![]()
23 August 2007 – Case of the Week #93
This case and other cases can be accessed by visiting our Home Page at www.PathologyOutlines.com and clicking on the Case of the Week button on the left hand side. To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for Pathologist-PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.
Do you use PathologyOutlines.com daily as part of your practice? We are trying to make it as useful as possible for pathologists and laboratory personnel, through our comprehensive textbook and lists of Jobs, Conferences, Fellowships, Books, New Products and Buyers Guide. Please tell us what we could do to make it more useful to you. Contact us at info@pathologyoutlines.com or call Dr. Nat Pernick at 248/646-0325.
We thank Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), for contributing this case. To contribute a Case of the Week, please email info@PathologyOutlines.com with attachments of microscopic images (any size, we will shrink if necessary) in JPG, GIF or TIFF format, a clinical history, your diagnosis and any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US) for your time after we send out the case. Please only send cases with a definitive diagnosis.
Case of the Week #93
Clinical History
A 63 year old woman with an unknown past medical history presented with a right axillary mass and lymphadenopathy. The axillary mass was excised.
Micro images:
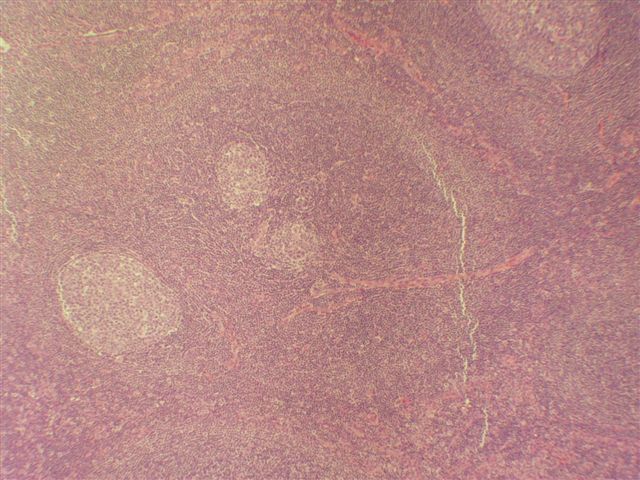
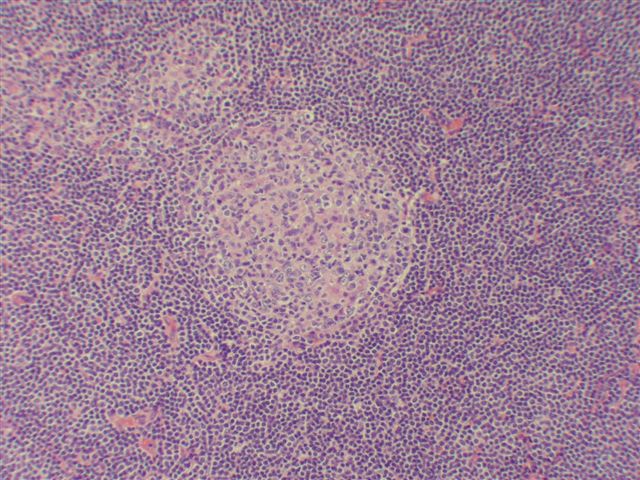
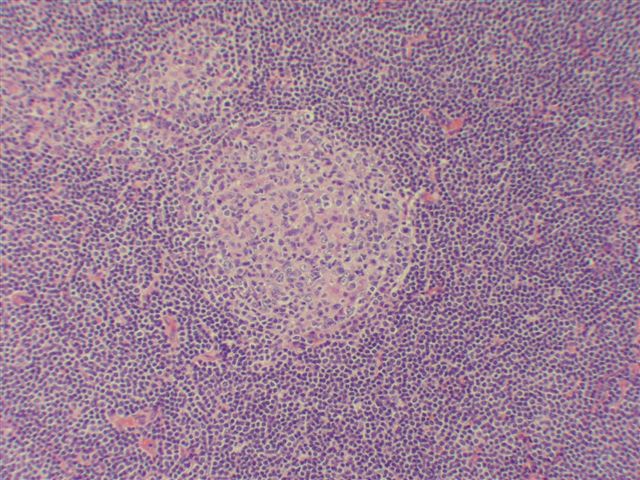
low/medium power - figure 1; figure 2; figure 3
{kind=link}
{kind=link}
{kind=link}
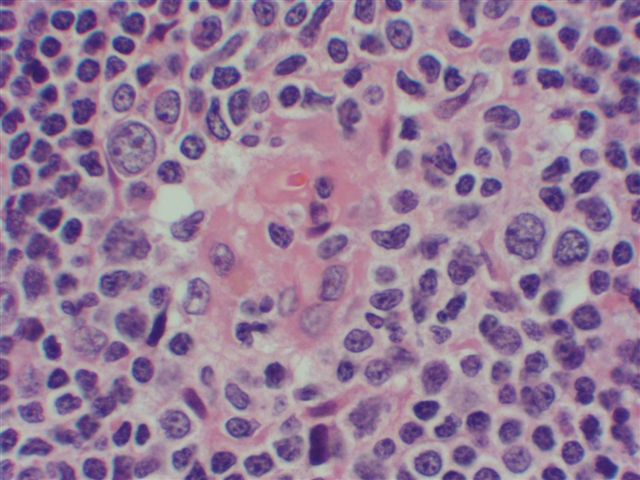
high power - figure 4; figure 5
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Castleman’s disease, hyaline-vascular variant
Discussion
Castleman’s disease, also known as giant lymph node hyperplasia or angiofollicular hyperplasia, is a rare lymphoproliferative disorder of unknown etiology with hyaline vascular, plasma cell and mixed variants. Most cases are polyclonal (Histopathology 2006;48:233). It may be solitary or multicentric (Acta Oncol 2004;43:698). Solitary masses often are mediastinal and asymptomatic, and 90% are hyaline-vascular subtype. Multicentric disease presents with generalized lymphadenopathy, and is almost always plasma cell subtype. It may be associated with the POEMS syndrome (Polyneuropathy, Organomegaly, Endocrinopathy, M-protein and Skin). In this case, although the disease appeared to be multicentric (the lymph nodes were not biopsied), the subtype was hyaline-vascular.
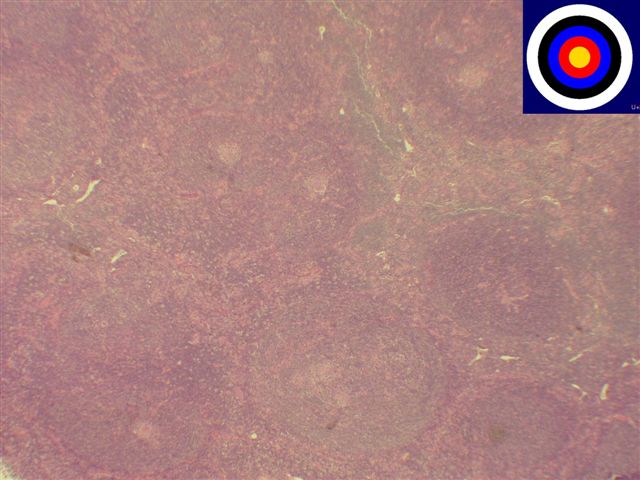
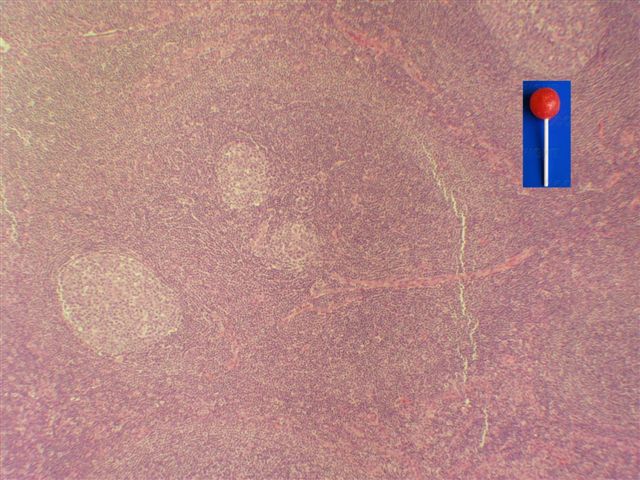
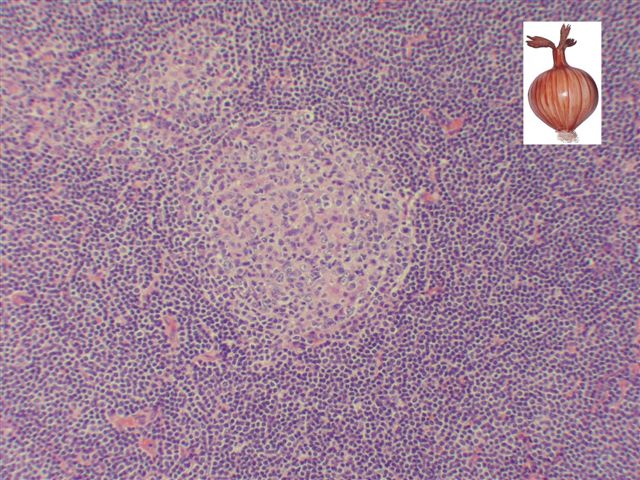
The hyaline vascular (angiofollicular) subtype has prominent follicles within lymphoid tissue but no sinuses, and a low power targetoid pattern (image). The appearance may resemble a lollipop (image). The follicles have a marked vascular proliferation with thick and hyalinized vessel walls and hyalinized germinal centers which resemble thymic Hassall’s corpuscles or splenic white pulp, but are actually regressed (involuted) germinal centers. They often have an onion-skin pattern of lymphocytes (image), and may contain large cells with prominent nucleoli (CD21+, CD35+ follicular dendritic cells, Diagn Cytopathol 2000;22:230). Frequently, a capillary is found that penetrates the follicle. On fine needle aspirate, large histiocytic cells with nuclei resembling crumpled tissue paper are seen in a background of small lymphocytes (Cytopathology 2007;18:168)
{kind=link}
{kind=link}
{kind=link}
The plasma cell variant also has follicular hyperplasia with large germinal centers, but with diffuse plasma cells between follicles. It is associated with HHV8 infection (AJSP 2003;27:91). In addition, a plasmablastic variant has been described (Blood 2000;95:1406)
The differential diagnosis includes follicular lymphoma, follicular hyperplasia, progressive transformation of germinal centers (APMIS 2005;113:288), HIV lymphadenopathy and mantle cell lymphoma.
Surgical excision is usually adequate for solitary lesions. For multicentric lesions, the optimal treatment is unknown, although anti-IL6 therapy has shown promising results (Intern Med 2007;46:771)
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com