
11 May 2012 - Case #241
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Saroona Haroon, The Aga Khan University Hospital (Pakistan), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case #241
Clinical history:
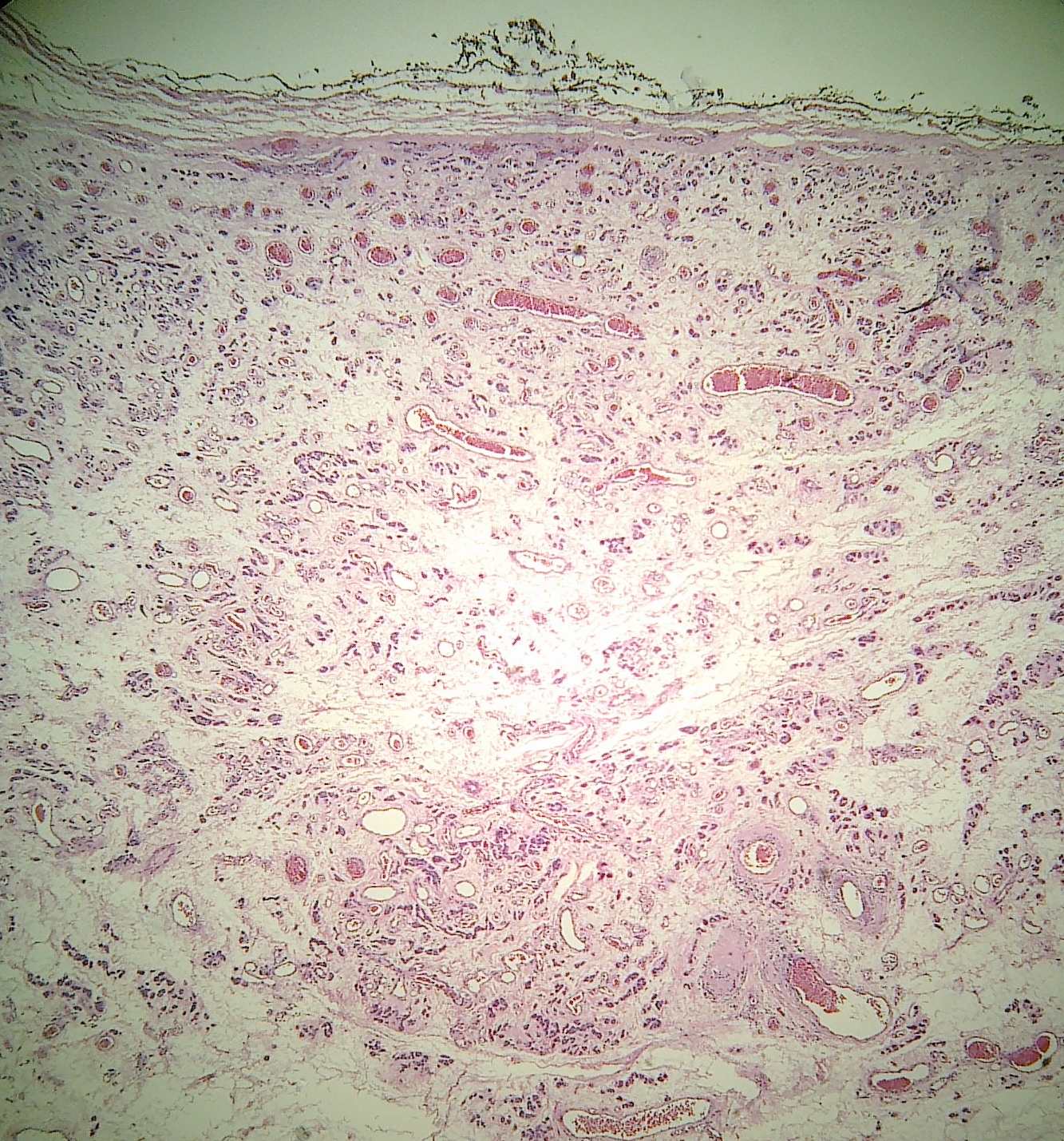
A 30 year old Asian woman presented with painless vulval swelling for the past 7 months. Clinically, it was diagnosed as a Bartholin cyst. At excision, the swelling was 2 cm, circumscribed and firm.
Microscopic images:

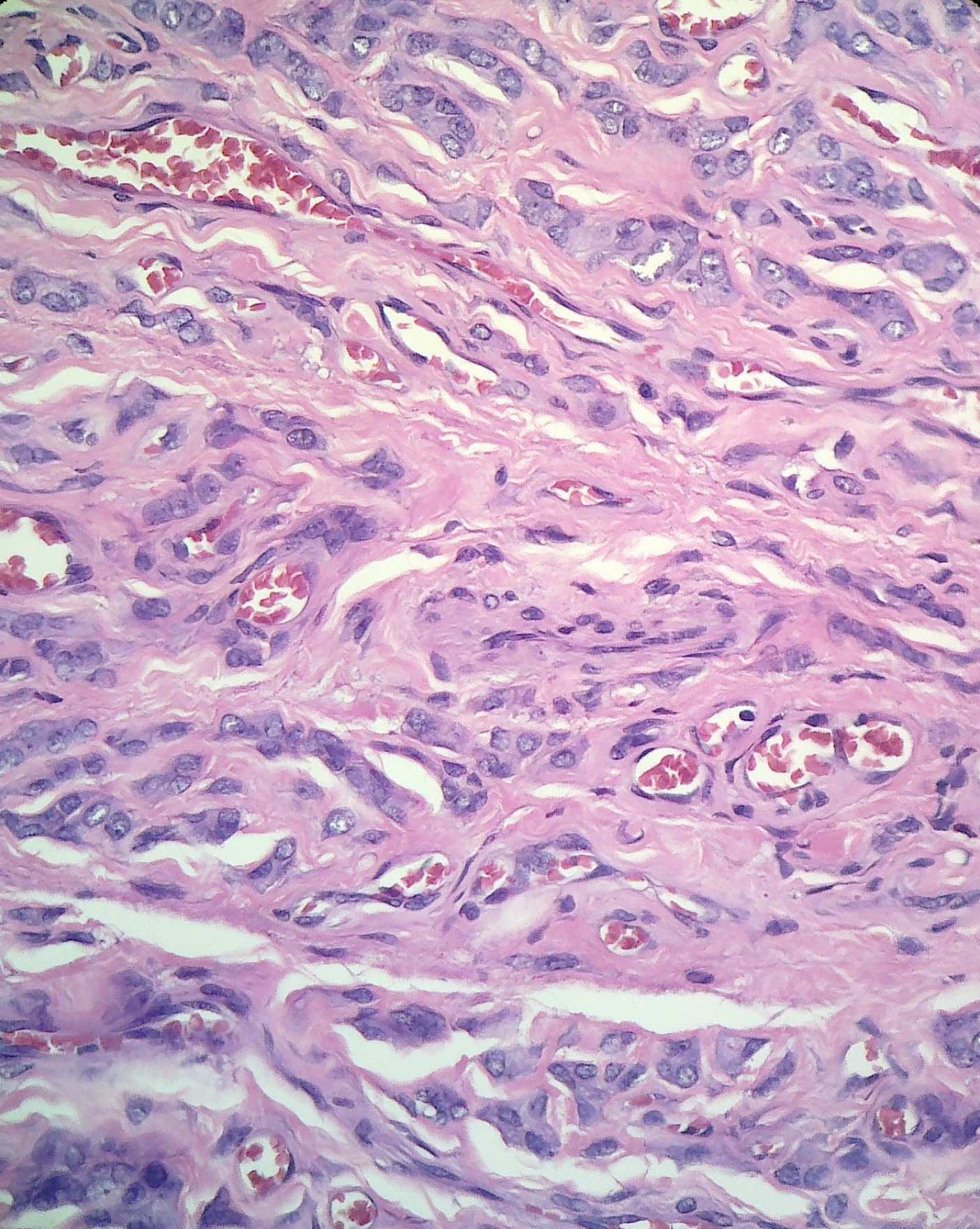
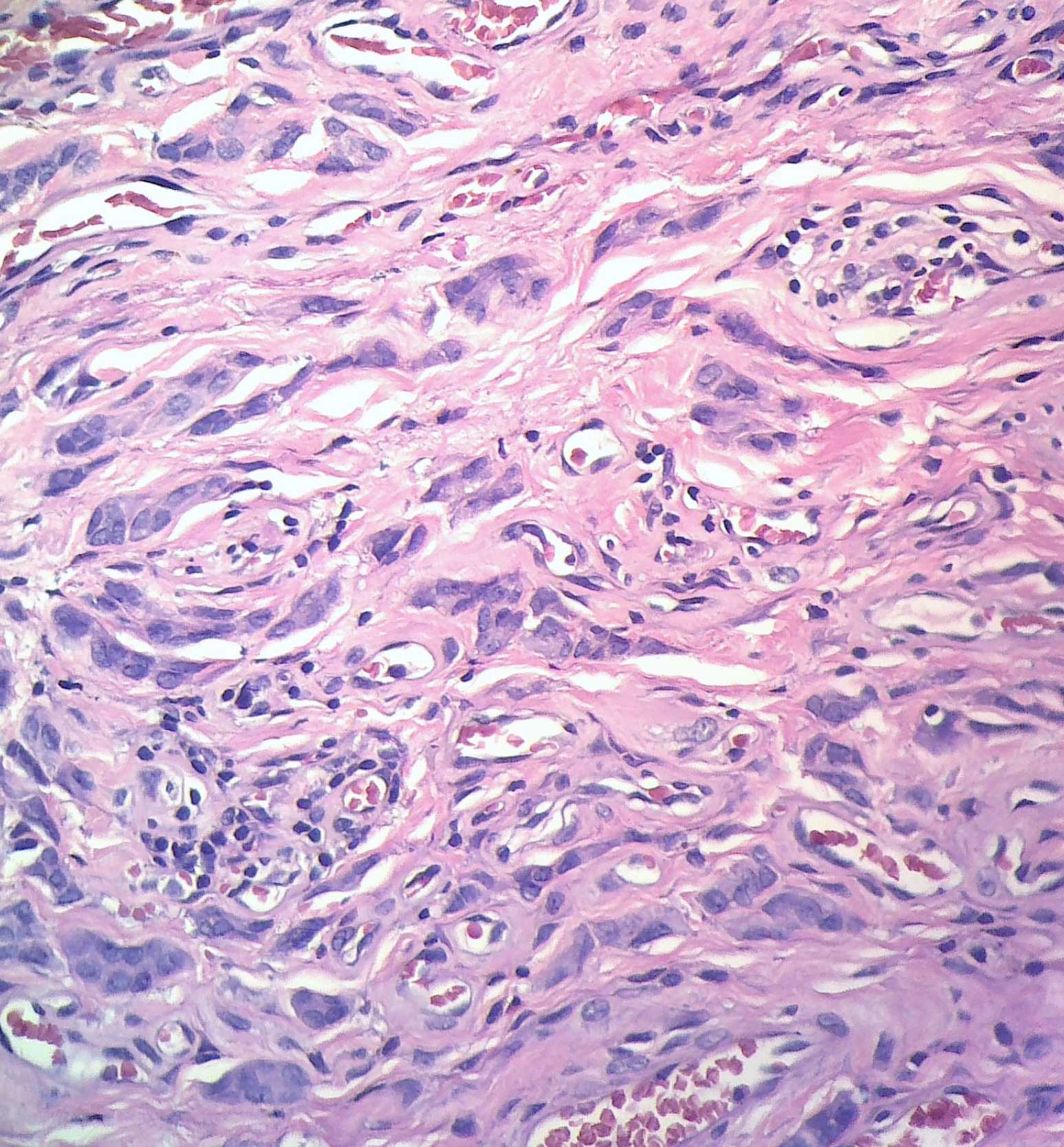
What is your diagnosis?
Diagnosis: Angiomyofibroblastoma
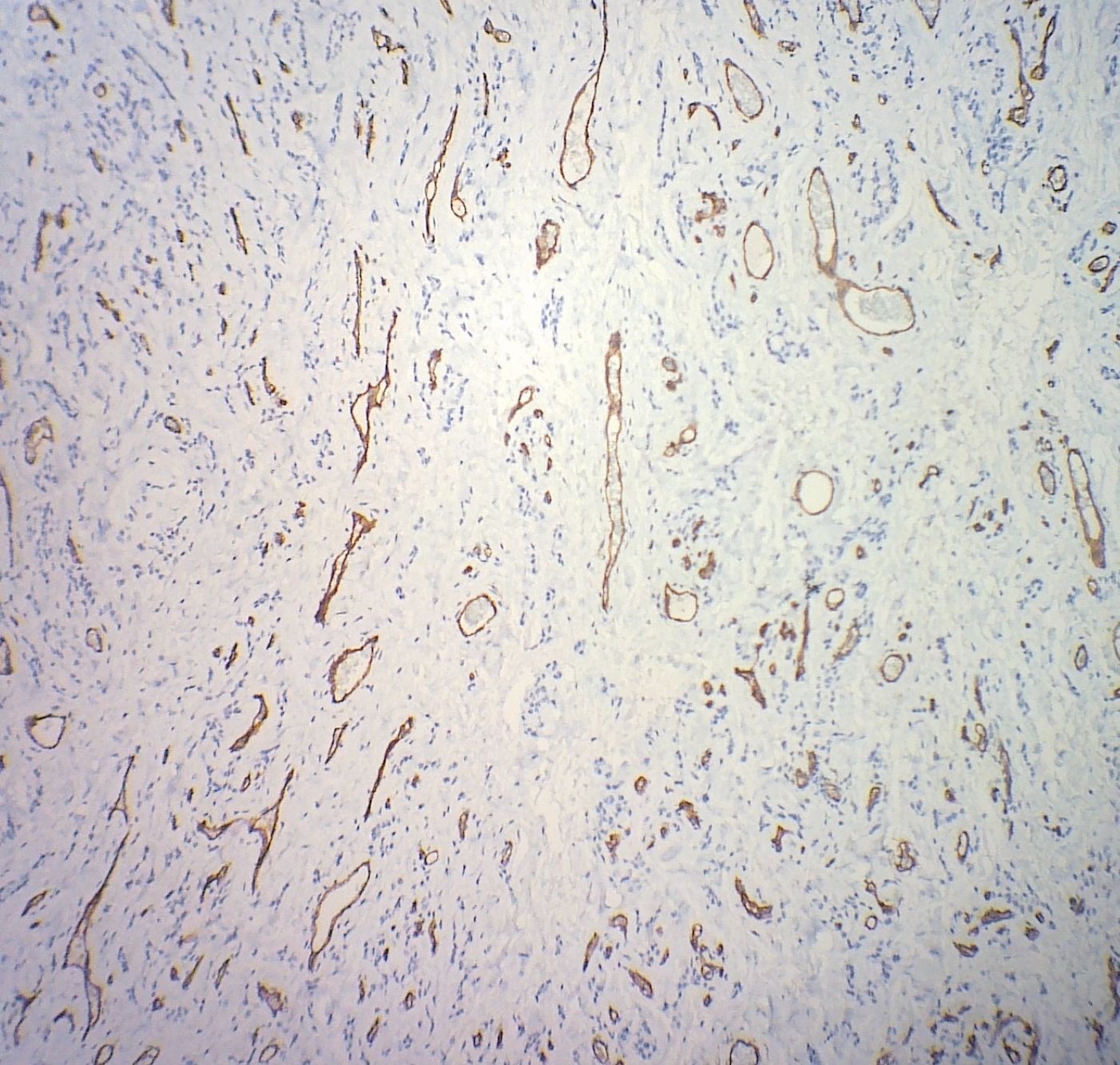
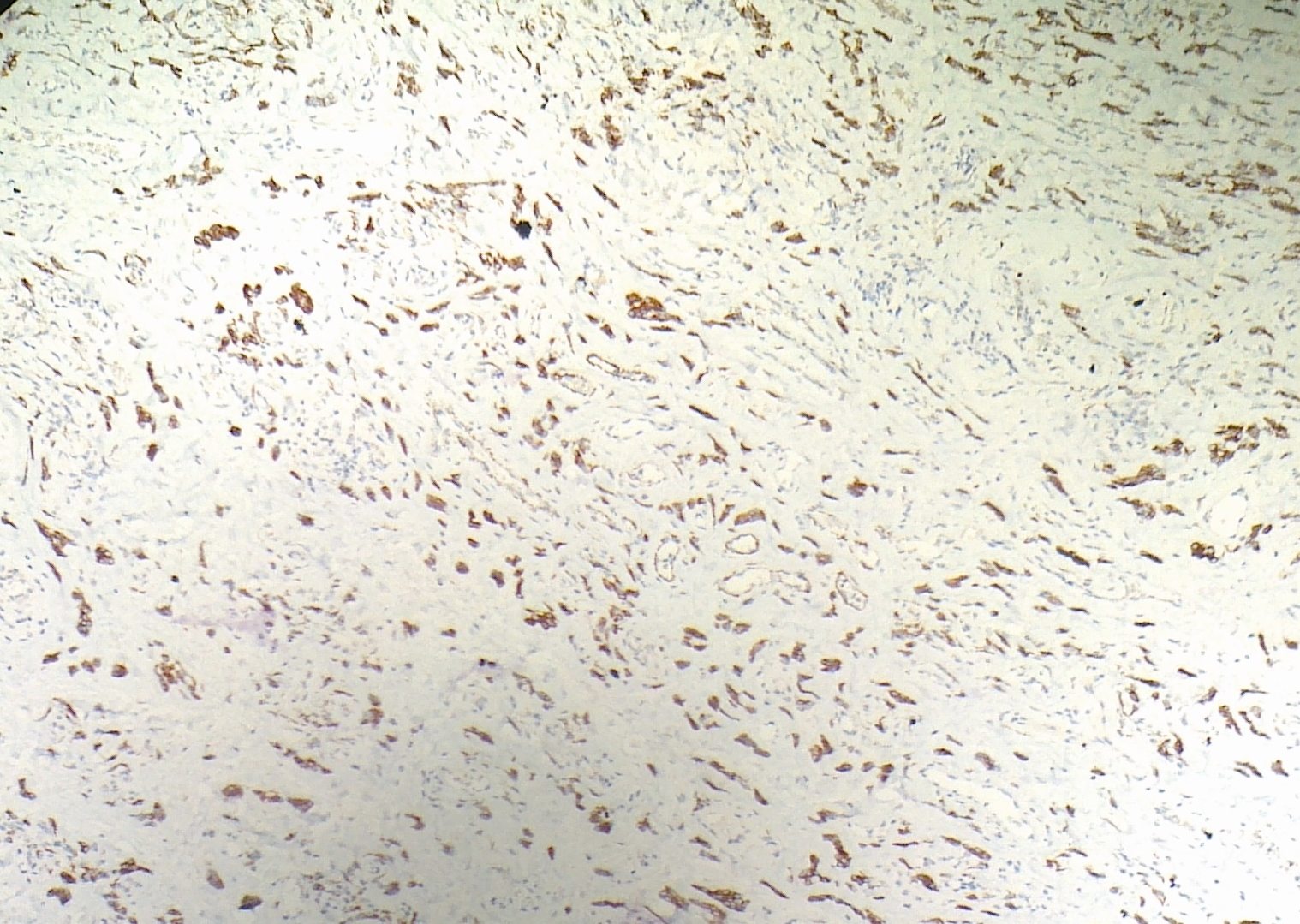
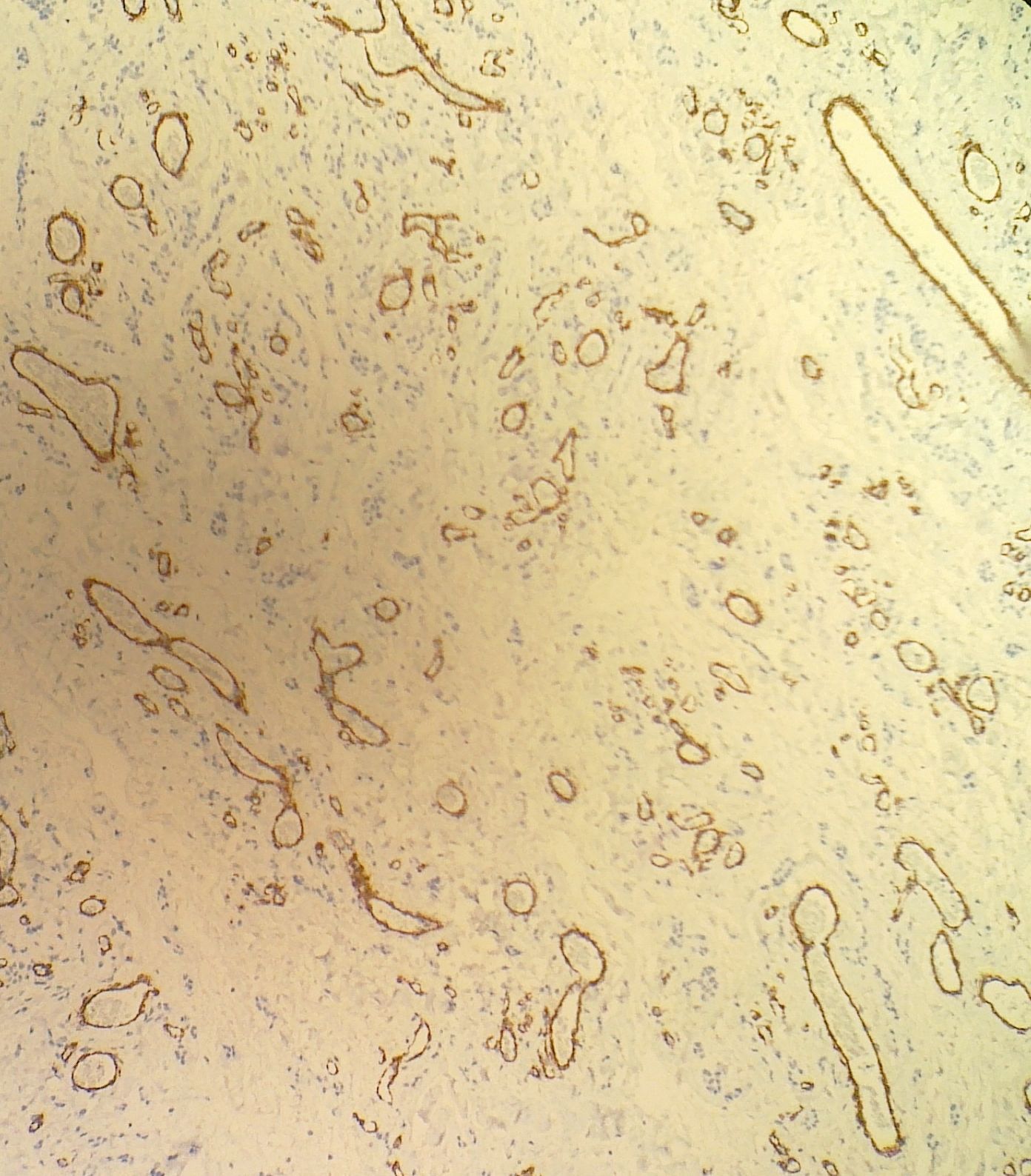
Immunostains

Discussion:
Angiomyofibroblastoma is a rare, benign, mesenchymal vulvar tumor, first described in 1992 (Am J Surg Pathol 1992;16:373). It occurs almost exclusively in the vulvovaginal region of women or the inguinoscrotal region of men.
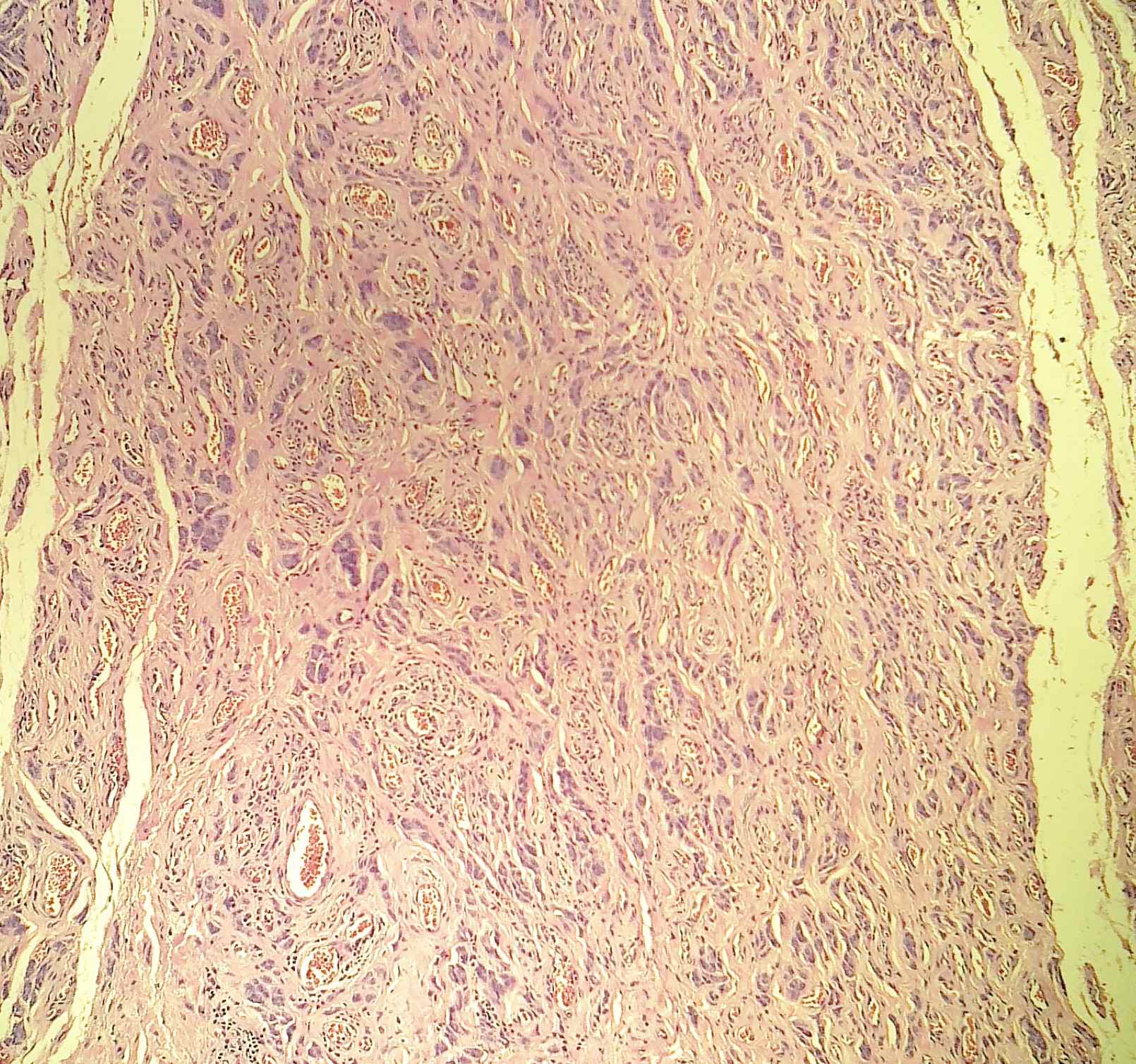
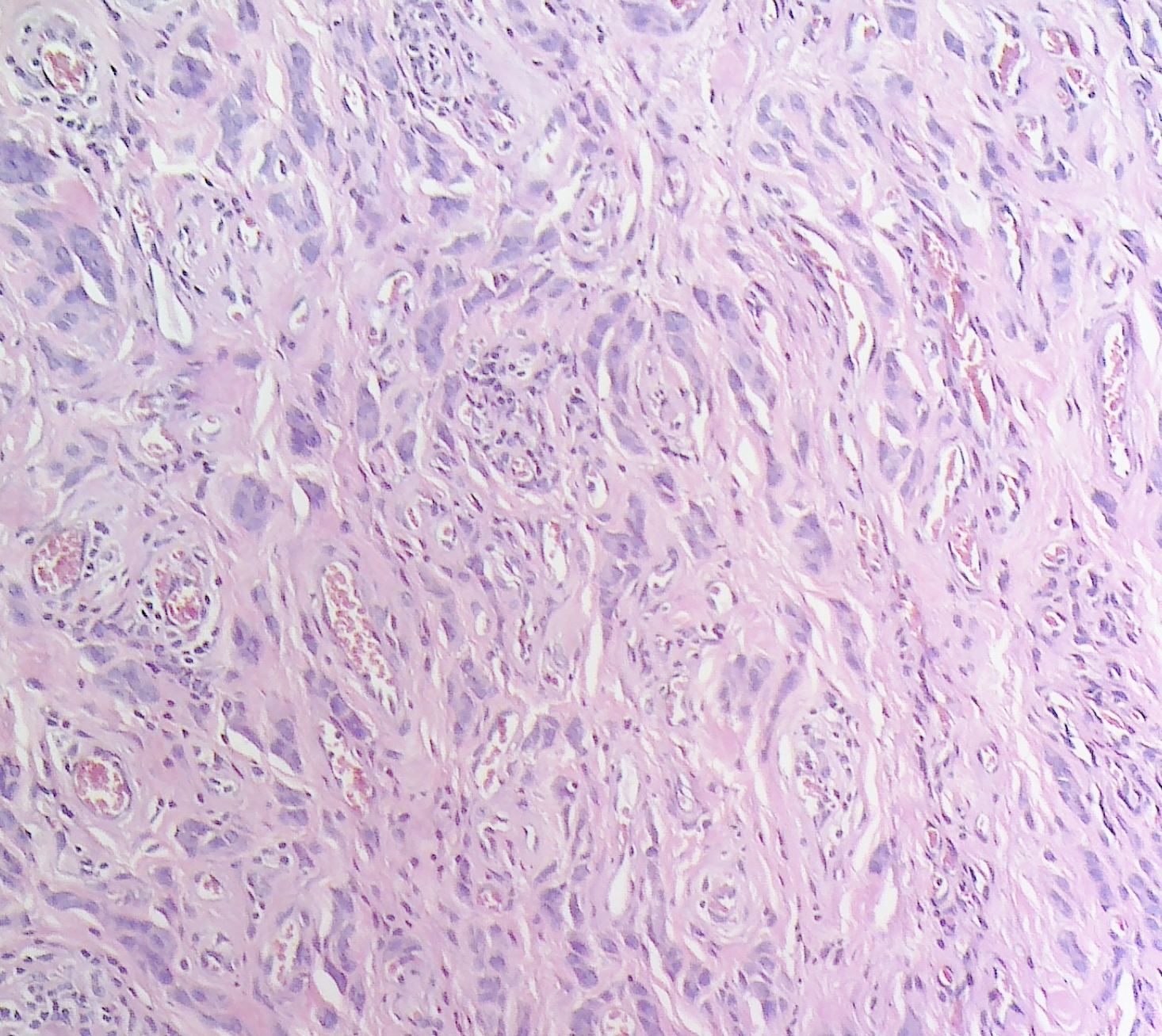
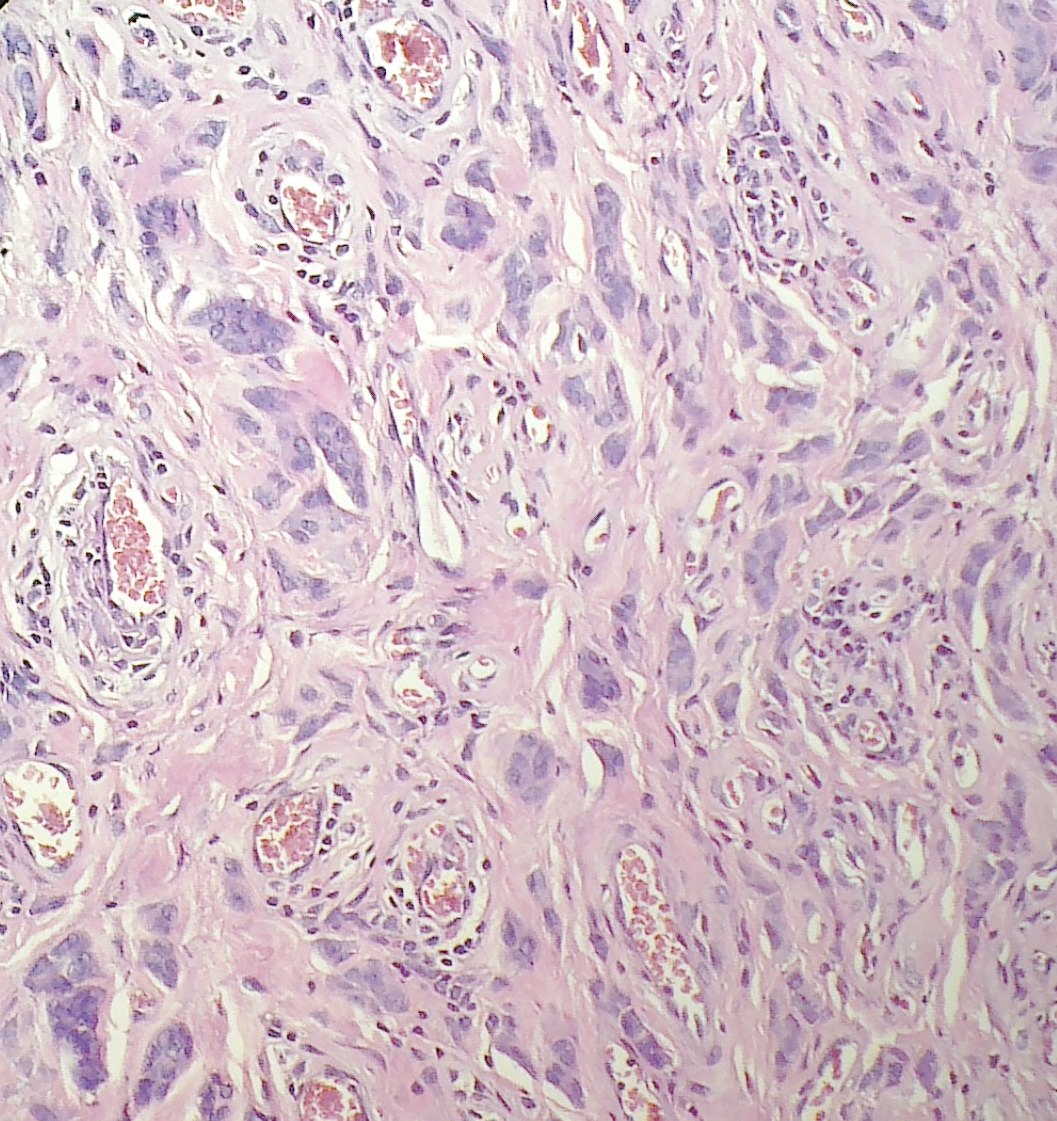
Grossly, it is well circumscribed, usually < 5 cm. Histologically, there are alternating hypercellular and hypocellular areas composed of spindle cells and plump stroma cells, often in clusters, with eosinophilic cytoplasm that aggregate around small, capillary-like blood vessels. Mast cells are common. There may be binucleated or multinucleated cells. There is minimal stromal mucin, rare / no red blood cell extravasation, no atypia and rare / no mitotic figures.
Angiomyofibroblastoma is immunoreactive for vimentin, desmin, ER and PR, and usually negative for keratin, S100 and actin (Mod Pathol 1996;9:284).
The differential diagnosis includes aggressive angiomyxoma. However, angiomyofibroblastoma has circumscribed borders, higher cellularity, more blood vessels (which lack prominent hyalinization), frequent plump stromal cells, minimal stromal mucin and only rare erythrocyte extravasation.
Cellular angiofibroma, also in the differential diagnosis, is uniformly moderately cellular with hyalinized vessels and bland spindle cells but usually no plump epithelioid cells.
Angiomyofibroblastoma has benign behavior and does not recur after excision.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Saroona Haroon, The Aga Khan University Hospital (Pakistan), for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.

Dont miss an issue of the basic pathology research journal
covering all biomedical disciplines in the broad spectrum of pathology.
www.LaboratoryInvestigation.org
Website news:
(1) Our Feature Page for the month highlights Computer software and systems, and includes Milestone Medical and Voicebrook.
(2) We are constantly looking for new Reviewers for our 7,000 topics, which we want to update every 1-2 years. Visit our newly updated Author Instructions page for more information.
(3) The Table of Contents of our Stains chapter now includes all 360 stains / biomarkers described in the chapter. The CD Markers chapter contains an additional 260 markers. We update these pages regularly but let us know of any new markers we should include or other changes we should make.
Visit and follow our Blog to see recent updates to the website.
(1) Our Feature Page for the month highlights Computer software and systems, and includes Milestone Medical and Voicebrook.
(2) We are constantly looking for new Reviewers for our 7,000 topics, which we want to update every 1-2 years. Visit our newly updated Author Instructions page for more information.
(3) The Table of Contents of our Stains chapter now includes all 360 stains / biomarkers described in the chapter. The CD Markers chapter contains an additional 260 markers. We update these pages regularly but let us know of any new markers we should include or other changes we should make.
Visit and follow our Blog to see recent updates to the website.
Case #241
Clinical history:
A 30 year old Asian woman presented with painless vulval swelling for the past 7 months. Clinically, it was diagnosed as a Bartholin cyst. At excision, the swelling was 2 cm, circumscribed and firm.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Angiomyofibroblastoma
Immunostains
Left to right: CD34, desmin, smooth muscle actin, vimentin
Discussion:
Angiomyofibroblastoma is a rare, benign, mesenchymal vulvar tumor, first described in 1992 (Am J Surg Pathol 1992;16:373). It occurs almost exclusively in the vulvovaginal region of women or the inguinoscrotal region of men.
Grossly, it is well circumscribed, usually < 5 cm. Histologically, there are alternating hypercellular and hypocellular areas composed of spindle cells and plump stroma cells, often in clusters, with eosinophilic cytoplasm that aggregate around small, capillary-like blood vessels. Mast cells are common. There may be binucleated or multinucleated cells. There is minimal stromal mucin, rare / no red blood cell extravasation, no atypia and rare / no mitotic figures.
Angiomyofibroblastoma is immunoreactive for vimentin, desmin, ER and PR, and usually negative for keratin, S100 and actin (Mod Pathol 1996;9:284).
The differential diagnosis includes aggressive angiomyxoma. However, angiomyofibroblastoma has circumscribed borders, higher cellularity, more blood vessels (which lack prominent hyalinization), frequent plump stromal cells, minimal stromal mucin and only rare erythrocyte extravasation.
Cellular angiofibroma, also in the differential diagnosis, is uniformly moderately cellular with hyalinized vessels and bland spindle cells but usually no plump epithelioid cells.
Angiomyofibroblastoma has benign behavior and does not recur after excision.
