
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Saroona Haroon, The Aga Khan University Hospital (Pakistan), for contributing this case.

You Need Us Now More Than Ever. Many pathologists and laboratories are suffering from a simple lack of revenue management. Your payments will get worse if you choose to do nothing. You need to start auditing your billing and collection process and negotiate for more revenue.
Vachette Pathology is a pathology and laboratory practice management and hospital consulting firm. We currently manage over 50 pathology and laboratory practices coast-to-coast. They range from single man pathology practices to independent laboratories to 35 hospital based practices. Our Practice Managers have extensive experience in the field of hospital and laboratory billing. We can help to increase your revenue and secure your income.
Pick up the phone and call me and lets start increasing your income today, contact Mick Raich toll free at 866-407-0763 or at
mraich@vachettepathology.com. Visit us online by clicking here.
(1) We have added links for free CME from Cleveland Clinic to our CME page, which has a link on the left side of the Home page.
(2) The second half of the Lymphoma and plasma cell neoplasms chapter (T/NK cell disorders, Hodgkin's lymphoma, post-transplant, other) was recently updated based on a review by Dragos C. Luca, M.D., Children's Hospitals & Clinics of Minnesota. The balance of this chapter was updated in early 2011.
Visit and follow our Blog to see recent updates to the website.
Case #235
Clinical history:
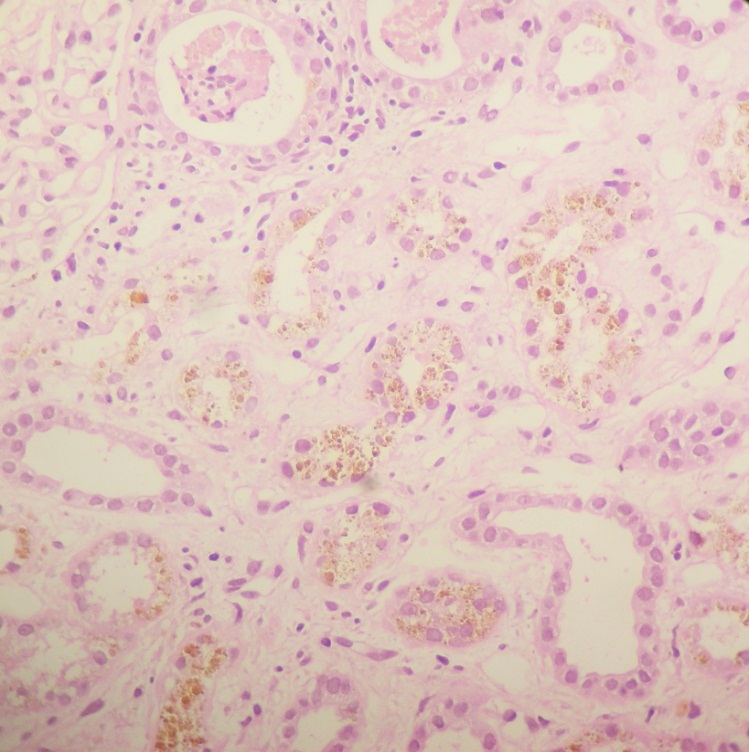
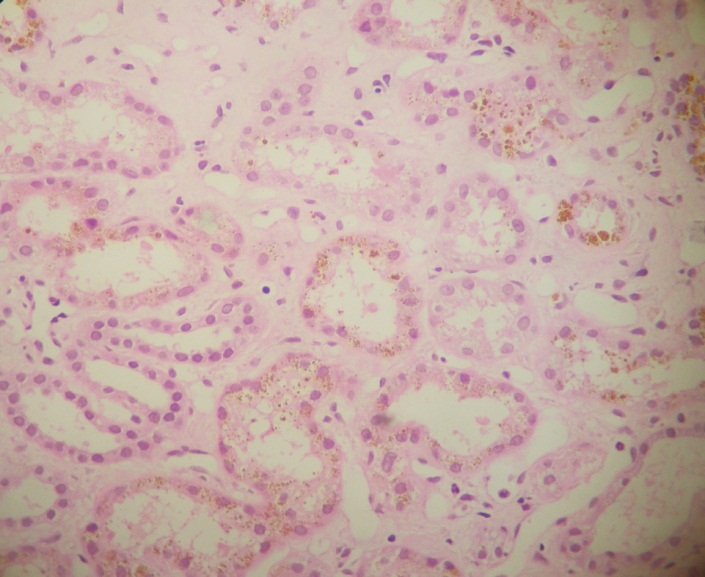
A 52 year old Asian man, hypertensive for 7 years, presented with slowly increasing serum creatinine levels, currently 3.1 mg/dl, and current renal failure. Urine showed microscopic hematuria. His past medical history included a heart valve replacement due to valvular heart disease at age 30 years. As the etiology of the increasing creatinine was unknown, a renal biopsy was obtained.
Microscopic images:
What is your diagnosis?
Diagnosis: Renal hemosiderosis, secondary to hemolytic anemia (heart valve complication)
Immunostains:
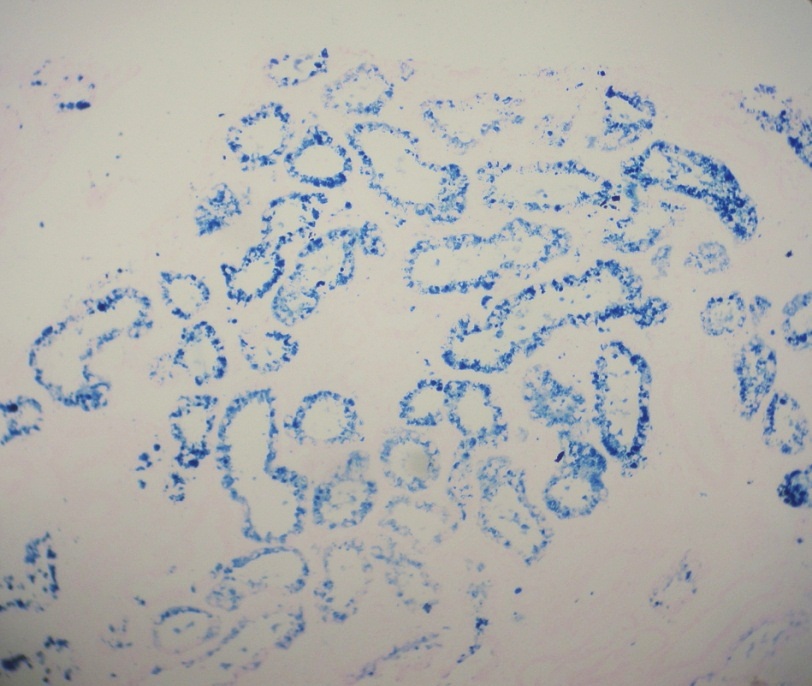
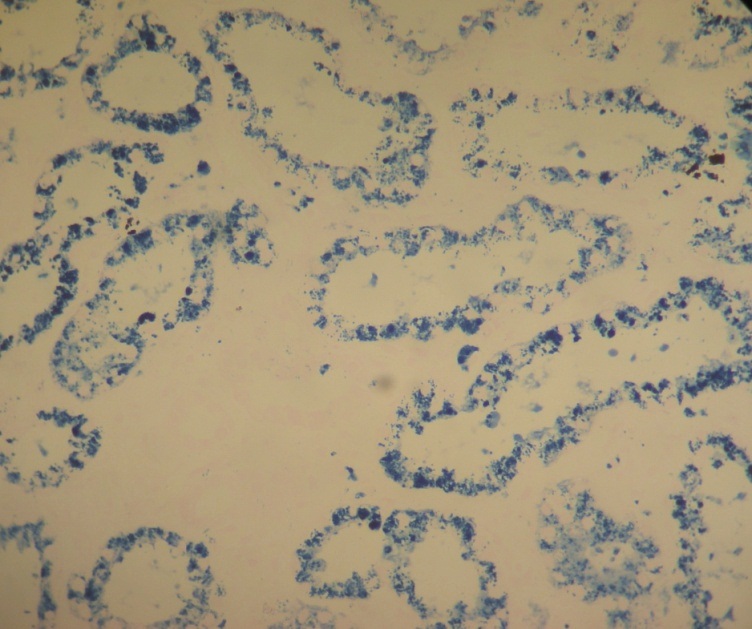
Iron stain
Discussion:
Renal hemosiderosis due to hemolytic anemia is a rare cause of renal failure (Am J Pathol 1966;48:409, Indian J Pathol Microbiol 2011;54:379). Hemosiderosis is defined as the histologic equivalent of secondary iron overload, usually due to hemosiderin, which may be focal. Hemosiderin is a golden yellow to brown granular cellular pigment due to hemoglobin breakdown. Typically, free serum hemoglobin is bound to haptoglobin, but in severe cases, the free hemoglobin is filtered by the kidney and deposited in the proximal convoluted tubules, which may cause renal failure.
Renal hemosiderosis is caused by recurrent intravascular hemolysis and may be due to hemolytic anemia, paroxysmal nocturnal hemoglobinuria (PNH) and mechanical hemolysis from prosthetic cardiac valves. In this case, the hemolysis was attribute to chronic mechanical damage due to shearing of red blood cells by the prosthetic valve. Correction of a dysfunctional valve may be therapeutic (Arch Mal Coeur Vaiss 1993;86:111).
