![]()
11 October 2007 – Case of the Week #97
This and other cases can be accessed by visiting our Home Page at www.PathologyOutlines.com and clicking on the Case of the Week button on the left hand side. To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.

This Case is sponsored by Lifepoint informatics, which provides a complete turnkey suite of IT connectivity products for Anatomic Pathology, Hospital, Reference and Independent Laboratories. Our Labtest.com on-line ordering and resulting system helps your lab connect, compete and comply. Our Lifepoint InfoHub connects your LIS/AP system to your client’s EMR systems securely and accurately. For more information, contact www.lifepoint.com, telephone: 866-LABTEST or email: jredding@labtest.com.
We thank Dr. Michael W. Robles, AmeriPath North Texas (USA), for contributing this case. To contribute a Case of the Week, please email info@PathologyOutlines.com with attachments of microscopic images (any size, we will shrink if necessary) in JPG, GIF or TIFF format, a clinical history, your diagnosis and any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US) for your time after we send out the case. Please only send cases with a definitive diagnosis.
Case of the Week #95
Clinical History
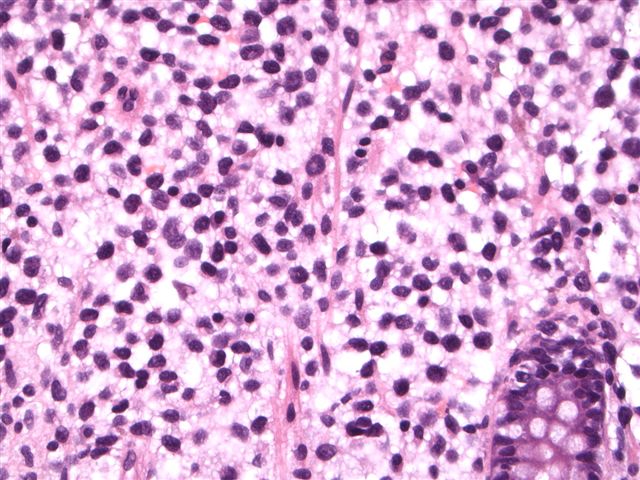
The patient was a 55 year old man with a history of colon polyps, diverticulosis and hypertrophy of the anal papillae. At routine colonoscopy, no polyps were found, but there was a 2 cm nodular patch in the cecum, which was biopsied.
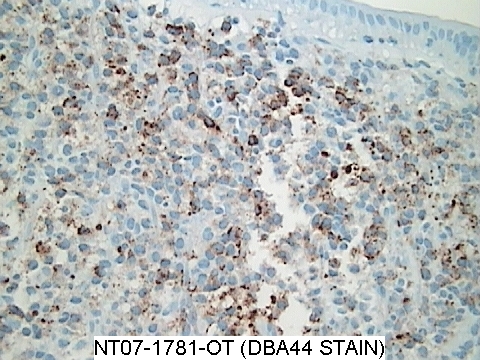
Micro images: image #1; #2; immunostain for DBA.44
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Consistent with hairy cell leukemia
Discussion
Multiple fragments of nodular colonic mucosa demonstrate mucosal and submucosal infiltrates of small and medium lymphocytes with abundant pale cytoplasm and oval, indented nuclei. The lymphocytes were immunoreactive for CD20, DBA.44, CD68, cyclinD1/bcl1 (patchy) and Ki-67 (mildly increased proliferation index). They were negative for CD5. After the biopsy was submitted, the pathologist learned that the patient had a history of hairy cell leukemia.
Hairy cell leukemia is a rare, chronic B cell lymphoproliferative disorder, usually affecting older white men (mean age 52 years), who present with massive splenomegaly with red pulp involvement and obliteration of the white pulp. There is often pancytopenia (50%) and infections (30%), but usually minimal lymphadenopathy. Bone marrow aspiration biopsies are often unsuccessful due to marrow fibrosis. The peripheral blood shows only rare leukemic cells. Occasional cases may involve the skin or other organs. GI involvement is rare.
The distinctive hairy cell is seen in bone marrow biopsies. It has clear to lightly eosinophilic or basophilic cytoplasm, with surface projections that may be delicate or broad. There may be cytoplasmic vacuoles or azurophilic granules. The nuclei are oval or indented. Formalin fixed tissue often has a perinuclear halo.
Besides the markers indicated above, the hairy cells are also positive for B cell markers CD19, CD22, CD79a and PAX5, as well as TRAP, CD25 and CD103. Recommended combinations of markers to order include DBA.44 and TRAP, and flow cytometry with CD11c, CD20, CD25 and CD103 (Archives 2007;131:383). Of note, atypical immunophenotyping has been reported in 34% of cases (AJCP 2006;125:251), and a variant type has also been described (AJCP 2005;123:132)
The differential diagnosis includes splenic marginal zone lymphoma and mastocytosis. Splenic marginal zone lymphoma, like hairy cell leukemia, typically involves the spleen, and may have circulating cells with abundant cytoplasm and cytoplasmic processes. In contrast to hairy cell leukemia, the cytoplasmic processes are usually polar, not circumferential, and there is a nodular pattern of splenic white pulp involvement, not obliteration of the white pulp. The cells usually do not express DBA.44, TRAP or CD103. Mastocytosis often involves the spleen, and mast cells also have abundant clear cytoplasm. However, they are negative for B cell markers and positive for toluidine blue, Giemsa, tryptase and CD117.
Treatment of hairy cell leukemia with purine analogs and interferon frequently causes complete responses and a markedly improved disease free survival (Hematol Oncol Clin North Am 2006;20:1153). Due to frequent aberrant staining, it is important to order an adequate number of immunostains, and to correlate histologic, immunohistochemical and clinical findings to ensure the correct diagnosis.
Additional references: eMedicine
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com