
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Chungja C. Shim, Titusville Area Hospital, Pennsylvania (USA) for contributing this case.


July 9-13, 2012
The Snow King Resort
Jackson, Wyoming (USA)
The 29th Annual Summer Update
in Clinical Immunology, Microbiology
and Infectious Disease
Course Topics:
This 23.75-hour review and update in the areas of clinical immunology, microbiology, and infectious diseases is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory, including selection and interpretation of results.
This course will provide a forum for the exchange of ideas dealing with microbial infections as well as immunity to infectious diseases and immunologic disorders. Faculty consists of clinicians involved in patient care, pathologists, and clinical laboratory scientists. Discussion of timely topics by faculty and participants assures that this course will be informative, interesting, and relevant.
Course Directors:
Harry R. Hill MD, Larry G. Reimer MD, July Daly PhD and John M. Matsen MD
Special Guests:
Paul G. Quie MD, Frederick A. Meier MD and John M. Matsen MD
Course CME:
This course is approved for 23.75 AMA PRA Category I Credit(s)
Website
Schedule
Hotel
Register
(1) The Uterus chapter has now been updated, based on reviews by Mohamed Mokhtar Desouki, M.D., Ph.D. and Nat Pernick, M.D.
Visit and follow our Blog to see recent updates to the website.
Case #237
Clinical history:
A 45 year old woman presented with a large pelvic mass thought to be uterine. She was scheduled for a total hysterectomy with bilateral salpingo-oophorectomy. At surgery, the pelvic mass was attached to the mid jejunum and adherent to the pelvic peritoneum behind the uterus. The entire mass was resected.
The pelvic mass was 253 gm and measured 12 x 10 x 5.5 cm. It was solid with necrosis and hemorrhage on the cut surface.
Gross image:

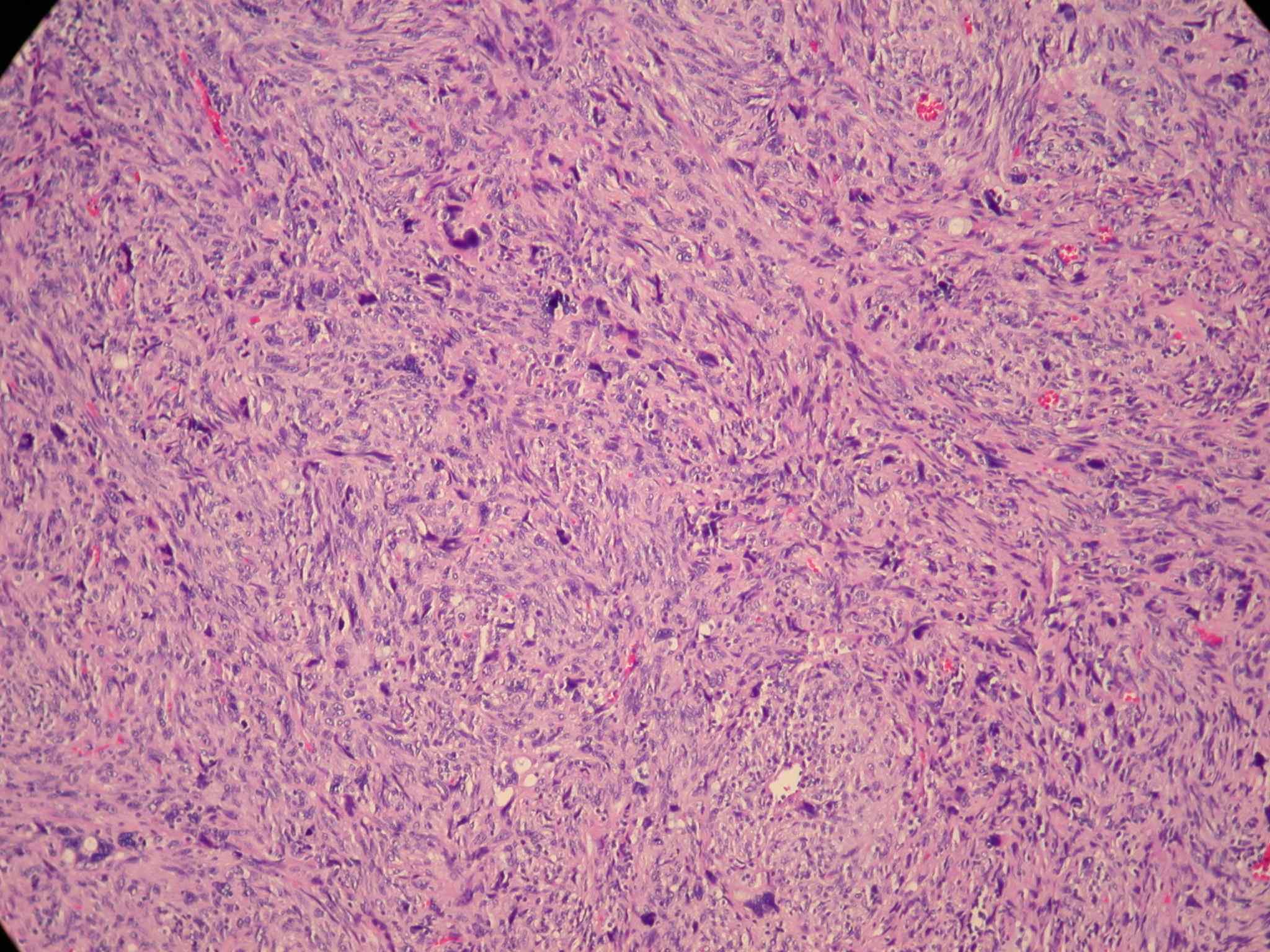
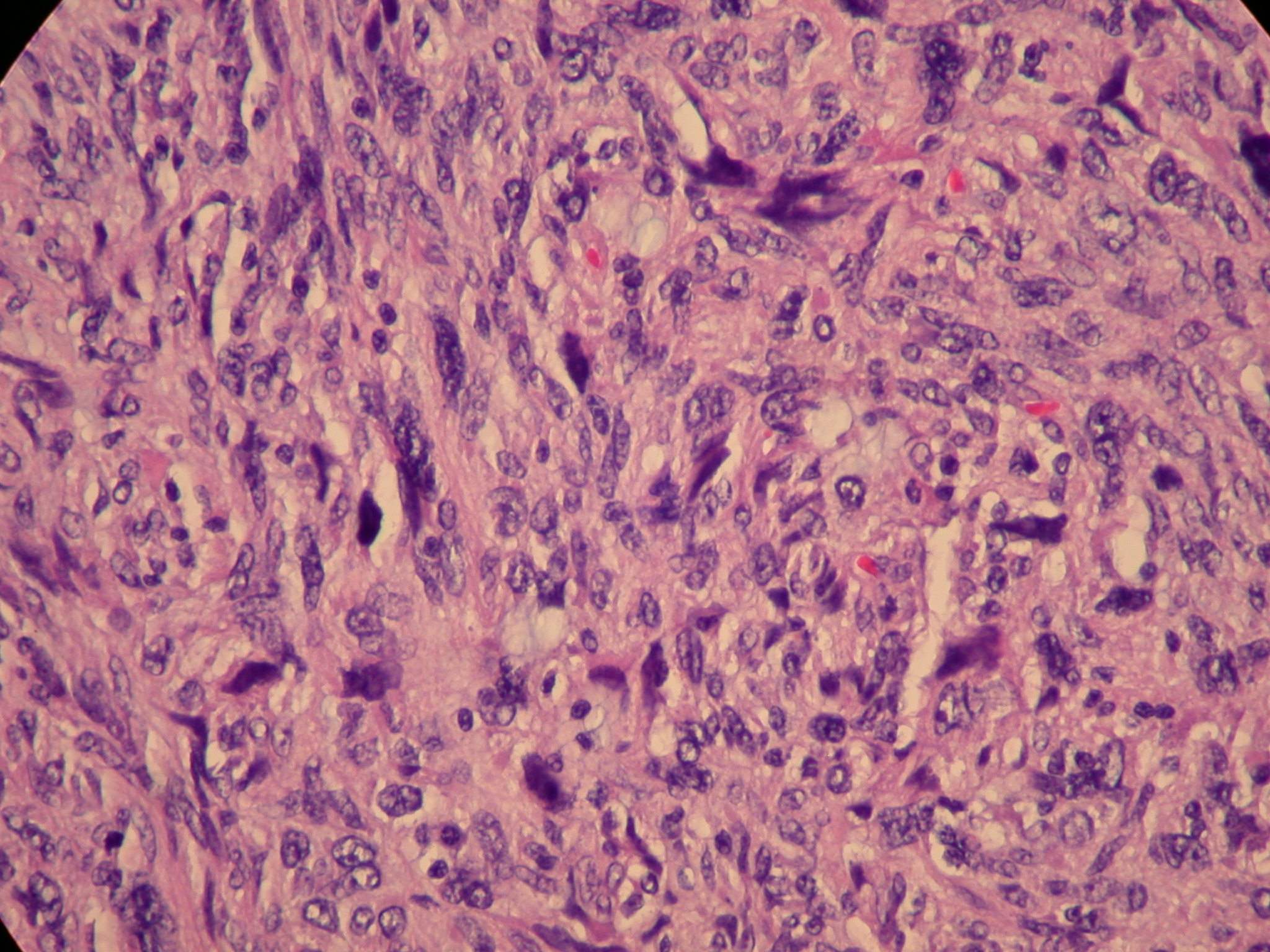
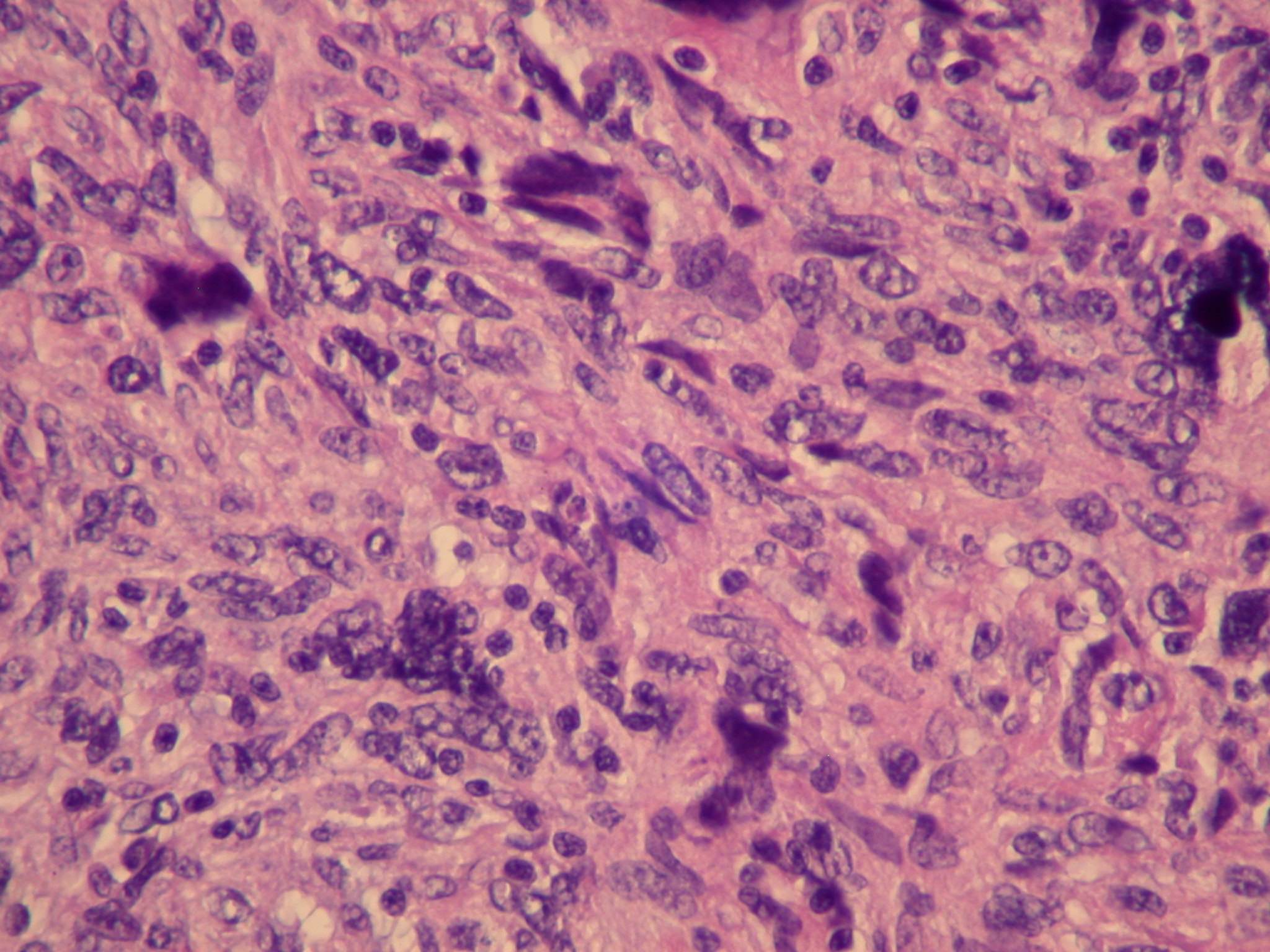
Microscopic images:


What is your diagnosis?
Diagnosis: High grade GIST
Immunostains:
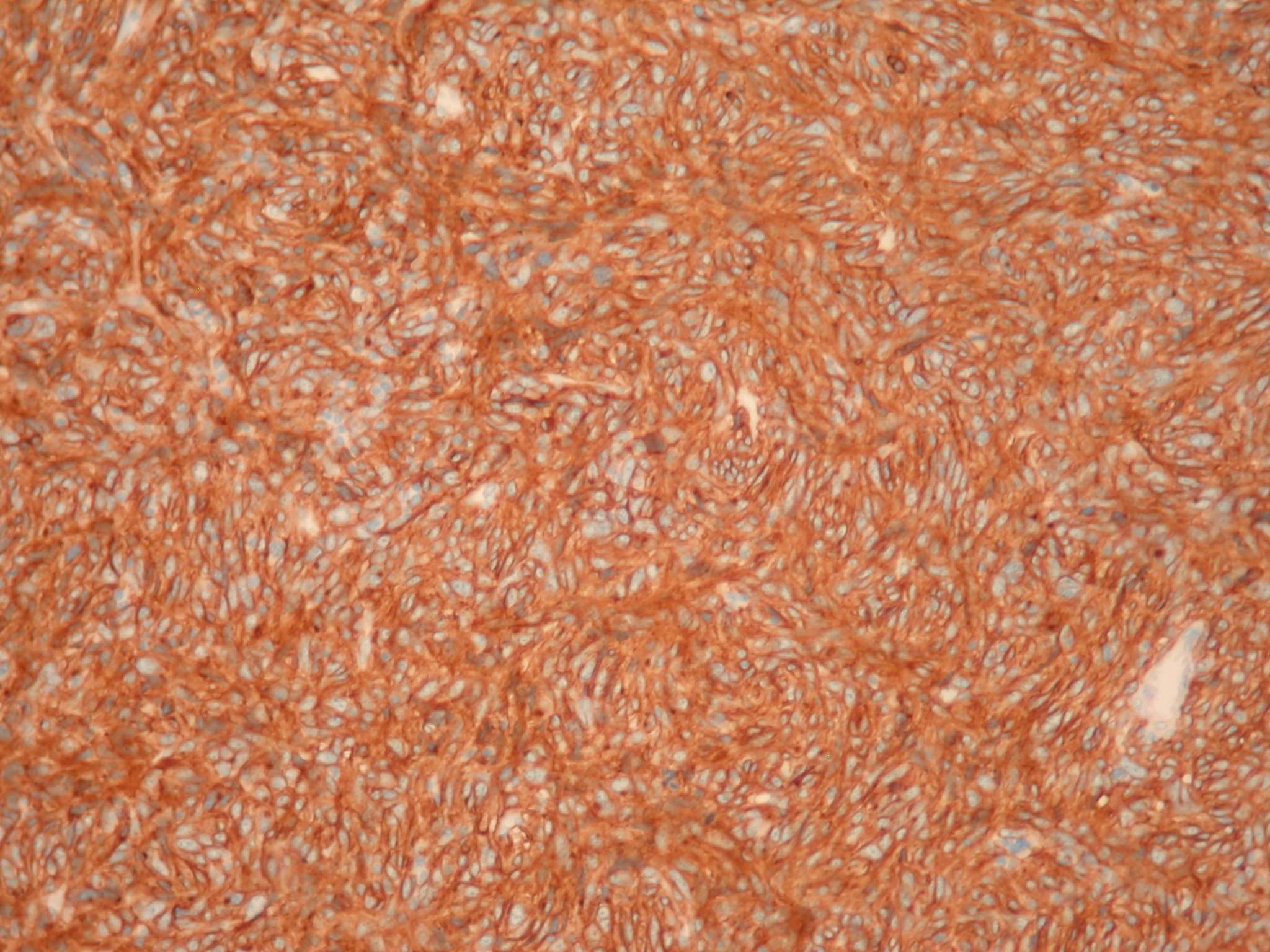

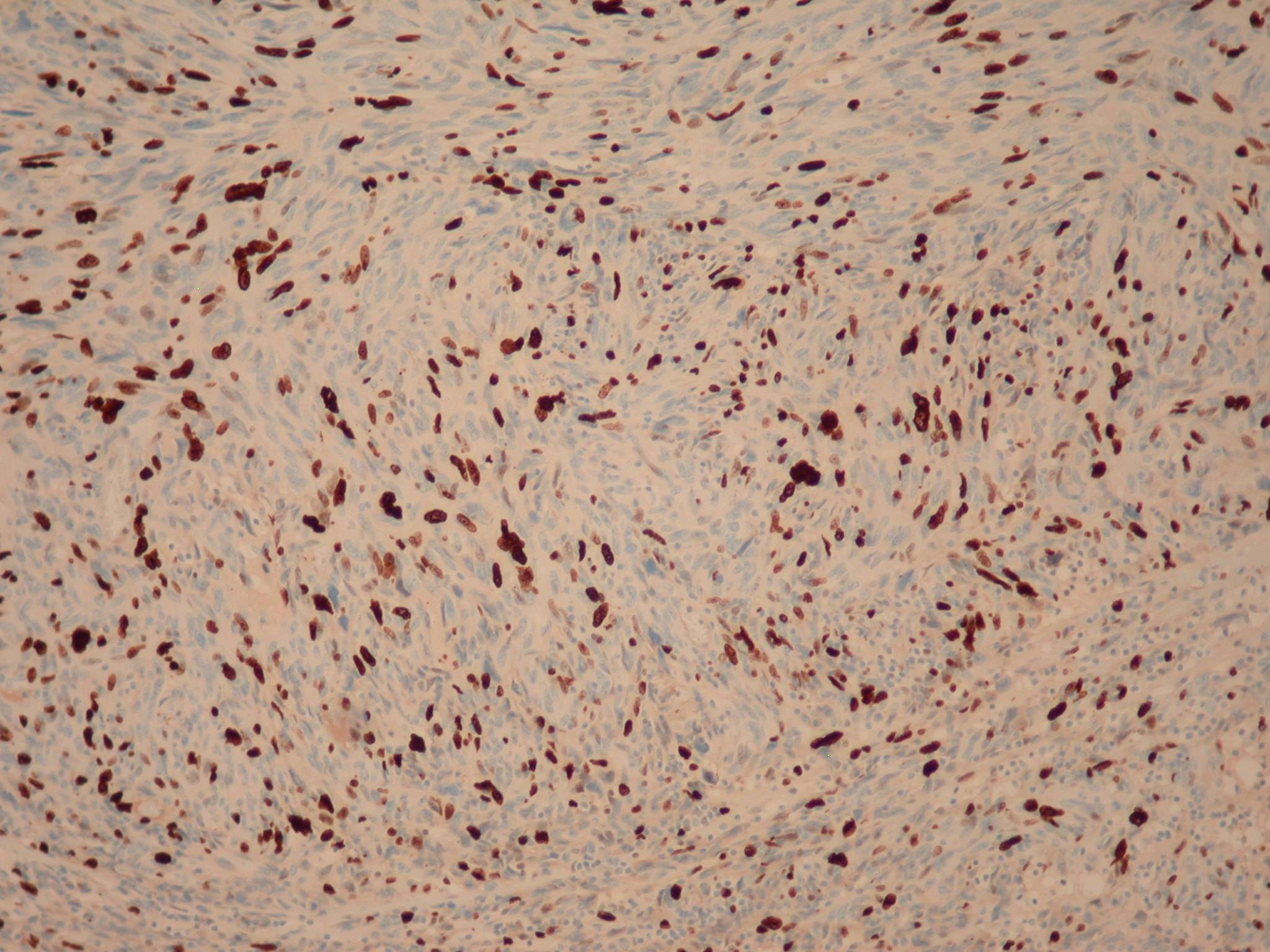
Left to right: CD117+ (strong membranous staining of most spindle cells), CD34+ (staining of many spindle cells with strong vascular staining), Ki67+ (strong nuclear staining)
Discussion:
Immunostains showed a CD117+, CD34+ tumor with a high proliferative (Ki67) index.
The tumor cells were negative for cytokeratin AE1 / AE3, S100, SMA, desmin and CD68.
This tumor was a 12 cm mass adherent to the small bowel, with hemorrhage and necrosis. Morphologically, it was a high grade and pleomorphic spindle cell tumor.
The differential diagnosis includes leiomyosarcoma, symplastic leiomyoma and fibromatosis. Leiomyosarcomas have smooth muscle morphology, although this may not be obvious in high grade cases. Symplastic leiomyoma contains bizarre multinucleated tumor cells that may look malignant but there are usually areas resembling typical leiomyoma and there is no hemorrhage or necrosis.
Both leiomyosarcomas and leiomyomas show some smooth muscle features by immunohistochemistry (SMA or desmin positive), are negative for CD117 and CD34, and lack c-kit mutations. Intraabdominal fibromatosis has some overlapping features but the morphology is different, with uniform cellularity composed of bipolar fibroblasts and myofibroblasts, and a background of distinct collagen with a mucopolysaccharide matrix containing thin walled, curvilinear or ectatic vessels. Fibromatosis has variable staining for smooth muscle actin and muscle specific actin and may stain for CD117. However, the cells are negative for CD34 and have no c-kit mutations (Adv Anat Pathol 2007;14:178).
Treatment of malignant GIST is typically surgical excision and tyrosine kinase inhibitors (J Natl Compr Canc Netw 2010;8 Suppl 2:S1). Prognosis is based on size and mitotic activity (Am J Surg Pathol 2006;30:477, J Natl Compr Canc Netw 2010;8 Suppl 2:S1).
