![]()
4 January 2008 Case of the Week #106
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly) and new books (monthly). You must subscribe or unsubscribe separately to these email lists.

![]()
ARUP Laboratories First Annual Winter Update in Clinical and Laboratory Medicine is scheduled for March 3-7, 2008 at The Canyons, in Park City, Utah.
This 22.5 hour review and update in the areas of clinical chemistry, immunology, microbiology, and molecular medicine is intended to improve knowledge about the pathogenesis and clinical manifestations of a wide variety of metabolic infectious, immunologic, and genetic disorders along with the selection, performance, and interpretation of clinical laboratory tests.
This course will provide a forum for the exchange of ideas among clinicians, clinical and anatomic pathologists, and laboratory scientists on new developments diagnosing these disorders. Ample discussion time will be provided to address controversial issues.
For more information, please click here.
We have new email addresses, due to problems with our server email. Please use NatPernick@Hotmail.com or NatPernick@gmail.com for future correspondence.
We thank Drs. Angie M. Schultz and Paul F. Mellen, Ball Memorial Hospital, Muncie, Indiana (USA) for contributing this case and the discussion. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) for your time after we send out the case. Please only send cases with a definitive diagnosis, and preferably cases that are out of the ordinary.
Case of the Week #106
Clinical History
At 35 weeks gestational age, this female fetus had evidence of intrauterine distress and underwent emergent delivery. The abdomen was markedly distended and the fetus did not survive delivery.
Autopsy showed a slightly large for gestational age, well-developed fetus. The general external appearance was unremarkable except for abdominal distension. The placenta was unremarkable. The pertinent findings were limited to the abdominal cavity.
Gross images: abdominal cavity; small intestine
{kind=link}
{kind=link}
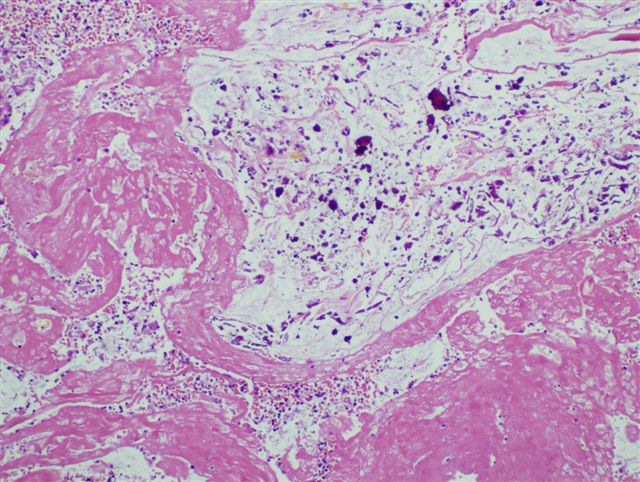
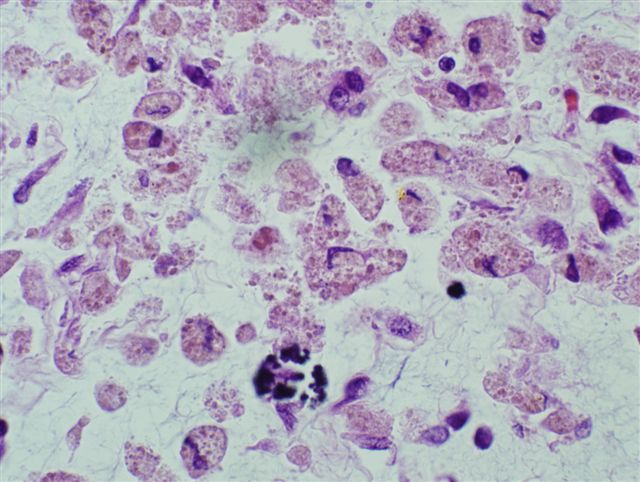
Micro images: peritoneal surface #1; #2
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Meconium peritonitis, associated with intrauterine small intestinal volvulus
Discussion
Meconium peritonitis is a rare prenatal complication, occurring in 1 per 30,000 live births (1). Gastrointestinal perforation releases meconium into the abdominal cavity, inducing a sterile inflammatory reaction and calcium deposition. Perforation may be due to meconium ileus, atresia, stenosis, internal hernia, Hirschprungs disease, volvulus, congenital bands, anoxia leading to bowel ischemia, or idiopathic (2).
The presenting symptoms include fetal distress, maternal polyhydramnios, abdominal distention or a mass (3). Prenatal ultrasound shows bowel dilatation, ascites, polyhydramnios, and intra-abdominal calcifications with acoustic shadowing (4, 10).
Grossly, there is an organized peritonitis with fibrosis, calcifications and dense intestinal adhesions. A fibrous wall, called a meconium pseudocyst, may form around the meconium (5).
Microscopically, the peritoneal surface shows a fibrinous exudate with microcalcifications, bile pigment-like debris, histiocytes and chronic inflammatory cells.
Treatment for meconium peritonitis is surgical, and prognosis varies greatly depending on pre- versus postnatal diagnosis. Gestational age at diagnosis does not predict postnatal outcome (4). However, some prenatal ultrasound findings have been shown to correlate with neonatal outcome in several studies (4,6,7,8).
Since patients in the Western hemisphere with meconium peritonitis often have cystic fibrosis and meconium ileus, newborns with this diagnosis should be evaluated for cystic fibrosis (9, 11).
1. Yang W, Ho S, Metreweli C. Case report: antenatal sonographic diagnosis of meconium peritonitis and subsequent evolving meconium pseudocyst formation without peritoneal calcification. Clin Radiol 1997;52:477
2. Reynolds E, Douglass B, Bleacher J. Meconium peritonitis. J Perinatol 2000;3:193
3. Olnick H, Hatcher M. Meconium peritonitis. JAMA 1953;152:582
4. Dirkes K, Crombleholme T, Craigo S, Latchaw L, Jacir N, Harris B, DAlton M. The Natural History of Meconium Peritonitis Diagnosed In Utero. J Pediatr Surg 1995;30:979.
5. Lauer J, Cradock T. Meconium pseudocyst: prenatal sonographic and antenatal radiologic correlation. J Ultrasound Med 1982;1:333
6. Shyu M, Shih J, Lee C, Hwa H, Chow S, Hsieh F. Correlation of prenatal ultrasound and postnatal outcome in meconium peritonitis. Fetal Diagn Ther 2003;18:255
7. Tseng J, Chou M, Ho E. Meconium peritonitis in utero: prenatal sonographic findings and clinical implications. J Chin Med Assoc 2003;66:355
8. Zangheri G, Andreani M, Ciriello E, Urban G, Incerti M, Vergani P. Fetal intra-abdominal calcifications from meconium peritonitis: sonographic predictors of postnatal surgery. Prenat Diagn 2007;27:960
9. Dahms BB. Pediatric Pathology. 2nd ed. Philadelphia: Stocker & Dehner, 2001:648.
10. Chan KL, Tang MH, Tse HY, Tang RY, Tam PK. Meconium peritonitis: prenatal diagnosis, postnatal management and outcome. Prenat Diagn 2005;25:676
11. Casaccia G, Trucchi A, Nahom A, Aite L, Lucidi V, Giorlandino C, Bagolan P. The impact of cystic fibrosis on neonatal intestinal obstruction: the need for prenatal/neonatal screening. Pediatr Surg Int 2003;19:75
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com