![]()
11 October 2007 Case of the Week #97
This and other cases can be accessed by visiting our Home Page at www.PathologyOutlines.com and clicking on the Case of the Week button on the left hand side. To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.

This Case is sponsored by Lifepoint informatics, which provides a complete turnkey suite of IT connectivity products for Anatomic Pathology, Hospital, Reference and Independent Laboratories. Our Labtest.com on-line ordering and resulting system helps your lab connect, compete and comply. Our Lifepoint InfoHub connects your LIS/AP system to your clients EMR systems securely and accurately. For more information, contact www.lifepoint.com, telephone: 866-LABTEST or email: jredding@labtest.com.
We thank Dr. Hanni Gulwani, Sir Ganga Ram Hospital, New Delhi (India), for contributing this case. To contribute a Case of the Week, please send an email to info@PathologyOutlines.com with the clinical history, your diagnosis and microscopic images in JPG, GIF or TIFF format (send as attachments, any size, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US dollars) for your time after we send out the case. Please only send cases with a definitive diagnosis, and preferably cases that are out of the ordinary.
Case of the Week #97
Clinical History
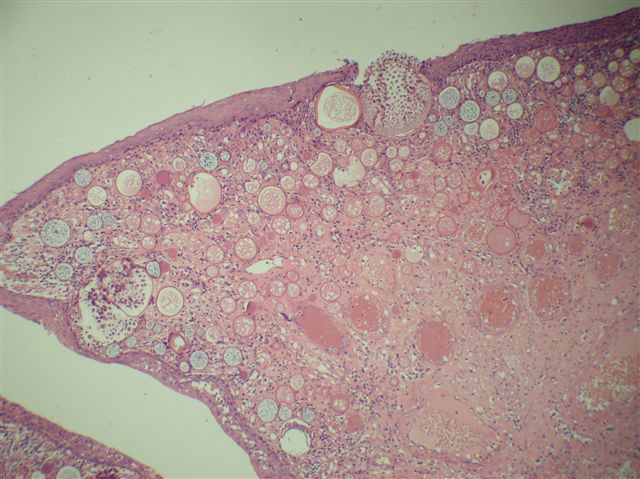
A 29 year old man from India presented with progressively increasing nasal obstruction for 6 months. A mass was excised.
Micro images: image #1; #2; #3
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
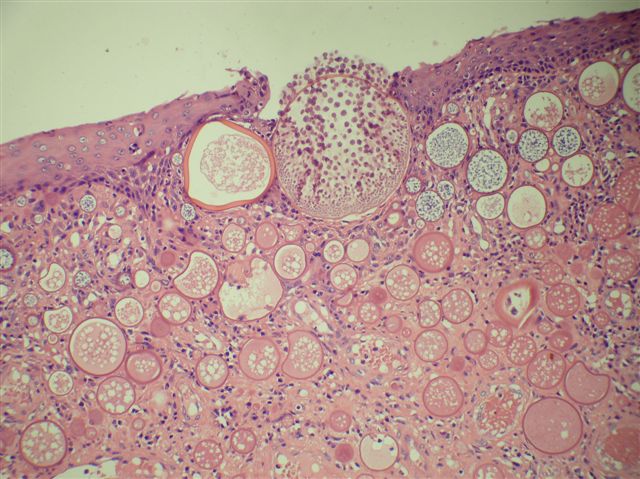
Rhinosporidiosis
Discussion
Rhinosporidiosis is caused by Rhinosporidium seeberi, traditionally thought to be a fungus, but actually an aquatic protistan parasite (J Clin Microbiol 1999;37:2750, Emerg Infect Dis 2000;6:273, Indian J Med Microbiol 2002;20:119). It is endemic in southern India and Sri Lanka and occurs in emigrants from this region (Diagn Pathol 2006;1:25, Singapore Med J 2004;45:224), but a few indigenous cases in the US have also been reported (South Med J 1996;89:65). Rhinosporidium seeberi has a natural aquatic habitat, and is transmitted through traumatized epithelium, most commonly in the nose and eye, but also in the skin, ear, genitals and rectum. Bathing or working in stagnant water is a risk factor. It rarely presents with disseminated skin disease (Indian J Dermatol Venereol Leprol 2007;73:185, Indian J Dermatol Venereol Leprol 2001;67:332). It is not transmitted person to person.
In the nose, it presents as hyperplastic, polypoid, red, granular masses. Yellow pinhead spots represent mature sporangia. Superficial mucus is common. Microscopically, there are large (100 to 450 microns), thick walled sporangia containing over 1000 endospores that are each 6-10 microns, accompanied by a mixed inflammatory infiltrate. These structures may not be present in all portions of the tissue, and additional sampling may be needed for diagnosis. The organisms are stained by GMS and PAS.
The differential diagnosis includes myospherulosis and other fungi. Myospherulosis is an iatrogenic lipogranuloma caused by hemostatic packing of the nasal cavity or paranasal sinuses with a petrolatum based ointment and gauze. Histologically, large tissue spaces are identified with saclike structures containing brown spherules that resemble Prototheca but are actually clumped red blood cells which do not stain with GMS. Coccidiodes immitis also has spherules and endospores, but they are smaller (spherules: 30-60 microns, endospores: 2-5 microns), and arthroconidia and hyphae may also be found.
Treatment is surgical excision, but recurrences are common. There is currently no effective medical treatment.
Additional references: eMedicine
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com