![]()
25 October 2007 – Case of the Week #98
This and other cases can be accessed by visiting our Home Page at www.PathologyOutlines.com and clicking on the Case of the Week button on the left hand side. To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.

This Case is sponsored by Milestone Medical, the technological leader in Microwave Accelerated Tissue Processing. Milestone manufactures instrumentation and accessories that enable Histologists and Pathologists to achieve the highest level of productivity, while maintaining their flexibility and safety.
Milestone’s family of rapid microwave lab stations allow tissue samples to be processed in a fraction of the time as compared to conventional methods, allowing for same-day diagnosis. Milestone also offers a line of digital imaging equipment for grossing stations and autopsy rooms. These systems serve as a comprehensive method of storing macroscopic images of all specimens examined in the laboratory, providing an invaluable diagnostic database for routine grossing, teaching, and research.
For more information, please visit Milestone’s website by clicking here.
We thank Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), for contributing this case. To contribute a Case of the Week, please email info@PathologyOutlines.com with the clinical history, your diagnosis and microscopic images in JPG, GIF or TIFF format (send as attachments, any size, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US dollars) for your time after we send out the case. Please only send cases with a definitive diagnosis, and preferably cases that are out of the ordinary.
Case of the Week #98
Clinical History
An 18 year old man with cystic fibrosis and Burkholderia dolosa infection presented with increasing fever, vomiting, dyspnea and cough. He previously was treated with multiple antibiotics, including tobramycin, minocycline, meropenem, and levofloxacin. He continued to have worsening respiratory status, and died shortly afterwards. At postmortem examination, the following findings were noted:
{kind=link}
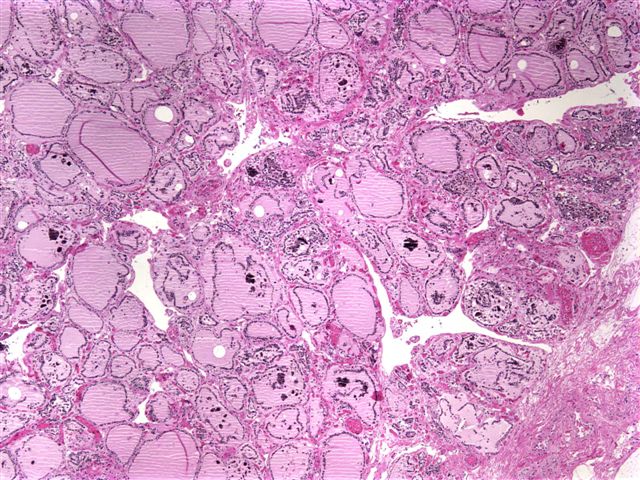
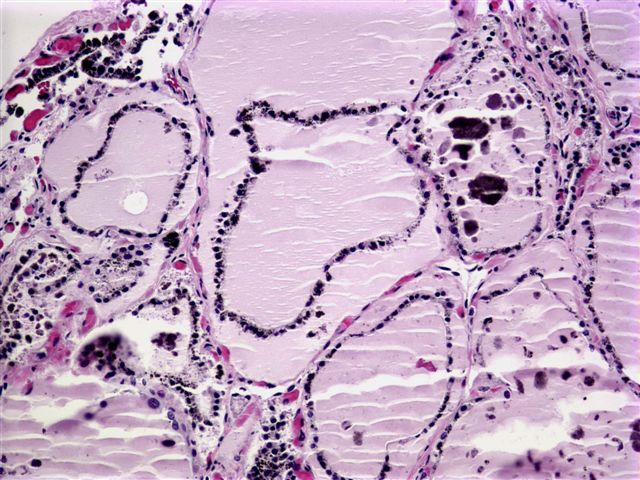
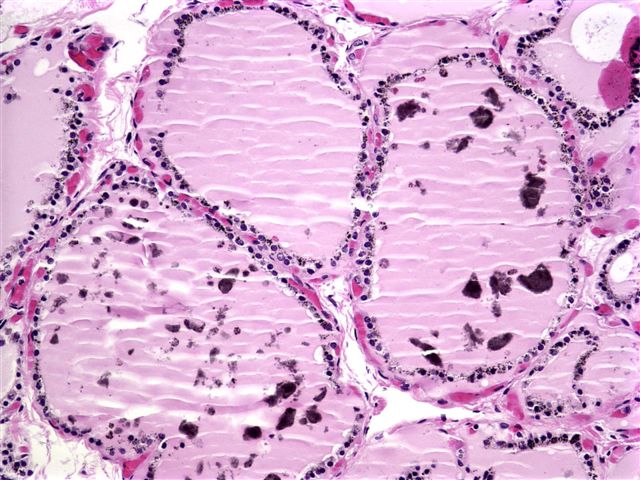
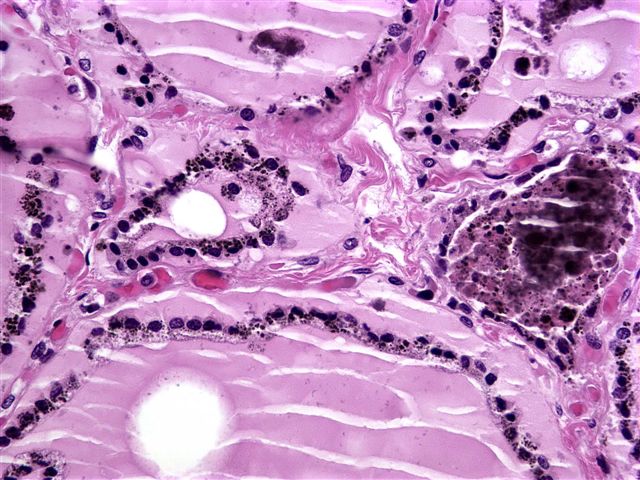
Micro images: image #1; #2; #3; #4
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Minocycline associated “black thyroid”
Discussion
Black thyroid due to pigment deposition is a well known side effect of minocycline (tetracycline) treatment. Pigment may also be deposited in bone and oral mucosa (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:718), and a similar effect from doxycycline has been reported (Head Neck 2006;28:373).
The pigment may be within thyroid epithelium, colloid or macrophages. Its exact nature is controversial. It stains with Fontana-Masson, resembling melanin. It has also been characterized as lipofuscin (AJCP 1983;79:738, Hum Path 1985;16:72), which may be an oxidative product of minocycline, due to its competitive inhibition with thyroid peroxidase.
Black thyroid may also be due to doxepin, lithium carbonate or tricyclic antidepressants. In these patients, the pigment is thought to be due to lysosomal accumulation of drug, not oxidation (Archives 2004;128:355).
Many reports have suggested that black thyroid is associated with thyroid pathology, but no clear relationship has yet been established. However, as papillary thyroid carcinoma in black thyroid is often unpigmented, hypopigmented foci should be thoroughly examined (Mod Path 1999;12:1181).
Despite the striking histologic findings, no specific cytologic findings have been described after fine needle aspiration (Diagn Cytopathol 2006;34:106).
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com