![]()
2 August 2007 Case of the Week #91
These cases can also be accessed by clicking on the Case of the Week button on the left hand side of our Home Page at www.PathologyOutlines.com. To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration.
This email is sent only to subscribers. To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for Pathologist jobs (biweekly), non-pathologist laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.
We recently posted a new chapter on Clinical Chemistry, which initially contains information on thyroid function tests. A sample entry is below:
Thyroid stimulating hormone receptor antibody
Also called TRAb (TSH Receptor Antibody)
Previously called thyroid stimulating immunoglobulin or long acting thyroid stimulators (LATS)
Present in 85-95% with Graves disease
Either stimulating (causing hyperthyroidism), blocking (usually no clinical impact) or no effect
Antibodies cross placenta and may cause thyroid dysfunction in newborns
Indications: not for routine clinical testing; to confirm Graves disease in difficult cases, monitor hormone replacement therapy, diagnose neonatal thyrotoxicosis
Methodology: thyrotropin binding inhibiting immunoglobulin technique, RIA
Reference ranges: negative - 0-9%, indeterminate - 10-15%, positive - 16% or more
Interpretation: positive results are consistent with autoimmune disease; low antibody titer before drug therapy for Graves disease is a good prognostic factor for remission after drug therapy (Horm Metab Res 2004;36:92) or relapse (Horm Metab Res 2007;39:56), predicts risk of thyroid dysfunction in newborns of mothers with Graves disease
References: J Clin Invest 2005;115:1972
We thank David E. Georgi, M.D. and Preetha Ramalingam, MBBS, Medical College of Georgia (USA), for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case of the Week #91
Clinical History
A 44 year old woman with previous cervical biopsies showing CIN II-III had a cervical loop-cone biopsy. The specimen showed focal residual CIN I with HPV changes arising in a background of focally atypical immature squamous metaplasia. Resection margins were free of dysplasia. The patient had no other significant past medical history.
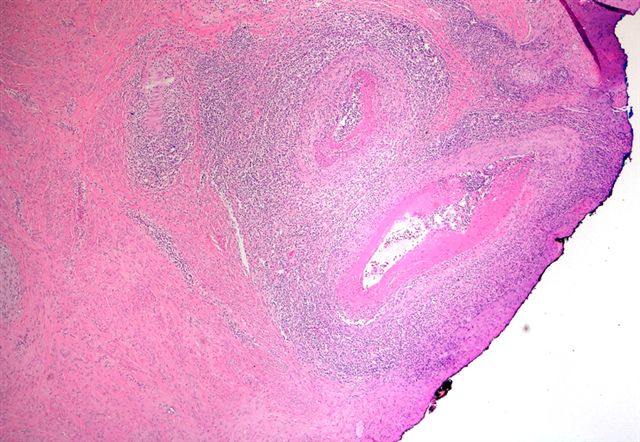
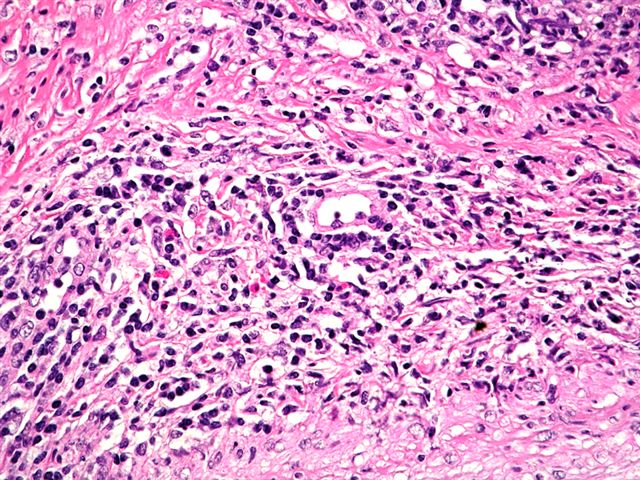
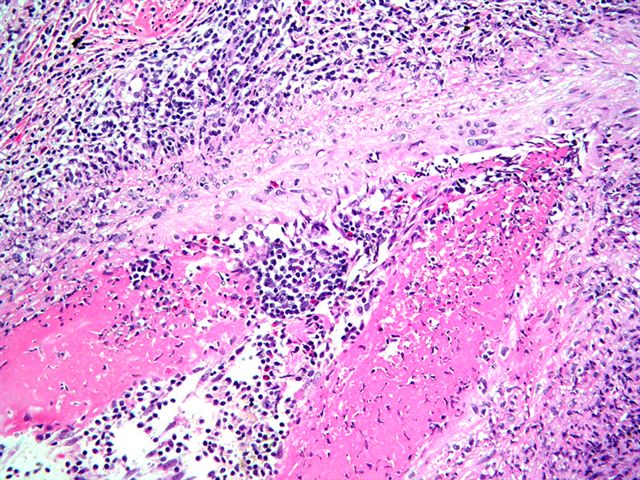
However, deep within the cervical stroma, two muscular arteries were noted to have a marked inflammatory infiltrate in the vessel wall (Figure 1, H&E, 100x), containing acute and chronic inflammatory cells including lymphocytes, neutrophils, and occasional eosinophils (Figure 2, H&E, 400x). Approximately half of the vessel circumference had fibrinoid necrosis within the media (Figure 3, H&E, 200x). No giant cells were noted. There was no adjacent cervicitis.
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Isolated Polyarteritis Nodosa of the Cervix
Discussion
Polyarteritis Nodosa (PAN) is a rare primary vasculitis, usually of unknown etiology, that affects muscular arteries at branch points. It produces lesions of varying stages of evolution, as well as aneurysms. It usually affects the kidney and GI tract. Two-thirds of patients are male, and most are age 50 years or older.
Isolated PAN of the female genital tract is rare. Abu Farsakh et al reported 2 cases of isolated vasculitis involving the female genital tract and compared them with prior cases. They divided necrotizing arteritis into a giant cell arteritis type, which primarily affected post-menopausal women in any part of the female genital tract; and a PAN-type vasculitis, which affected the cervix of younger women, similar to our patient.1 Since this patient had only a loop cone, it was not possible to assess the presence of vasculitis elsewhere.
Vasculitis of any type affecting the female genital tract is usually an isolated finding. Ganesan et al studied 46 patients with vasculitis in the female genital tract, with an average followup of 3 years.2 Only four patients initially or subsequently had systemic disease.
The parthenogenesis of PAN is unclear. The inflammatory cells are mainly T lymphocytes and macrophages 3. An isolated necrotizing arteritis appears to be immune complex-mediated.
The patient in this case has been followed for 17 months, and has not progressed to systemic PAN. It is important to recognize isolated PAN of the female genital tract as an entity so that it is not mistaken for systemic vasculitis. On the other hand, an appropriate workup may be helpful to rule out the rare systemic cases.
References
1. Abu-Farsakh H, Mody D, Brown RW, Truong LD. Isolated Vasculitis involving the female genital tract; clinicopathologic spectrum and phenotyping of inflammatory cells. Mod Pathol 1994;7:610.
2. Ganesan R, Ferryman SR, Meier L, Rollason TP. Vasculitis of the female genital tract with clinicopathologic correlation: a study of 46 cases with follow-up. Int J Gynecol Path 2000;19:258.
3. Francke ML, Mihaescu A, Chaubert P. Isolated necrotizing arteritis of the female genital tract: a clinicopathologic and immunohistochemical study of 11 cases. Int J Gynecol Path 1998;17:193.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com