, chordoid meningioma, WHO grade II, is an uncommon variant of meningioma with an increased likelihood of recurrence. Therefore, recognition of this entity is important and its distinction from cases that show overlapping morphological features is essential.
References: IARC: WHO Classification of Tumours of the Central Nervous System, 4th Edition, 2007, Cancer 1988;62:391, Genes Chromosomes Cancer 1999;26:270
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Eman Abdelzaher, Alexandria Faculty of Medicine (Egypt), for contributing this case and the discussion.

A new Mouse on Mouse IHC kit (ab127055) offering you:
• The freedom and peace of mind to stain mouse tissues using mouse antibodies with no background from endogenous IgG
• Confidence to produce publication quality images the first time with a sensitive polymer detection system
• The flexibility to study biotin containing tissues with a biotin-free detection system
• Easy staining experiments with a simple and reproducible protocol
Further enhance your staining experiments with EXPOSE IHC detection systems offering reduced background and greater sensitivity than polymer detection systems. In addition, discover extensive resources (click here) to troubleshoot your IHC experiments.
Website news:
(1) Our Feature Page for the month highlights Computer software and systems and includes Milestone Medical and Voicebrook.
(2) We are constantly looking for new Reviewers for our 7,000 topics, which we want to update every 1-2 years. Visit our newly updated Author Instructions page for more information.
(3) The Table of Contents of our Stains chapter now includes all 360 stains / biomarkers described in the chapter. The CD Markers chapter contains an additional 260 markers. We update these pages regularly but let us know of any new markers we should include or other changes we should make.
Visit and follow our Blog to see recent updates to the website.
(1) Our Feature Page for the month highlights Computer software and systems and includes Milestone Medical and Voicebrook.
(2) We are constantly looking for new Reviewers for our 7,000 topics, which we want to update every 1-2 years. Visit our newly updated Author Instructions page for more information.
(3) The Table of Contents of our Stains chapter now includes all 360 stains / biomarkers described in the chapter. The CD Markers chapter contains an additional 260 markers. We update these pages regularly but let us know of any new markers we should include or other changes we should make.
Visit and follow our Blog to see recent updates to the website.
Case #242
Clinical history:
A 39 year old woman presented with headache. CT showed a 6.5 x 6 x 4 cm extra-axial dural-based lesion at the right temporoparietal region. Intense homogenous postcontrast enhancement was noted. The lesion exerted mass effects on the surrounding structures. Underlying bone showed mild hyperostosis. Gross total removal was performed.
Macroscopic examination showed multiple soft tissue fragments (10 x 8 x 3 cm in aggregate) were bluish with a gelatinous appearance.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Chordoid meningioma, WHO grade II
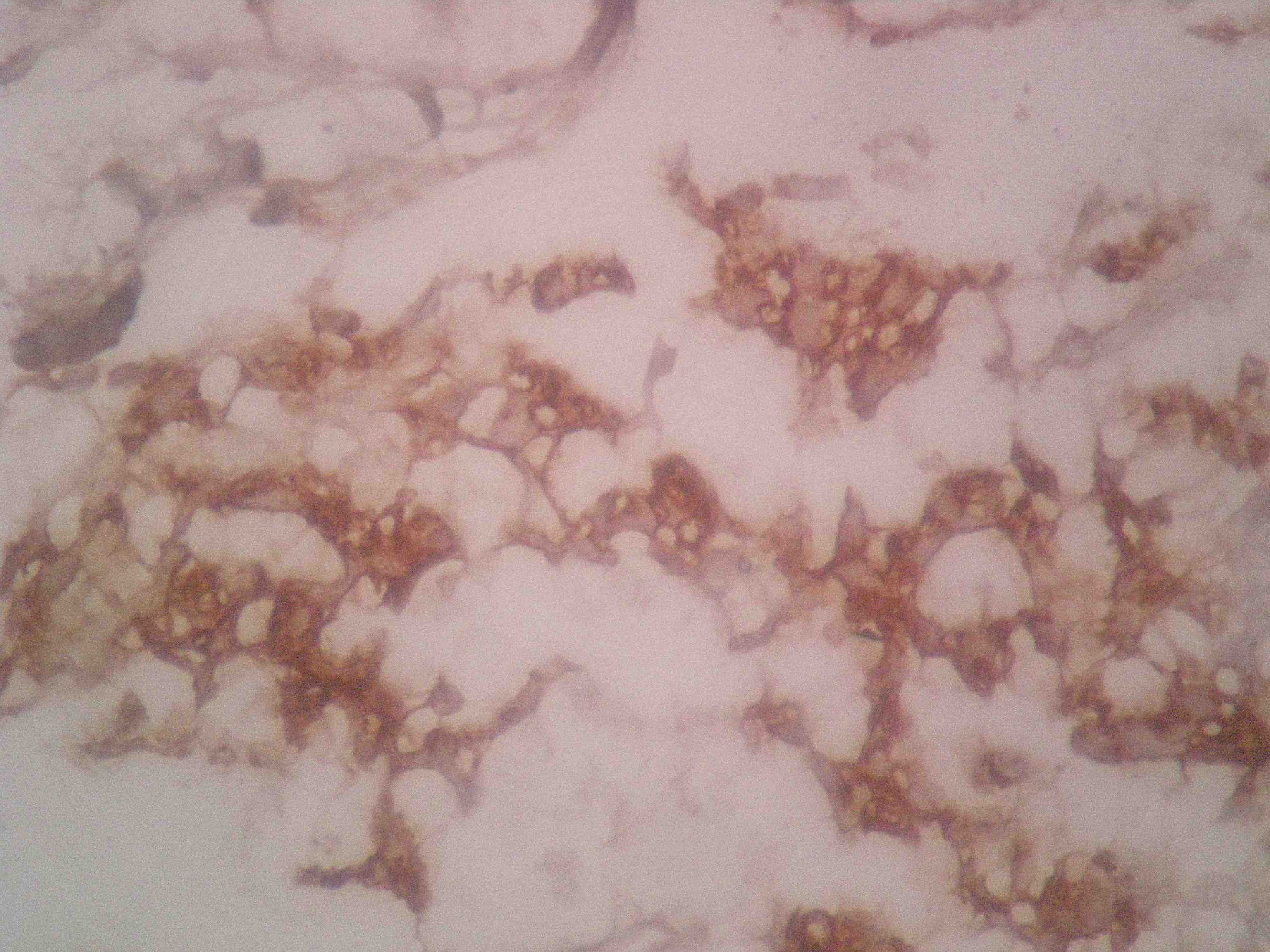
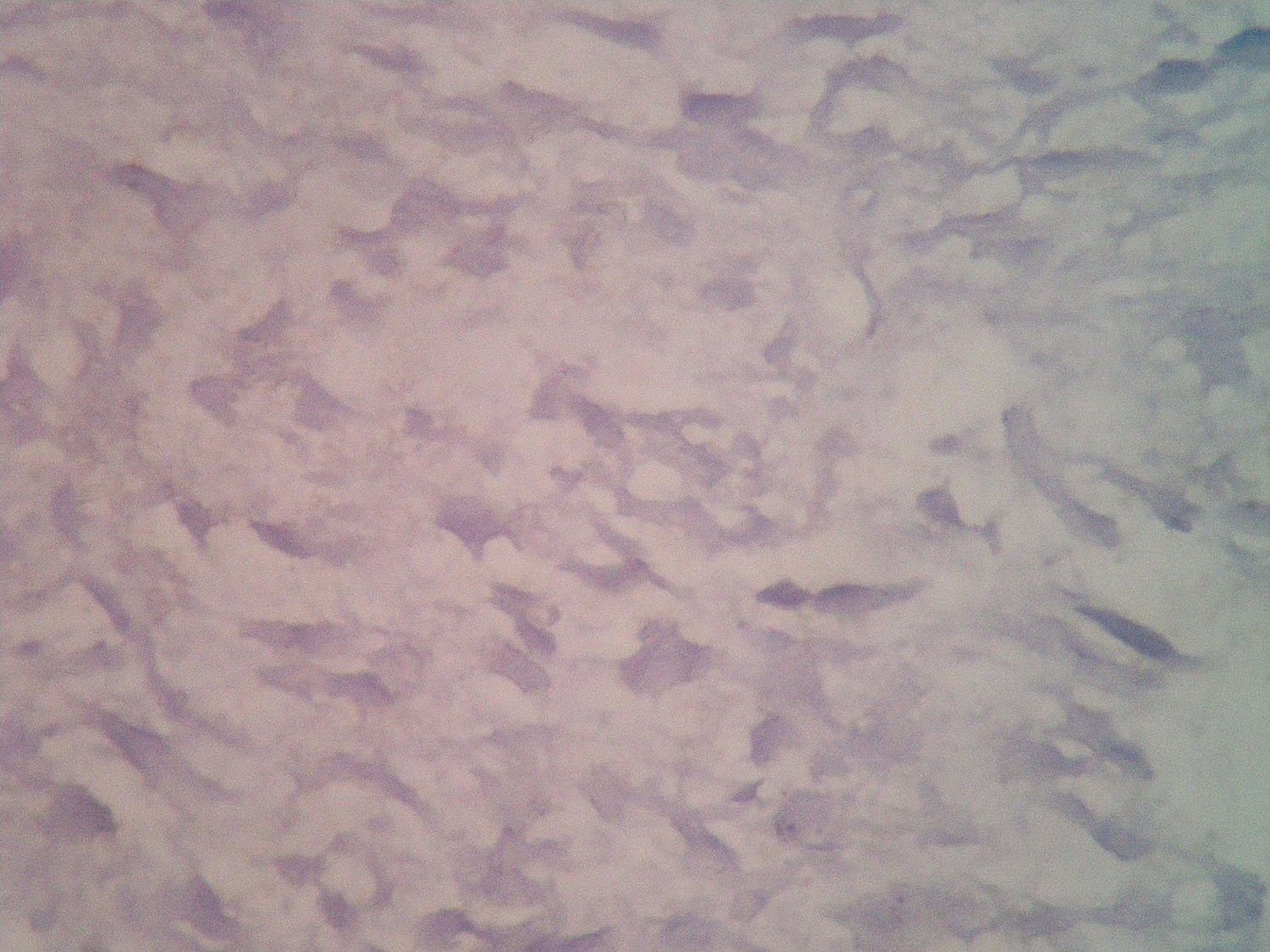
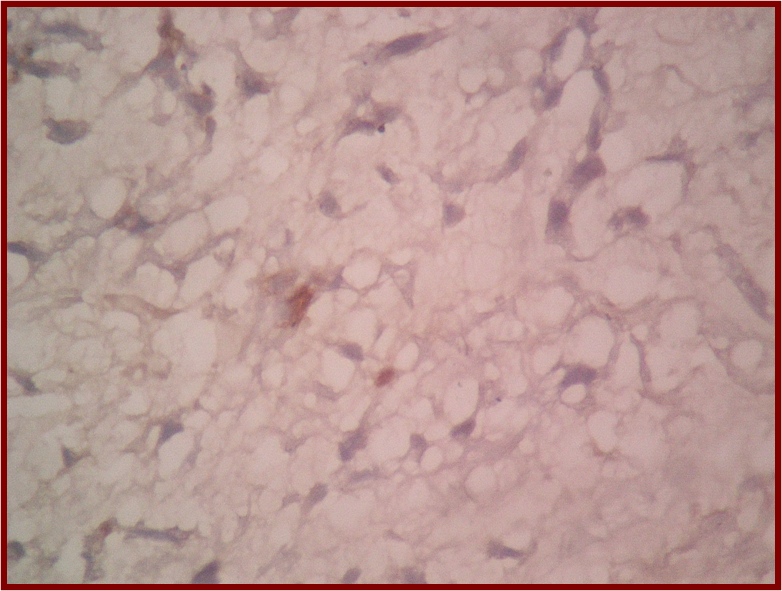
Immunostains:
Left to right: EMA, S100, cytokeratin
Discussion:
Histology revealed cords of epithelioid cells surrounded by abundant blue mucoid stroma. The cells had eosinophilic cytoplasm and small hyperchromatic nuclei without prominent nucleoli. There was no brain invasion, no lymphoplasmacytic infiltrate, no mitotic activity and no necrosis. Immunohistochemistry showed membranous staining for EMA, negative staining for S100 and rare positive CK staining.
This case is an extra-axial dural-based enhancing supratentorial lesion in a 39 year old woman associated with hyperostosis. These features raise the possibility of meningioma but the tumor had chordoid features and did not look like a classic meningioma at macroscopic or microscopic examination.
The differential diagnosis of CNS lesions with chordoid features includes:
- Chordoma: intracranial lesions that straddle the midline and erode the clivus, EMA+, CK+, S100+ (50%)
- Chordoid meningioma: EMA+, focal or negative CK, S100-, GFAP-
- Myxoid chondrosarcoma: S100+, EMA-, CK-
- Chordoid glioma of the third ventricle: located at third ventricle, GFAP+
- Metastatic mucinous carcinoma: known primary, anaplasia, diffuse CK+ and EMA+
- Glioblastoma: GFAP+
- Atypical teratoid / rhabdoid tumor: infants, posterior fossa lesion, INI1- with positive control of blood vessels and lymphocytes
- Epithelioid hemangioendothelioma: intracytoplasmic lumina, CD31+
- Meningioma with myxoid degeneration: no epithelioid cells
- Schwannoma with myxoid degeneration: S100+, EMA-, CK
Achieving the correct diagnosis requires correlation with clinicoradiological data and adequate sampling. Immunohistochemistry is also helpful.
In this case, the supratentorial extra-axial location, bone hyperostosis and immunohistochemical results were all in favor of chordoid meningioma. According to the WHO classification of CNS tumors (2007), chordoid meningiomas are assigned to grade II.
Chordoid meningioma was first described by Kepes et al. in 1988. In their study, all 7 patients were < 20 years of age and the tumors were associated with a dense lymphoplasmacytic infiltrate. These patients had preoperative manifestations of Castleman disease and their hematologic abnormalities normalized following excision. Subsequent studies did not confirm the association with Castleman disease nor its preferred occurrence in young patients. Our case did not present with any hematological abnormality. An unbalanced translocation t(1;3)(p12-13;q11) has been reported in chordoid meningiomas and may serve as a potential diagnostic aid in the future.
Histologically, chordoid meningiomas resemble chordoma. They uncommonly occur in a pure form. More frequently, they have predominant chordoma-like areas coexisting with areas of typical meningioma.
In conclusion, chordoid meningioma, WHO grade II, is an uncommon variant of meningioma with an increased likelihood of recurrence. Therefore, recognition of this entity is important and its distinction from cases that show overlapping morphological features is essential.
References: IARC: WHO Classification of Tumours of the Central Nervous System, 4th Edition, 2007, Cancer 1988;62:391, Genes Chromosomes Cancer 1999;26:270
