
Home
Case
of Week Home
Jobs
Conferences
Fellowships
Books
28 September 2011 Case of the Week #218
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email
lists, click
here.
All cases are archived on our website. To view them sorted by number, diagnosis or category,
visit our Home Page and click on the Case of the Week button on the left hand side.
Thanks to Dr. Oluyomi Asojo, University of Cincinnati, Ohio, for contributing this case. To contribute a Case of the Week, follow the guidelines on our Case of the Week page.
CancerTYPE ID is a standardized, objective molecular test based on the differential expression of 92 genes, that classifies tumors by matching the gene expression pattern of a patients tumor tissue to a database of known tumor types and histological subtypes.
CancerTYPE IDs database includes 2,206 tumors from multiple tumor banks, selected to provide broader and deeper representation of the heterogeneity of tumors. The 92-gene assay does not overlap with IHC markers, providing complementary data to standard tumor diagnosis.
CancerTYPE ID uses real-time reverse transcription polymerase chain reaction (RT-PCR). A very low copy number of RNA molecules can be detected, thus reducing the sample tissue required for testing. Testing is conducted and results are generated at bioTheranostics' CAP-accredited, CLIA-certified laboratory.
For more information, click here.
Advertisement
Website news:
(1) To encourage a wider display of pathology related books on our Books pages, we are pleased to announce a new low price of $100 to post any pathology related book, with a link to the publisher. We will post the book on the appropriate books page, as well as on the New Books and Author pages. We will also include it in our Website News / New Books email. There is a 20% discount for posting 3 or more books. There is no charge to post a book which is sold through Amazon.com
(2) As a result of CAP '11 suggestions, we are working on: (a) finishing the Home Page Topic search by October 31, 2011; (b) more frequent reviews / updates of topics (ongoing); (c) developing a new format for viewing the website on an iPad or Smartphone; (d) possibly developing more social media discussions. Let us know what you think.
(3) Thanks to Dr. Perry Cohen, Montefiore Medical Center of the Albert Einstein College of Medicine, for his suggestion to post Cases of the Week by Category without a diagnosis, which has now been done.
(4) We posted an article on our Management Page, How to Gain a Better Managed Care Contract for your Independent Laboratory, by Mick Raich, Vachette Pathology, click here.
Case of the Week #218
Clinical History:
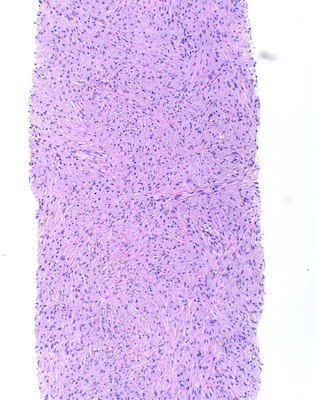
A 35 year HIV+ man had diffuse lymphadenopathy (retroperitoneal, paraaortic, supraclavicular, inguinal and mesenteric) and increased FDG uptake on PET CT. His left supraclavicular node was 3.1 cm. A CT guided biopsy of a retroperitoneal lymph node was performed.
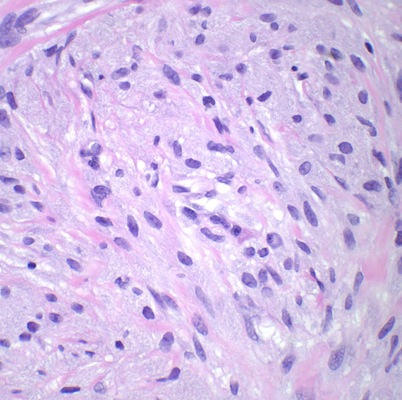
Micro images:

What is your diagnosis?
Diagnosis:
Mycobacterial spindle cell pseudotumor of lymph nodes
Discussion:
Mycobacterial spindle cell pseudotumor of lymph nodes is a disorder associated with HIV+ patients, often with involvement of many sites. It may also affect infants after bCG vaccination (Zhonghua Bing Li Xue Za Zhi 2001;30:89) or occur post-transplant (Am J Clin Pathol 1985;83:524).
Morphologically, the lymph nodes show a partial or complete effacement with a storiform pattern of bland spindle cells, some with vacuoles. There are also numerous vessels lined by plump endothelial cells, plasma cells and lymphocytes. There are no multinucleated tumor cells and no foamy histiocytes. The spindle cells are actually macrophages with large numbers of mycobacteria (Am J Surg Pathol 1992;16:276). Intraoperative touch imprints demonstrate numerous intracellular organisms (Arch Pathol Lab Med 1995;119:811).
The tumor cells are immunoreactive for CD68, S100 and AFB and negative for CD34:
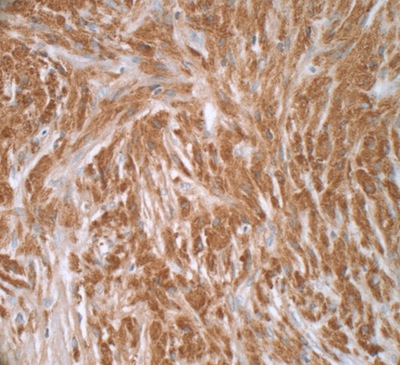
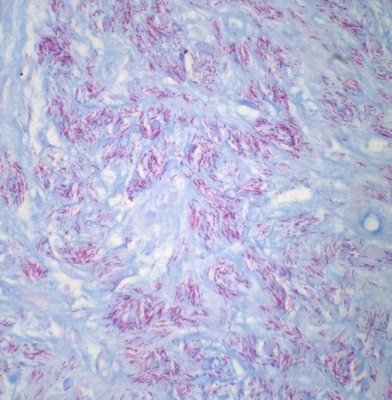
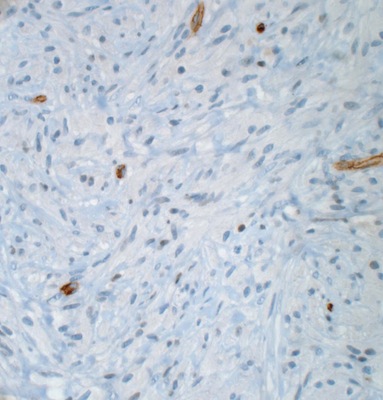
Left to right: S100, AFB, CD34
The differential diagnosis includes:
● Kaposi's sarcoma: has slit-like spaces and mitotic figures; cytoplasm is not granular or acidophilic; spindle cells are CD31+ and CD34+, but negative for S100, CD68 and AFB (Am J Surg Pathol 1999;23:656)
● Smooth muscle tumor: positive for actin and desmin, negative for S100, CD68 and AFB
Treatment consists of antiretroviral therapy for HIV and antibiotics.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email:
NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com