![]()
1 November 2007 – Case of the Week #99
This and other cases can be accessed by visiting our Home Page at www.PathologyOutlines.com and clicking on the Case of the Week button on the left hand side. To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. This means that when we are asked to sell our email lists, we tell them “No!”
We also have emails for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.

This Case is sponsored by Lifepoint informatics, which provides a complete turnkey suite of IT connectivity products for Anatomic Pathology, Hospital, Reference and Independent Laboratories. Our Labtest.com on-line ordering and resulting system helps your lab connect, compete and comply. Our Lifepoint InfoHub connects your LIS/AP system to your client’s EMR systems securely and accurately. For more information, contact www.lifepoint.com, telephone: 866-LABTEST or email: jredding@labtest.com.
We have added Consumer Goods to our Buyer’s Guide. This page now contains many companies with products and services of interest to pathologists and laboratory personnel in both their professional and personal lives. Visit our Buyer’s Guide as your first step when thinking about products to purchase. Don’t forget to also visit our New Products and Services page (click here) for announcements about what’s new.
We thank Dr. Keloth E. Pradeep, Wrexham Maelor Hospital, United Kingdom, for contributing this case. To contribute a Case of the Week, please email info@PathologyOutlines.com with the clinical history, your diagnosis and microscopic images in JPG, GIF or TIFF format (send as attachments, any size, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US dollars) for your time after we send out the case. Please only send cases with a definitive diagnosis, and preferably cases that are out of the ordinary.
Case of the Week #99
Clinical History
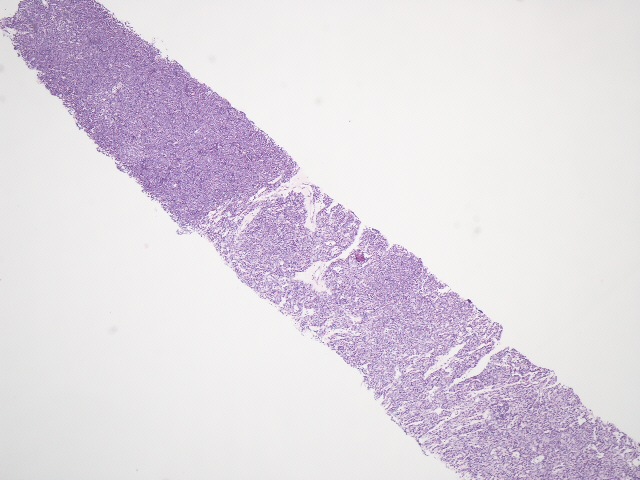
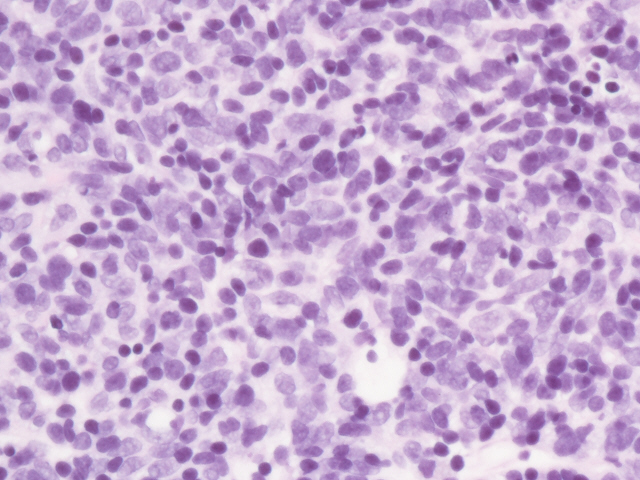
A 70 year old man had a calcified mediastinal mass on chest Xray. A core needle biopsy was taken.
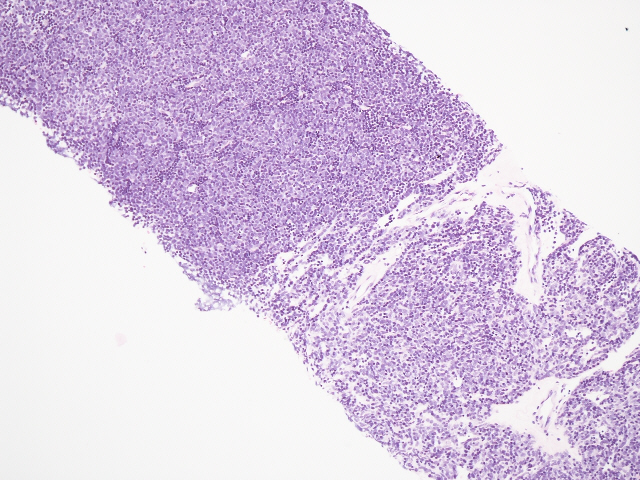
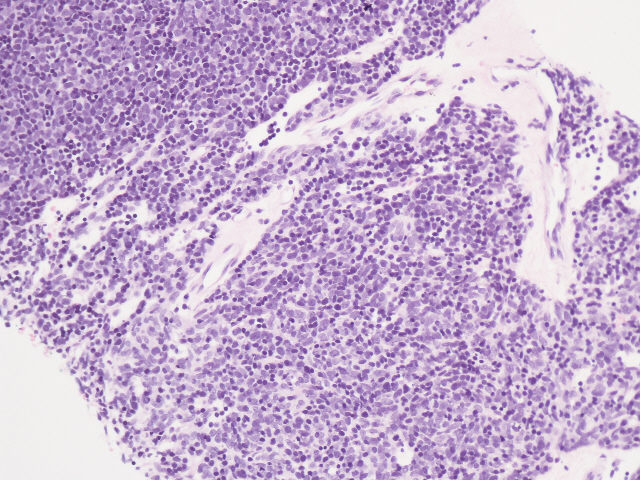
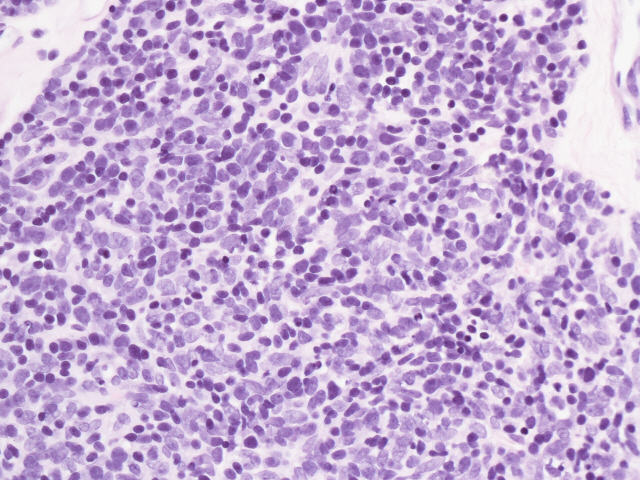
Micro images: #1; #2; #3; #4; #5
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
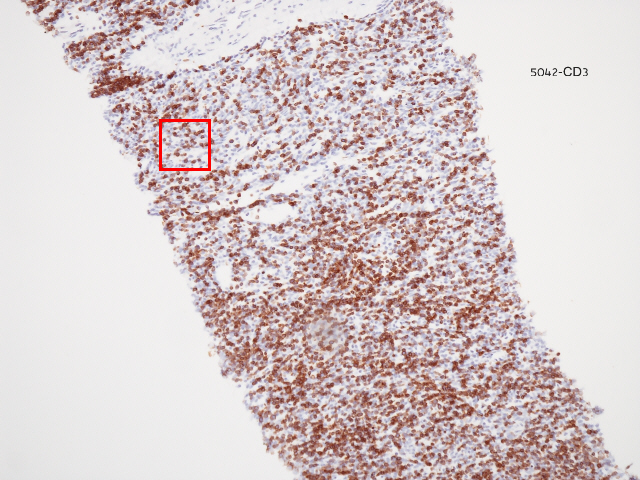
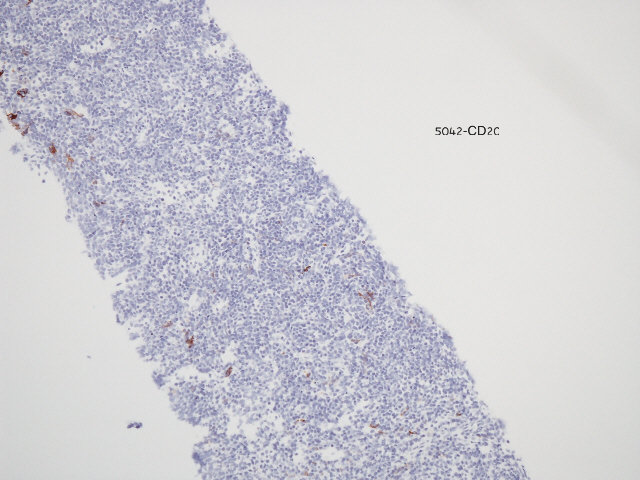
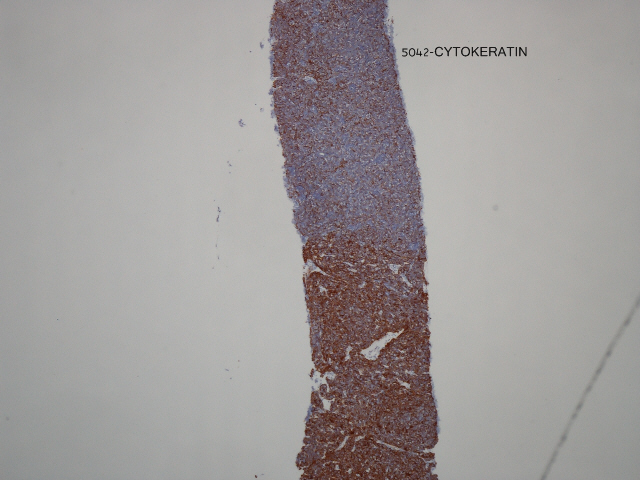
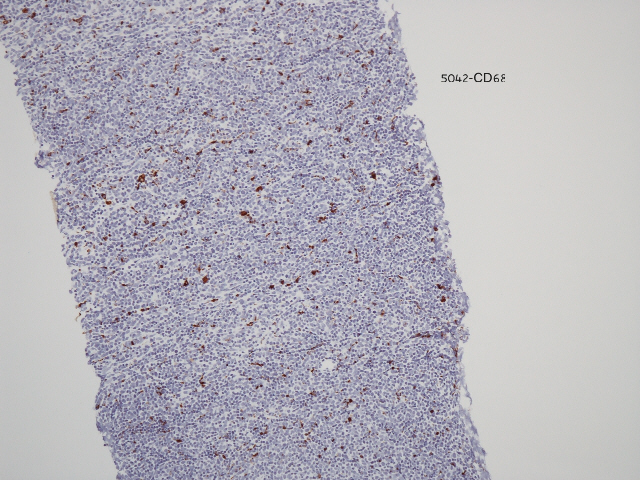
Immunostains: CD3; CD20; keratin; CD68
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Thymoma, B1 type
Discussion
Thymoma is the most common primary anterior mediastinal neoplasm. It is often associated with myasthenia gravis and other immune-mediated disorders.
Morphologically, thymoma is a combination of bland epithelial cells and non-neoplastic lymphocytes. This case was classified as type B1 (WHO) based on the large number of T lymphocytes (CD3+) mixed with epithelial cells (keratin+).
The numerous classification systems of thymoma have been extensively discussed, most recently by Suster and Moran (Am J Clin Pathol 2006;125:542). For prognostic purposes, it is important to distinguish thymoma types that typically have benign behavior (types A, AB, B, B1 and B2), from those with atypical behavior (type B3, Ann Thorac Cardiovasc Surg 2005;11:367) and those that are cytologically malignant (type C, also called thymic carcinoma, AJSP 2002;26:1605).
The differential diagnosis of this lymphocyte rich type of thymoma is primarily lymphoblastic lymphoma and thymic lymphoid hyperplasia. Lymphoblastic lymphoma typically presents in teenagers or young adults. In contrast to thymoma, the lymphocytes are malignant and the epithelial component, if present, represents trapped normal epithelial cells. Careful use of immunostains is necessary to avoid misdiagnosis. Thymic lymphoid hyperplasia is also associated with myasthenia gravis, but typically does not produce a mass. Lymphoid follicles are present with normal germinal centers, but the pattern of epithelial cells may be disrupted. In some cases, the differential diagnosis of thymoma may also include thymic carcinoid tumor (if rosettes are present), or Castleman’s disease.
As an aside, we are pleased that American Journal of Clinical Pathology is now providing articles that are free full text, no registration, after 1 year from publication. Other free full text, no registration pathology journals that we find particularly useful are Archives of Pathology and Laboratory Medicine (always free) and Modern Pathology (free after 1 year from publication).
Additional references: Mediastinum chapter of PathologyOutlines.com
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com