
Home
Case
of Week Home
Jobs
Conferences
Fellowships
Books
30 November 2011 - Case of the Week #225
All cases are archived on our website. To view them sorted by number, diagnosis or category, visit our Home Page and click on the Case of the Week button on the left hand side. To subscribe or unsubscribe to the Case of the Week or our other email lists, click here.
Thanks to Jerad M. Gardner, M.D. and Ruan T. Ramjit, M.D., Emory University, Georgia (USA), for contributing this case. To contribute a Case of the Week, follow the guidelines on our Case of the Week page.
CancerTYPE ID is a standardized, objective molecular test based on the differential expression of 92 genes, that classifies tumors by matching the gene expression pattern of a patients tumor tissue to a database of known tumor types and histological subtypes.
CancerTYPE IDs database includes 2,206 tumors from multiple tumor banks, selected to provide broader and deeper representation of the heterogeneity of tumors. The 92-gene assay does not overlap with IHC markers, providing complementary data to standard tumor diagnosis.
CancerTYPE ID uses real-time reverse transcription polymerase chain reaction (RT-PCR). A very low copy number of RNA molecules can be detected, thus reducing the sample tissue required for testing. Testing is conducted and results are generated at bioTheranostics' CAP-accredited, CLIA-certified laboratory.
For more information, click here.
Advertisement
Website news:
(1) Don't forget to do your Holiday shopping by clicking on the Amazon.com links on our Home Page, by clicking here or by clicking on any link on our Books pages.
(2) The Stains and CD Markers chapters have been changed so each now appears on one page, instead of being divided into separate pages. We are also updating these topics more frequently.
(3) Our Mystery case is back! Each month, we will post an interesting image on the right side of the Home page. Click on the picture to enlarge it. Click on the link below the image for the answer, and a link to the topic for more information.
Case of the Week #225
Clinical History:
A 73 year old man had a 4 month history of progressive right leg swelling with tender nodules, which began with a splinter injury while chopping firewood. Past medical history is remarkable for treated non-Hodgkins lymphoma, diagnosed 2 years previously. The nodules were biopsied.
Micro images:
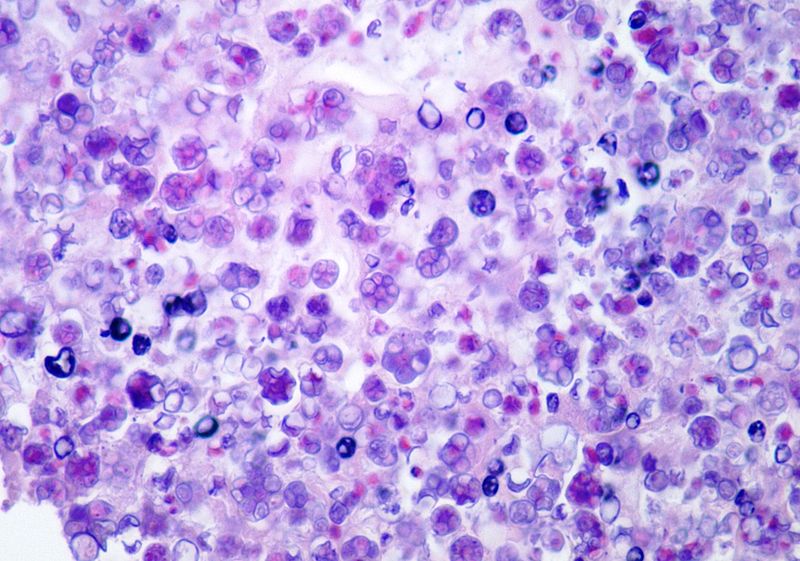
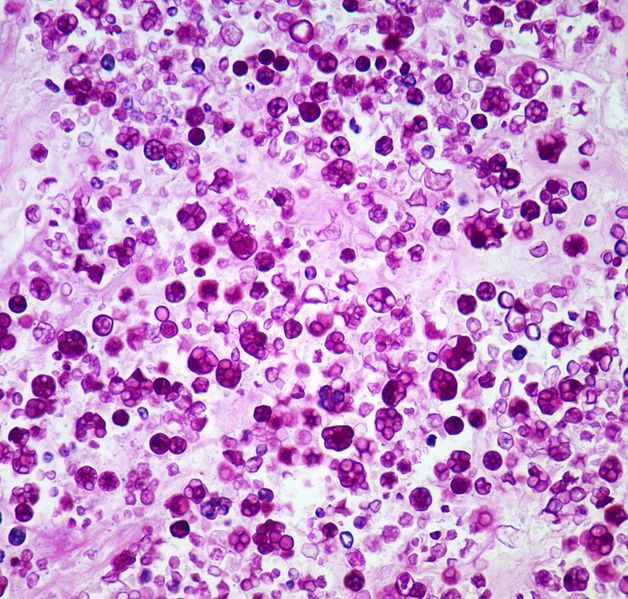
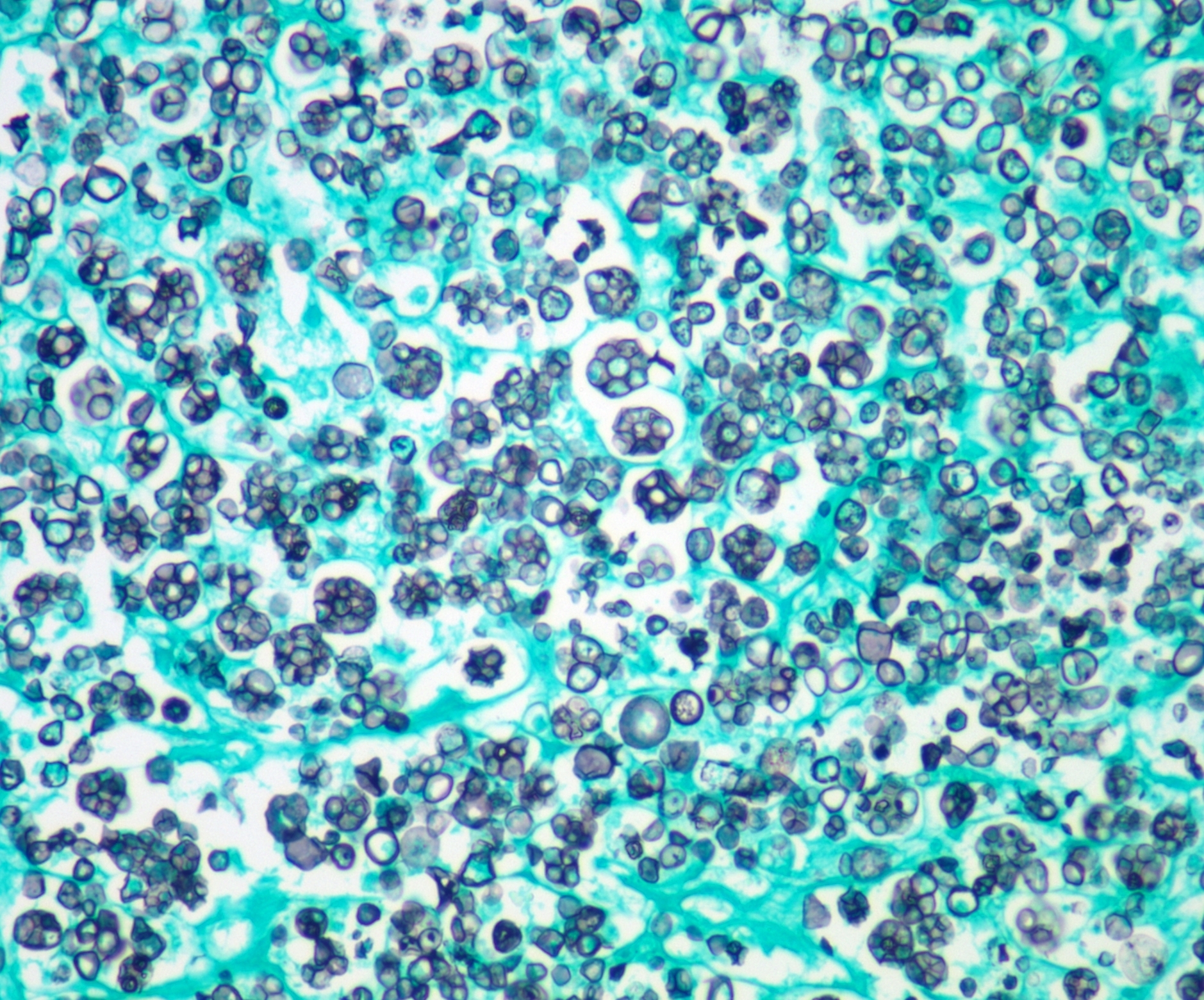
Left to right: H&E, PAS, GMS
What is your diagnosis?
Diagnosis:
Prototheca wickerhamii
Discussion:
The organism was cultured on blood, chocolate, and
Sabourauds dextrose agar. After two days, the organism appeared as yeast-like colonies on all media.
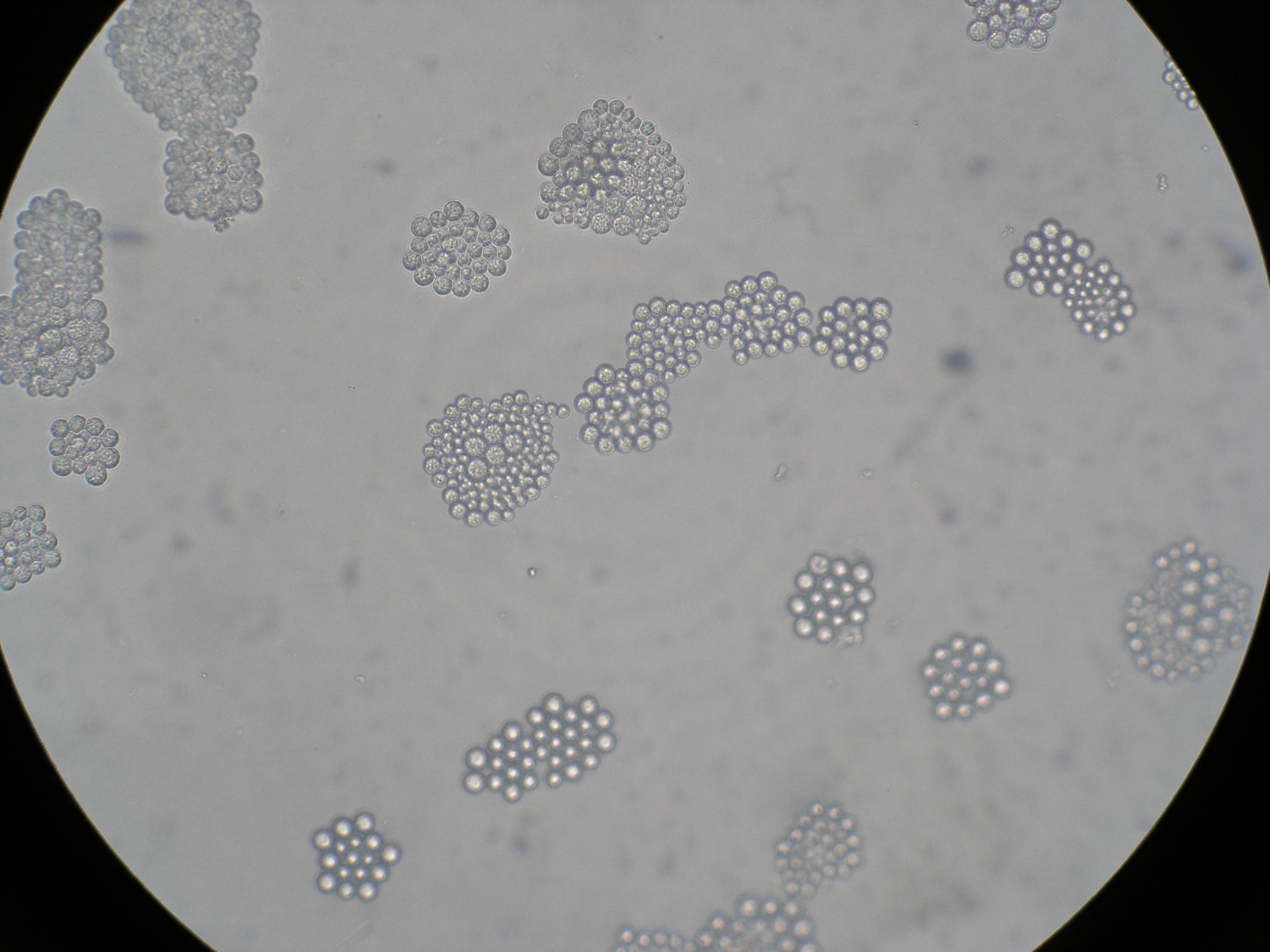
Microscopic examination of the culture plates showed multiple spherical organisms in clusters with thick walls. The organism cultured on the agar plates was inoculated onto an API 20 C AUX strip (bioMerieux Inc., Durham, NC, USA), used to identify the most frequently encountered yeasts. Based on the results of the carbohydrate assimilation tests on this panel, the organism was identified as Prototheca wickerhamii.
Prototheca was first recognized as a human pathogen in 1964 (J Clin Microbiol 2004;42:4907). Two species are associated with human disease - P. wickerhamii and P. zopfii. These fungi-like organisms are actually aerobic, achlorophyllous, algae-like, unicellular organisms commonly present in water, sewage and soil. Human infection is rare, and usually occurs via trauma or contaminated water, and involves the face or exposed extremities. Patients are often immunocompromised (Arch Pathol Lab Med 2011;135:941, Am J Surg Pathol 1994;18:1261). Patients present with erythematous plaques, nodules or superficial ulcers.
Histologically, there are necrotizing granulomas containing spherical organisms with central basophilia, internal septation and double layered cell walls. There may also be multiple endospores 2-4 microns in size. Green algae may appear similar, but contain abundant cytoplasmic starch granules (Arch Pathol Lab Med 1978;102:353).
Recommended treatment is surgery or Amphotericin B for disseminated disease. In this case, the patient had rapid progression of his disease in a lymphangiitic pattern. He was admitted to the hospital with a plan to either debride or amputate the leg, but died before surgery began. No autopsy was performed.
Additional references: Skin-nontumor chapter of PathologyOutlines.com
Nat Pernick, M.D., President
and Liz Parker, B.A., Associated Medical Editor
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email:
NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com