![]()
22 March 2007 – Case of the Week #78
These cases can also be accessed by clicking on the Case of the Week button on the left hand side of our Home Page at www.PathologyOutlines.com. This email is sent only to those who subscribe in writing or by email. To view the images or references, you must click on the links in blue.
To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also have a biweekly email of new Pathologist jobs added to our Jobs pages, a biweekly email of new Laboratory jobs added to our Jobs pages, a monthly email of website news, a monthly email of new books, and a twice a year newsletter by email or regular mail. You must subscribe or unsubscribe separately to these email lists.

This Case is sponsored by Milestone Medical, the technological leader in Microwave Accelerated Tissue Processing. Milestone manufactures instrumentation and accessories that enable Histologists and Pathologists to achieve the highest level of productivity, while maintaining their flexibility and safety. Milestone’s family of rapid microwave lab stations allow tissue samples to be processed in a fraction of the time as compared to conventional methods, allowing for same-day diagnosis. They also offer a line of digital imaging equipment for grossing stations and autopsy rooms. These systems serve as a comprehensive method of storing macroscopic images of all specimens examined in the laboratory, providing an invaluable diagnostic database for routine grossing, teaching, and research. For more information, please visit our website by clicking here.
We thank Drs. Ignat Schwartz and Eddie Fridman, The Chaim Sheba Medical Center, Ramat-Gan, Israel, for contributing this case. We invite you to contribute a Case of the Week by emailing NPernick@PathologyOutlines.com with microscopic images (any size, we will shrink if necessary) in JPG format, a clinical history, your diagnosis and any other images (gross, immunostains, EM, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you a check for $35 (US) for your time after we send out the case. Please only send cases with a definitive diagnosis.
Case of the Week #78
Clinical history
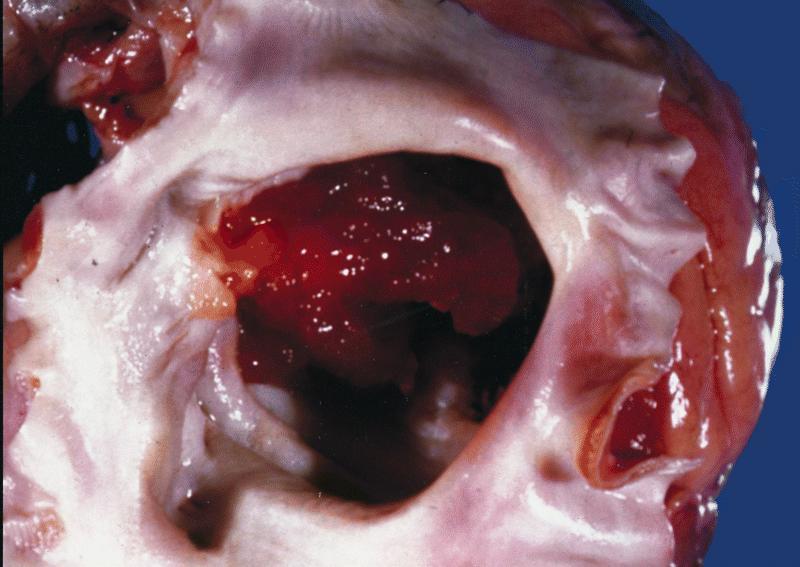
A previously healthy 65 year old woman had a left atrial mass approximately 30 cc in volume.
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
(scroll down to continue)
Diagnosis:
Cardiac myxoma with glandular differentiation
Discussion
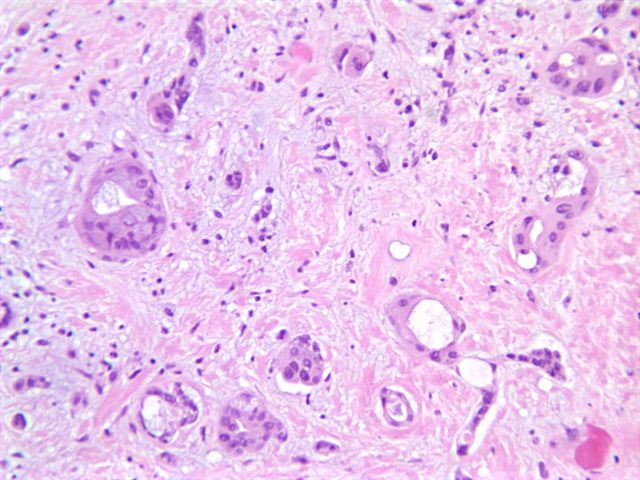
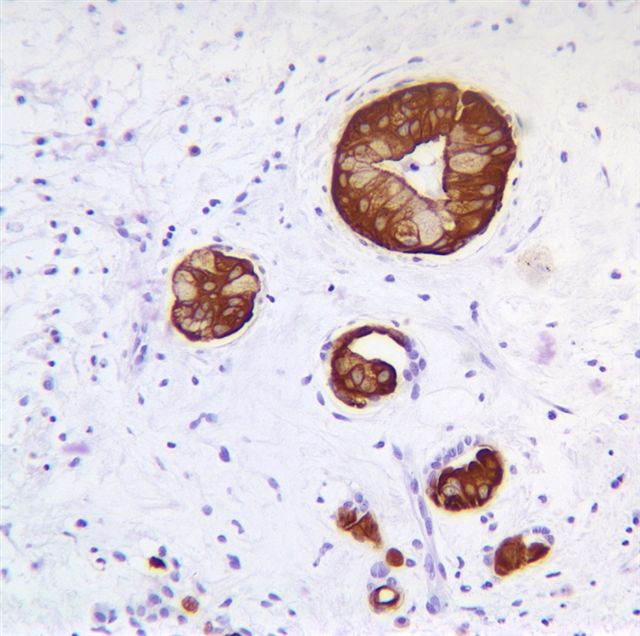
The tumor has a focal glandular component with bland columnar cells containing mucinous vacuoles. No cytologic atypia or mitotic activity is present. The stroma is hypocellular, edematous and myxoid, with occasional prominent blood vessels.
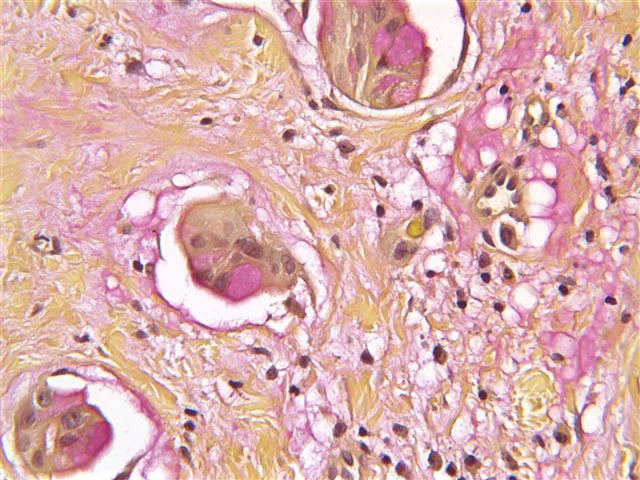
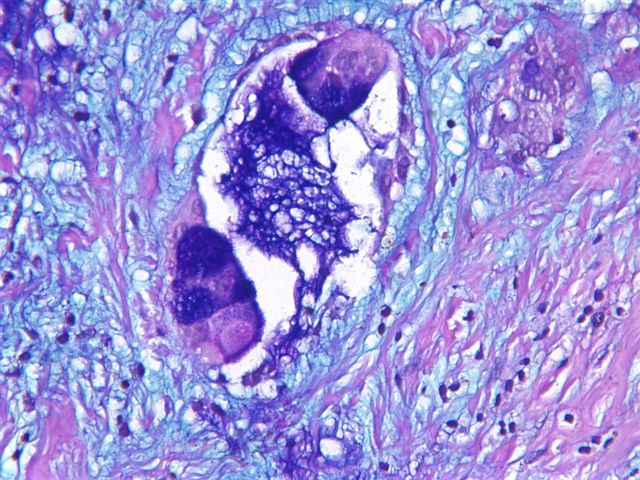
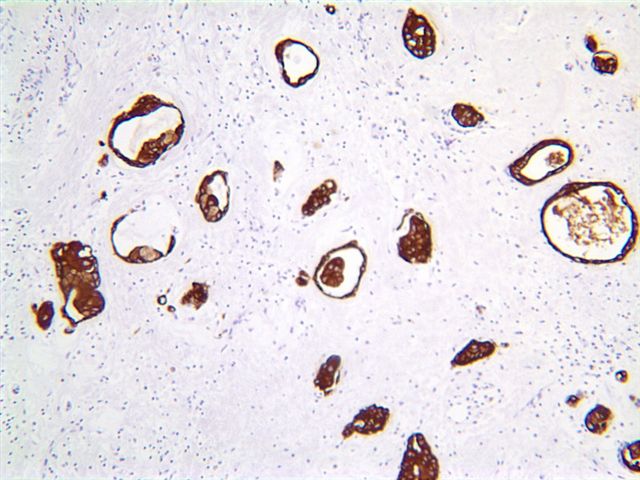
Routine stains performed included mucicarmine and Alcian blue (pH 2.5), which highlighted mucinous vacuoles. Immunostains performed included CK7 and MNF-116 (a broad spectrum cytokeratin), which strongly stained the glandular structures. Other positive markers were CAM 5.2, CEA, CA19.9, EMA and CD31. Negative markers included CA 15.3 and CU-18 / BCA-225 (breast cancer tumor markers), CK20, TTF1, chromogranin A, synaptophysin, thyroglobulin and S100.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Myxomas are the most common primary tumor of the heart, although they are still rare. They are distinct from soft tissue myxomas. The mean patient age is 50 years. Ninety percent occur in the atria, with 80% occurring on the left side. They often occur at the fossa ovalis, and may be up to 10 cm in dimension. Cases associated with Carney’s syndrome typically present at a mean age of 24 years (AJSP 1985;9:53).
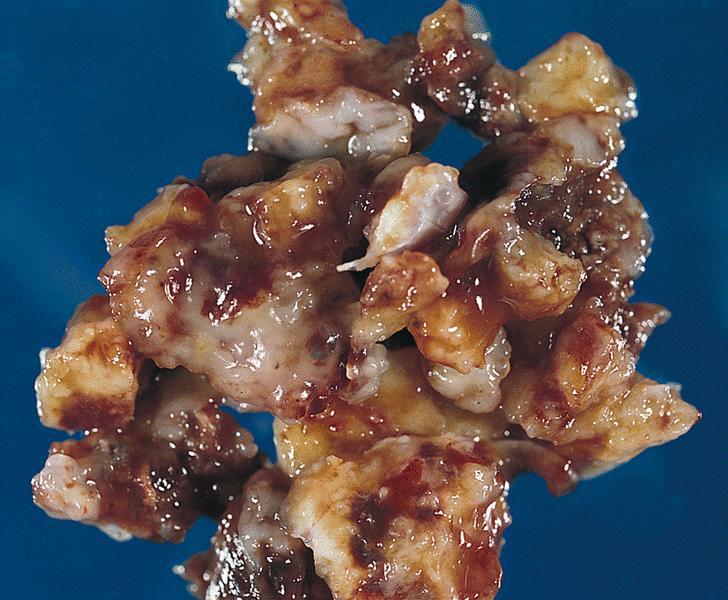
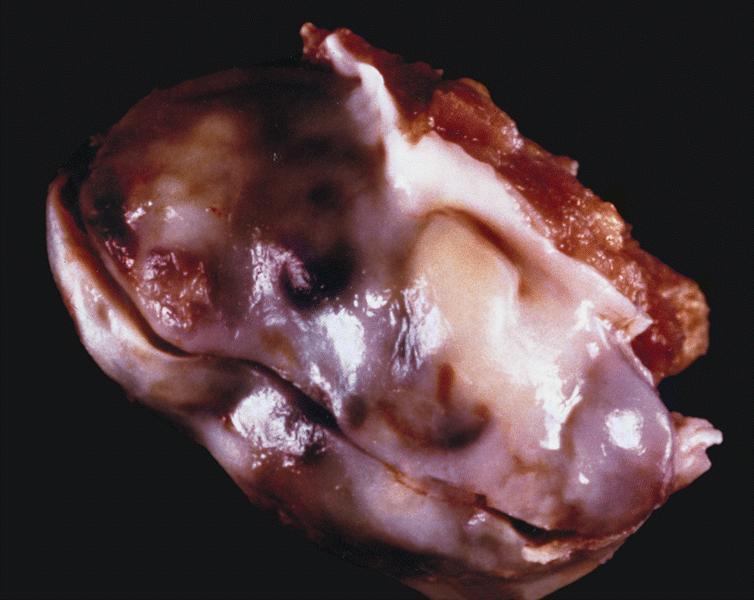
Myxomas often have a gelatinous surface. The margins may be irregular or smooth. Histologically, myxomas contain complex structures resembling rings or poorly formed glands, composed of stellate or globular (lepedic) cells with abundant eosinophilic cytoplasm and an indistinct cell border. The nuclei are oval with open chromatin and indistinct nuclei. There is a prominent myxoid stroma. Mitotic activity is variable, and often more prominent near the tumor surface.
{kind=link}
{kind=link}
{kind=link}
Tumor cells are immunoreactive for CD31, CD34 and calretinin (AJCP 2000;114:754). Glandular components may be keratin positive, as in this case.
The main differential diagnosis in this case is metastatic carcinoma. It typically has anaplastic tumor cells with prominent mitotic activity. Clinical history may also be helpful. Immunostains are often less helpful, as both tumors may be strongly keratin immunoreactive.
Myxomas are benign, but may cause death via embolization. Excision is curative in most cases, with only rare recurrence or metastases.
References: AJCP 1993;100:671, Tumors of the Heart and Great Vessels (AFIP Atlas of Tumor Pathology, Series 3, Vol 16); 1996
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com