
7 February 2012 - Case #232
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Hillary Kimbrell, Tulane University School of Medicine, for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case #232
Clinical history:
A 51 year old woman with uterine leiomyomas underwent a total abdominal hysterectomy bilateral salpingo-oophorectomy for a 3 cm adnexal mass, which turned out to be a serous cystadenofibroma. The uterus also contained a 3.0 cm white-tan subserosal nodule.
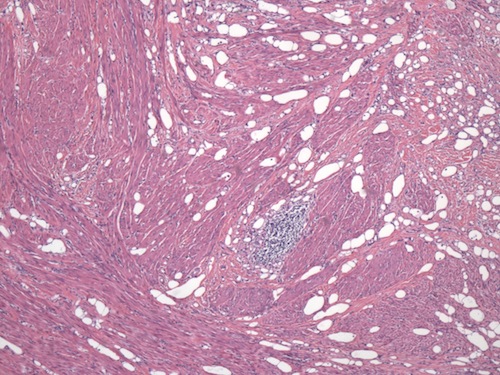
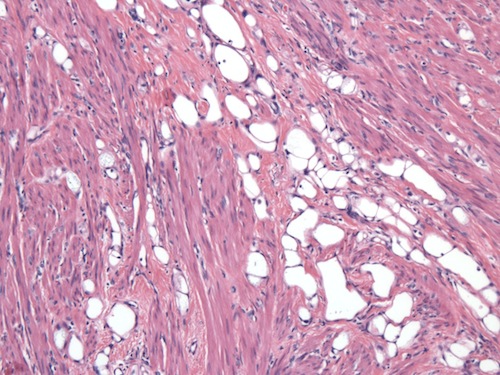
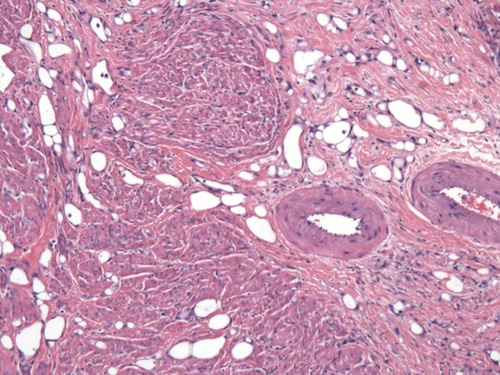
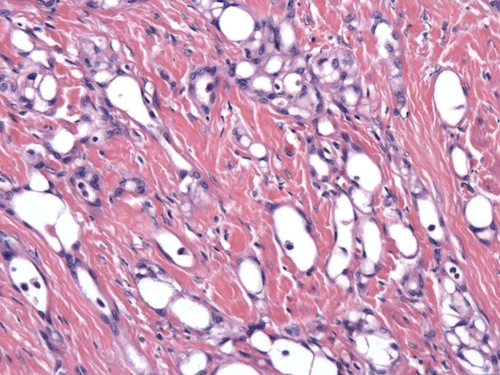
Microscopic images:
What is your diagnosis?
Diagnosis: Adenomatoid tumor of uterus
Discussion:
Adenomatoid tumors are benign mesothelial tumors present in many different organs, particularly in the male and female genital tracts. The mesothelial cells form slit-like, tubular or gland-like (adenomatoid) structures that infiltrate smooth muscle bundles or a fibrous stroma. The tumor cells range from cuboidal to flattened; thus, the gland-like structures can resemble lymphatic channels, signet ring cells or adipocytes; however the tumor cells are positive for mesothelial markers calretinin and HBME-1.
The tumor cell nuclei are cytologically bland and there is little mitotic activity. Ki67 stains < 1% of the tumor cells. Despite the invasive appearing growth pattern, there is no desmoplasia or stromal response. The smooth muscle bundles within the tumor are felt to be hyperplastic rather than neoplastic. Lymphocytic aggregates or follicles are commonly seen.
In the uterus, adenomatoid tumors grossly resemble leiomyomas but adenomatoid tumors are not as well defined and may not bulge out as much from the surrounding myometrium. They may also be softer than a typical leiomyoma. Most adenomatoid tumors are subserosal but may be intramural or even submucosal.
They are usually incidental findings but can have large cystic spaces and may present as a pelvic mass. They are invariably benign.
References: Int J Gynecol Pathol 2002;21:34, Lee: Diagnostic Gynecologic and Obstetric Pathology, 2nd Edition, 2011, IARC: Pathology and Genetics of Tumours of the Breast and Female Genital Organs, 1st Edition, 2003
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Hillary Kimbrell, Tulane University School of Medicine, for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Saturday, May 19, 2012
The Townsend Hotel
Birmingham, Michigan (USA)
Current Concepts in
GYN Oncology and Pathology

Sponsored by Karmanos Cancer Institute, Henry Ford Health System,
Wayne State University School of Medicine and the Detroit Medical Center

Course Director:
Rouba Ali-Fehmi, M.D.
Website
Hotel
Register
For more information, please call (313) 745-8555 or
email rali@med.wayne.edu
[#2913]
Website news:
(1) Our Feature Page for the month highlights Microscopes / slide imaging, and includes Celestron, Leica Microsystems and Optronics.
(2) In January 2012, we again had record traffic, with 366,984 visits (8.8 million "hits").
(3) We posted a new article on our Management Page, Thoughts for the New Year (2012), by Mick Raich, Vachette Pathology.
(4) We have added links for free CME from ARUP and Johns Hopkins to our new CME page, which has a link on the left side of the Home page.
Visit and follow our Blog to see recent updates to the website.
(1) Our Feature Page for the month highlights Microscopes / slide imaging, and includes Celestron, Leica Microsystems and Optronics.
(2) In January 2012, we again had record traffic, with 366,984 visits (8.8 million "hits").
(3) We posted a new article on our Management Page, Thoughts for the New Year (2012), by Mick Raich, Vachette Pathology.
(4) We have added links for free CME from ARUP and Johns Hopkins to our new CME page, which has a link on the left side of the Home page.
Visit and follow our Blog to see recent updates to the website.
Case #232
Clinical history:
A 51 year old woman with uterine leiomyomas underwent a total abdominal hysterectomy bilateral salpingo-oophorectomy for a 3 cm adnexal mass, which turned out to be a serous cystadenofibroma. The uterus also contained a 3.0 cm white-tan subserosal nodule.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Adenomatoid tumor of uterus
Discussion:
Adenomatoid tumors are benign mesothelial tumors present in many different organs, particularly in the male and female genital tracts. The mesothelial cells form slit-like, tubular or gland-like (adenomatoid) structures that infiltrate smooth muscle bundles or a fibrous stroma. The tumor cells range from cuboidal to flattened; thus, the gland-like structures can resemble lymphatic channels, signet ring cells or adipocytes; however the tumor cells are positive for mesothelial markers calretinin and HBME-1.
The tumor cell nuclei are cytologically bland and there is little mitotic activity. Ki67 stains < 1% of the tumor cells. Despite the invasive appearing growth pattern, there is no desmoplasia or stromal response. The smooth muscle bundles within the tumor are felt to be hyperplastic rather than neoplastic. Lymphocytic aggregates or follicles are commonly seen.
In the uterus, adenomatoid tumors grossly resemble leiomyomas but adenomatoid tumors are not as well defined and may not bulge out as much from the surrounding myometrium. They may also be softer than a typical leiomyoma. Most adenomatoid tumors are subserosal but may be intramural or even submucosal.
They are usually incidental findings but can have large cystic spaces and may present as a pelvic mass. They are invariably benign.
References: Int J Gynecol Pathol 2002;21:34, Lee: Diagnostic Gynecologic and Obstetric Pathology, 2nd Edition, 2011, IARC: Pathology and Genetics of Tumours of the Breast and Female Genital Organs, 1st Edition, 2003
