
8 May 2008 - Case #118
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Vincent Graffeo, Peninsula Medical Center, Salisbury, Maryland, USA.
Case #118
Clinical history:
A 60 year old man had a several year history of moderate to severe right lower leg edema, relieved at rest in the evening while lying down. Physical exam revealed right inguinal lymphadenopathy. An excisional lymph node biopsy was performed.
Microscopic images:



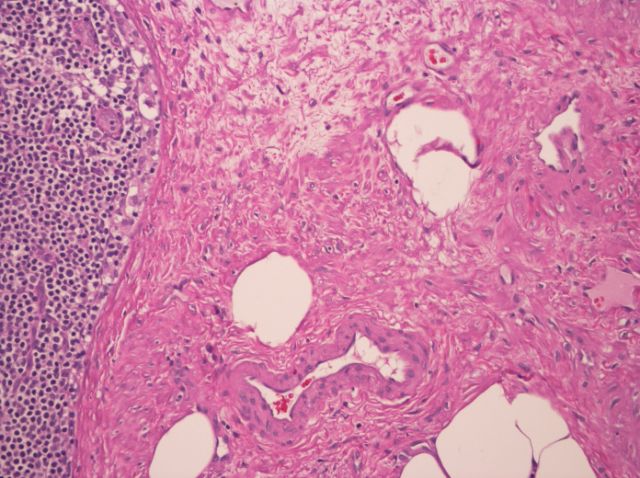
What is your diagnosis?
Diagnosis: Angiomyomatous hamartoma of lymph node
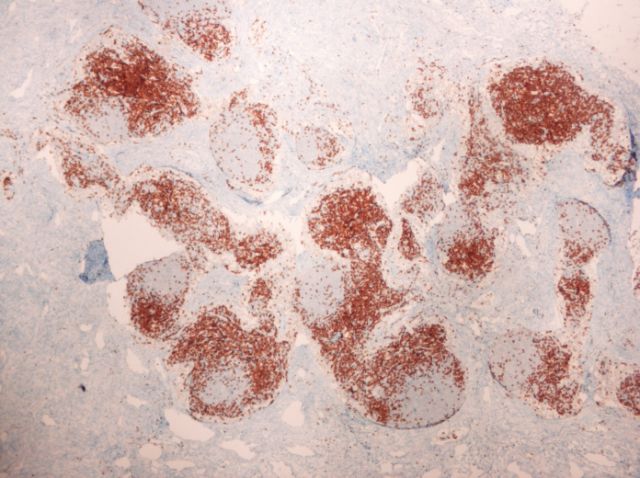
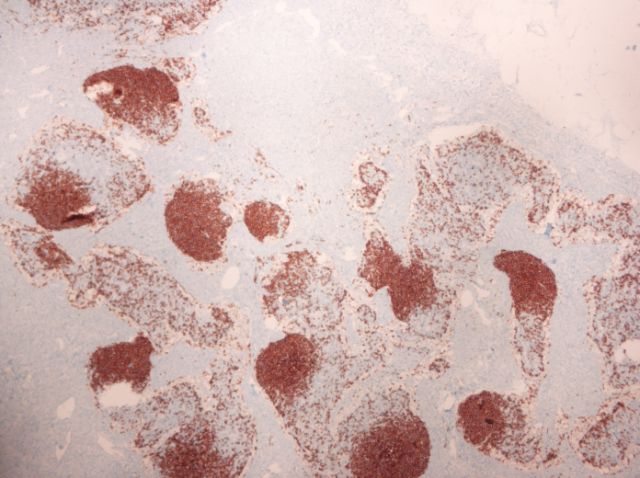
Stain images:
Discussion:
Sections show a lymph node with an effaced architecture. The nodal tissue is partially replaced by a proliferation of smooth muscle, dilated and ectatic vessels and sclerotic stroma, with residual nodules of lymphoid tissue. The lymphocytes are small and mature, with larger transformed cells and a few germinal centers. There are patent sinuses with moderate sinus histiocytosis. The thick walled vessels are more prominent in the hilum and there is a small amount of mature adipose present. CD3 and CD20 immunostains demonstrate an unremarkable mixture of T and B lymphocytes in the nodules. Flow cytometry was negative for a monotypic B cell population.
Angiomyomatous hamartoma, first described in 1992, is a rare, benign smooth muscle proliferation with a predisposition for inguinal lymph nodes (Am J Surg Pathol 1992;16:335). Patients of varying ages are affected, with a male predominance. The lymph nodes are enlarged and may be matted. Ipsilateral limb edema often accompanies this process, which may be long standing. Excision is curative.
Other case reports: 51 year old with 4 cm mass (Pathol Int 2000;50:655), lymph node with significant adipose tissue involvement (Gen Diagn Pathol 1997;143:247).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Vincent Graffeo, Peninsula Medical Center, Salisbury, Maryland, USA.
Case #118
Clinical history:
A 60 year old man had a several year history of moderate to severe right lower leg edema, relieved at rest in the evening while lying down. Physical exam revealed right inguinal lymphadenopathy. An excisional lymph node biopsy was performed.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Angiomyomatous hamartoma of lymph node
Stain images:
CD3
CD20
Discussion:
Sections show a lymph node with an effaced architecture. The nodal tissue is partially replaced by a proliferation of smooth muscle, dilated and ectatic vessels and sclerotic stroma, with residual nodules of lymphoid tissue. The lymphocytes are small and mature, with larger transformed cells and a few germinal centers. There are patent sinuses with moderate sinus histiocytosis. The thick walled vessels are more prominent in the hilum and there is a small amount of mature adipose present. CD3 and CD20 immunostains demonstrate an unremarkable mixture of T and B lymphocytes in the nodules. Flow cytometry was negative for a monotypic B cell population.
Angiomyomatous hamartoma, first described in 1992, is a rare, benign smooth muscle proliferation with a predisposition for inguinal lymph nodes (Am J Surg Pathol 1992;16:335). Patients of varying ages are affected, with a male predominance. The lymph nodes are enlarged and may be matted. Ipsilateral limb edema often accompanies this process, which may be long standing. Excision is curative.
Other case reports: 51 year old with 4 cm mass (Pathol Int 2000;50:655), lymph node with significant adipose tissue involvement (Gen Diagn Pathol 1997;143:247).
