
29 November 2006 - Case #65
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ronald M. Angeles, University of Pittsburgh, Pennsylvania, USA.
Case #65
Clinical history:
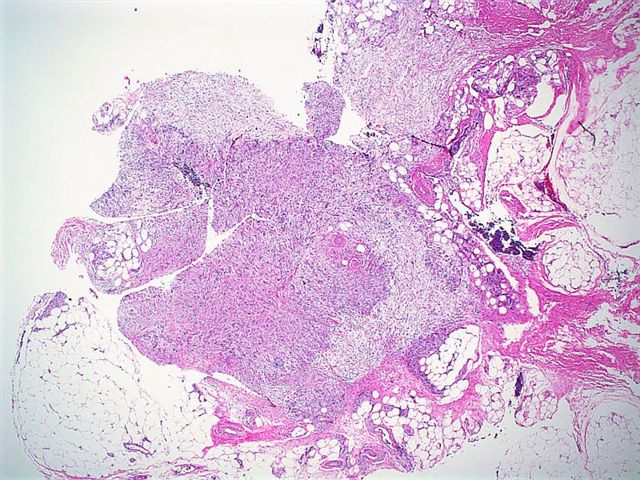
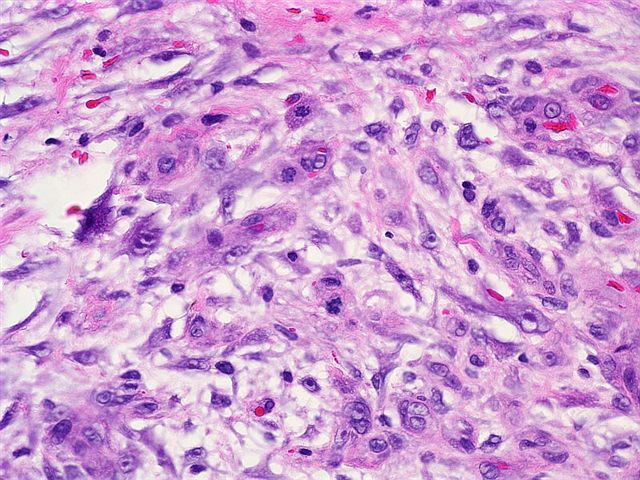
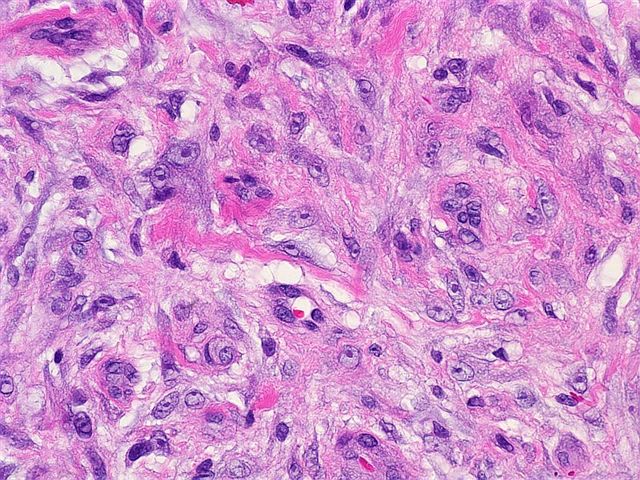
A 37 year old woman had a wrist mass that was clinically thought to be a lipoma. The spindle cells had diffuse cytoplasmic immunoreactivity for CD68 and calponin and were negative for S100 and pankeratin. CD34 highlighted the blood vessels.
Microscopic images:
What is your diagnosis?
Diagnosis: Nodular fasciitis of the wrist
Discussion:
Nodular fasciitis is a common lesion that typically presents with a history of a rapidly growing mass on the flexor forearm, chest or back. It can also develop within the bladder, breast, vulva, vagina, cervix or prostate (Hinyokika Kiyo 1994;40:427, Breast 2005;14:384, Int J Gynecol Pathol 1997;16:117). There is often a history of trauma. It is frequently misdiagnosed as sarcoma based on its cellularity, the presence of mitotic figures and its rapid growth.
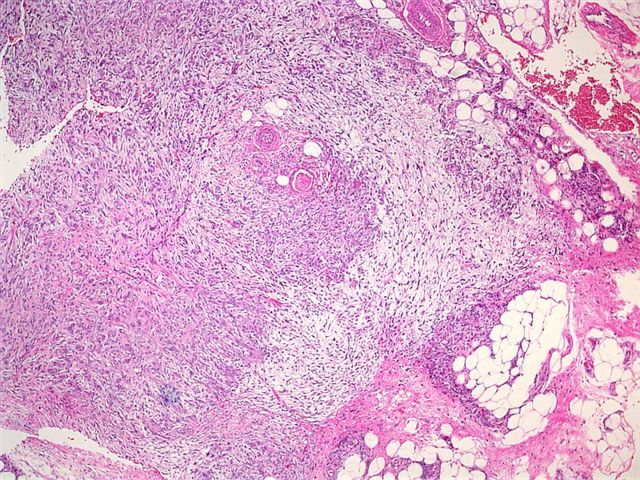
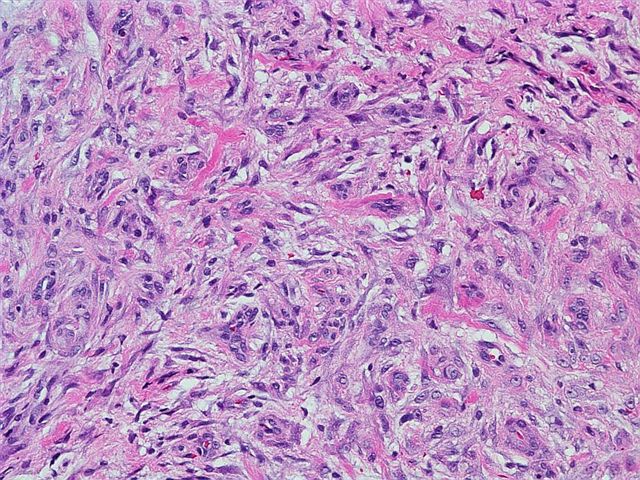
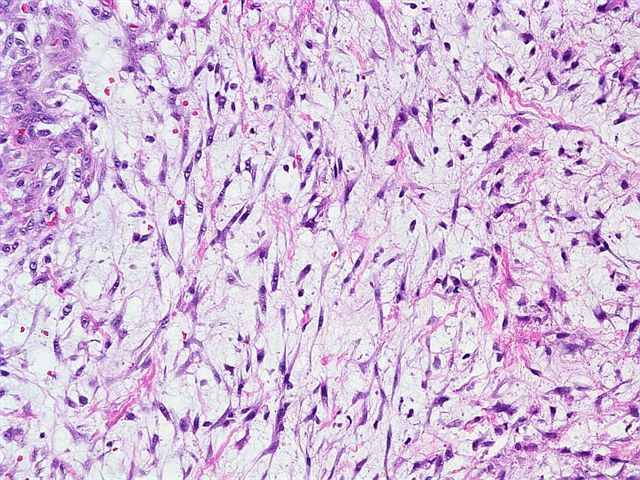
It typically is 2 cm or less in size and relatively well circumscribed. It is highly cellular and composed of plump, immature fibroblasts or myofibroblasts, with a feathery pattern due to the abundance of ground substance. The tumor cells usually have prominent nucleoli. There is often a myxoid stroma, frequent mitotic figures but no atypical forms, a lymphocytic infiltrate and red blood cell extravasation. The vasculature is usually prominent. There may be bands of collagen similar to keloid scars or metaplastic bone.
The fibroblasts and myofibroblasts are typically immunoreactive for smooth muscle actin, muscle specific actin and calponin (Am J Dermatopathol 2006;28:105). Macrophages are CD68+, as are some fibroblasts that have acquired phagocytic properties. Immunostains for S100, keratin and CD34 are typically negative (Am J Surg Pathol 1993;17:1039).
The differential diagnosis includes fibromatosis, fibrous histiocytoma and malignant fibrous histiocytoma (MFH). Fibromatosis is usually a large lesion that infiltrates surrounding soft tissue. Tumor cells are spindled and separated by abundant collagen. Fibrous histiocytoma is usually dermal based and has a storiform pattern. There are also prominent xanthoma cells and often Touton giant cells. Myxoid MFH has tumor cells with more pleomorphism and often has regular arborizing vessels. There are often atypical mitotic figures and areas of classic MFH.
Nodular fasciitis is a benign, reactive process and excision is almost always curative, even if the lesion is incompletely excised.
References: Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ronald M. Angeles, University of Pittsburgh, Pennsylvania, USA.
Website news:
(1) With the holiday season upon us, we recommend you consider purchasing gifts and books online at Amazon.com through the links on our Home Page (footer), on the Books page (click on any Book title) or by clicking here. Most Amazon.com shoppers have a good shopping experience. You can buy new or used products from various companies for competitive prices. There is free shipping for many products and they have a good return policy. In addition, purchases made through links on our website help us continue to expand our free website, without costing you anything and may even save you money through Amazon's discounts.
Visit and follow our Blog to see recent updates to the website.
(1) With the holiday season upon us, we recommend you consider purchasing gifts and books online at Amazon.com through the links on our Home Page (footer), on the Books page (click on any Book title) or by clicking here. Most Amazon.com shoppers have a good shopping experience. You can buy new or used products from various companies for competitive prices. There is free shipping for many products and they have a good return policy. In addition, purchases made through links on our website help us continue to expand our free website, without costing you anything and may even save you money through Amazon's discounts.
Visit and follow our Blog to see recent updates to the website.
Case #65
Clinical history:
A 37 year old woman had a wrist mass that was clinically thought to be a lipoma. The spindle cells had diffuse cytoplasmic immunoreactivity for CD68 and calponin and were negative for S100 and pankeratin. CD34 highlighted the blood vessels.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Nodular fasciitis of the wrist
Discussion:
Nodular fasciitis is a common lesion that typically presents with a history of a rapidly growing mass on the flexor forearm, chest or back. It can also develop within the bladder, breast, vulva, vagina, cervix or prostate (Hinyokika Kiyo 1994;40:427, Breast 2005;14:384, Int J Gynecol Pathol 1997;16:117). There is often a history of trauma. It is frequently misdiagnosed as sarcoma based on its cellularity, the presence of mitotic figures and its rapid growth.
It typically is 2 cm or less in size and relatively well circumscribed. It is highly cellular and composed of plump, immature fibroblasts or myofibroblasts, with a feathery pattern due to the abundance of ground substance. The tumor cells usually have prominent nucleoli. There is often a myxoid stroma, frequent mitotic figures but no atypical forms, a lymphocytic infiltrate and red blood cell extravasation. The vasculature is usually prominent. There may be bands of collagen similar to keloid scars or metaplastic bone.
The fibroblasts and myofibroblasts are typically immunoreactive for smooth muscle actin, muscle specific actin and calponin (Am J Dermatopathol 2006;28:105). Macrophages are CD68+, as are some fibroblasts that have acquired phagocytic properties. Immunostains for S100, keratin and CD34 are typically negative (Am J Surg Pathol 1993;17:1039).
The differential diagnosis includes fibromatosis, fibrous histiocytoma and malignant fibrous histiocytoma (MFH). Fibromatosis is usually a large lesion that infiltrates surrounding soft tissue. Tumor cells are spindled and separated by abundant collagen. Fibrous histiocytoma is usually dermal based and has a storiform pattern. There are also prominent xanthoma cells and often Touton giant cells. Myxoid MFH has tumor cells with more pleomorphism and often has regular arborizing vessels. There are often atypical mitotic figures and areas of classic MFH.
Nodular fasciitis is a benign, reactive process and excision is almost always curative, even if the lesion is incompletely excised.
References: Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
