![]()
26 April 2007 Case of the Week #81
These cases can also be accessed by clicking on the Case of the Week button on the left hand side of our Home Page at www.PathologyOutlines.com. This email is sent only to subscribers. To view the images or references, you must click on the links in blue.
To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have emails for new Pathologist jobs (biweekly), new other Laboratory jobs (biweekly), website news (monthly), new books (monthly), and a newsletter (twice a year). You must subscribe or unsubscribe separately to these email lists.

Bond fully automated IHC and ISH
This case is sponsored by Vision BioSystems, whose fully automated Bond system is improving the quality and workflow of IHC and ISH staining. With complete automation and specially developed reagents (including ready-to-use antibodies), the Bond system eliminates unnecessary manual handling and ensures consistency at every step.
Bond also has a unique continuous processing capability with three independent slide trays. This allows laboratories to start slides as soon as they are ready while retaining capacity to add more slides at any time. Continuous processing ensures stained slides are ready exactly when they are needed.
Bond is part of Vision BioSystems Lean Histology range and it is ideal for laboratories pursuing Lean and six sigma principles. For more information on the Bond system, visit our website www.vision-bio.com.
We thank Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), for contributing this case and the discussion. We invite you to contribute a Case of the Week by emailing info@PathologyOutlines.com with microscopic images (any size, we will shrink if necessary) in JPG or TIFF format, a clinical history, your diagnosis and any other images (gross, immunostains, EM, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US dollars) for your time after we send out the case. Please only send cases with a definitive diagnosis.
Case of the Week #81
Clinical History
A 36 year old man was admitted to an outside institution with a one month history of nausea, vomiting, diarrhea and abdominal pain. He also had a 30 pound unintentional weight loss, anorexia and fatigue. He did not experience early satiety, dysphagia, increase in abdominal girth or hematuria, urinary frequency or rash. His past medical history included a cholecystectomy.
The physical exam was entirely within normal limits, with no palpable abdominal mass or lymphadenopathy. Laboratory tests included WBC 17.6, hematocrit 43.8% and platelets 513K. The electrolyte panel was within normal limits. An abdominal CT scan demonstrated a large mass arising from the distal third of the duodenum, with intra and extra-duodenal components (Figure 1). There was mild dilation of the proximal duodenum, suggesting obstruction. Radiologically, a gastrointestinal stromal tumor (GIST) was strongly considered in the differential diagnosis, because of the size and location.
{kind=link}
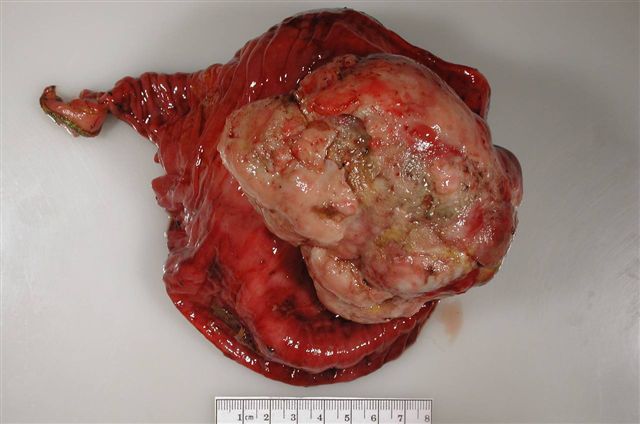
The patient underwent an en-bloc resection of the tumor, partial pancreatectomy, and abdominal and regional retroperitoneal lymphadenectomy.
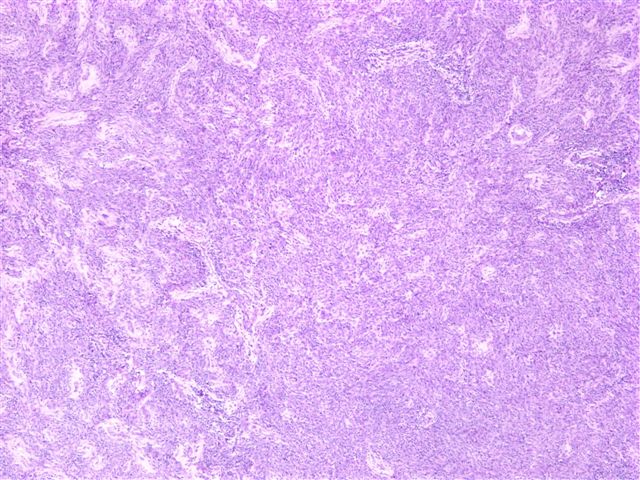
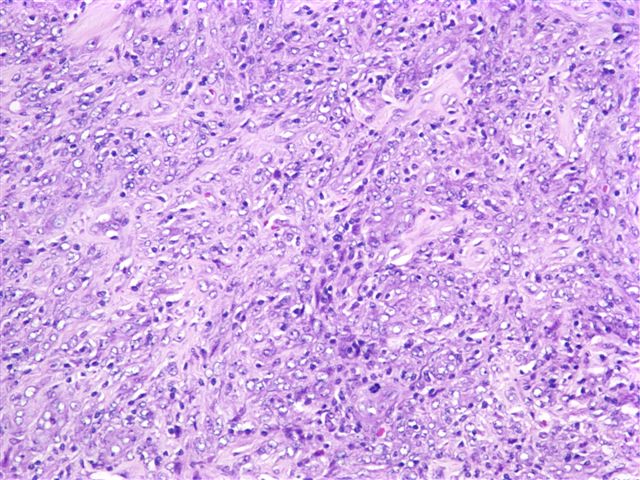
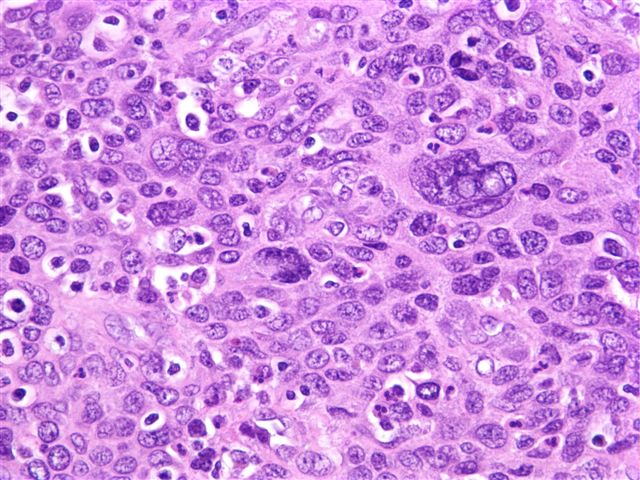
The mass grew into the duodenal lumen and measured 10.5 x 10 x 8 cm (Figure 2). It did not appear to be originating from a lymph node. On H&E, the tumor was predominantly composed of spindle cells with a storiform pattern (Figure 3). Necrosis was present, along with numerous large, hyperchromatic cells and occasional multi-nucleated cells, with a scattering of small lymphocytes (Figure 4, Figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
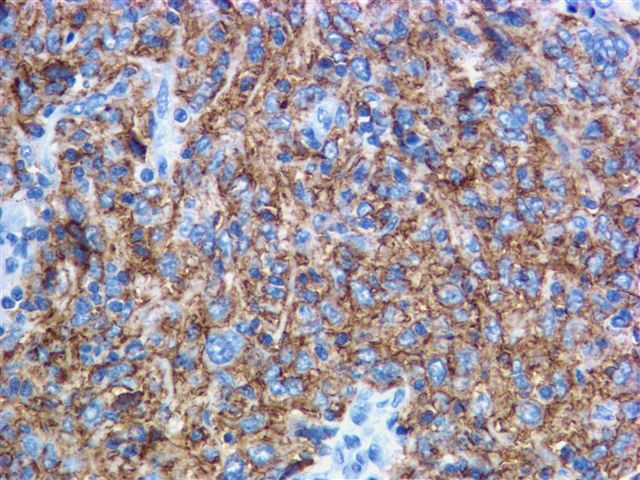
Tumor cells stained dimly for S100, but were negative for c-kit/CD117, HMB45, CD34, desmin and actin. The tumor cells were immunoreactive for CD21 and CD35 (Figure 6).
{kind=link}
What is your diagnosis?
Diagnosis:
Follicular dendritic cell sarcoma
Discussion
Follicular dendritic cell sarcoma is a rare neoplasm, characterized by Monda et al in 1986 7. It usually occurs as a painless, indolent mass. The median age of patients is in their fifth decade, with an age range of 17-76 years 5, and no gender preference. Patients with abdominal involvement may present with pain, but there are usually no constitutional symptoms. It may be associated with Castlemans disease-hyaline vascular type 5, either preceding the sarcoma, or growing separately. It usually involves lymph nodes 3, predominantly cervical, axillary or mediastinal. Extranodal sites include oral cavity, spleen, liver, small intestine, pancreas, peritoneum, soft tissue, and skin. Splenic and hepatic tumors are associated with Epstein Barr virus 1, 6.
These tumors typically recur locally, with occasional distant metastases to liver or lung. In a review by Fletcher et al., it appeared that large tumor size (6 cm or more), intraabdominal location and coagulative necrosis were associated with a higher rate of recurrence, metastasis, and mortality 2.
These tumors are likely to be misdiagnosed unless one thinks of them and tests for follicular dendritic cell markers (CD21 and CD35). The main clinical and pathologic differential diagnosis, particularly within the abdomen, is a gastrointestinal stromal tumor (GIST). GIST and follicular dendritic cell sarcomas share some histologic features, including the fascicular arrangement of spindle cells, the frequent presence of epithelioid cells 4, and occasional S-100 reactivity. However, GISTs are uniformly c-kit positive and usually CD34 positive.
The differential diagnosis also includes fibroblastic reticulum cell sarcoma (vimentin+, smooth muscle actin+, desmin+, CD21-, CD35-), interdigitating dendritic cell tumor (S100+, vimentin+, CD21-, CD35-), melanoma or other sarcomas.
Additional references: Lymph nodes-not lymphoma chapter, Case of the Week #1
References
1. Li CF, Chuang SS and Lin CN. A 70-year-old-man with multiple intra-abdominal masses and liver and spleen metastases. Archives of Pathology and Laboratory Medicine 2005; 129: e130-131. link
2. Chan JK, Fletcher CD, Nayler SJ and Cooper K. Fletcher CDM, Nayler S, Cooper K. Follicular dendritic cell sarcoma. Cancer 1997; 79: 294-313. link
3. Fonseca R, Yamakawa M, Nakamura S et al. Follicular dendritic cell sarcoma and interdigitating reticulum cell sarcoma: a review. American Journal of Hematology 1998; 59:161-67. link
4. Han JH, Se-Hoon K, Sung-Hun N, Yong-Chan L, Ho-Guen K, Woo-Ick Y. Follicular dendritic cell sarcoma presenting as a submucosal tumor of the stomach. Archives of Pathology and Laboratory Medicine 2000; 124: 1693-1696. link
5. Ioachim HL, Ratech H. Ioachims Lymph Node Pathology. Philadelphia: Lippincott Williams & Wilkins, 2002: 490-95.
6. Jaffe ES. Histiocytic and dendritic cell neoplasms. Follicular dentritic cell sarcoma / tumor. In: Jaffe ES, Harris NL, Stein H, Vardiman JW, eds. Pathology and Genetics of Tumours of the Haematopoietic and Lymphoid System. Lyon, France: IARC Press; 2001; 286-288. World Health Organization Classification of Tumours; volume 3.
7. Monda L, Warnke R, Rosai J. A primary lymph node malignancy with features suggestive of dendritic reticulum cell differentiation. A report of 4 cases. American Journal of Pathology 1986; 122: 562-72. link
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com