
18 October 2006 - Case #62
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Juan Jose Segura Fonseca, Departamento de Patologia Hospital, San Juan de Dios, San Jose, Costa Rica.
Case #62
Clinical history:
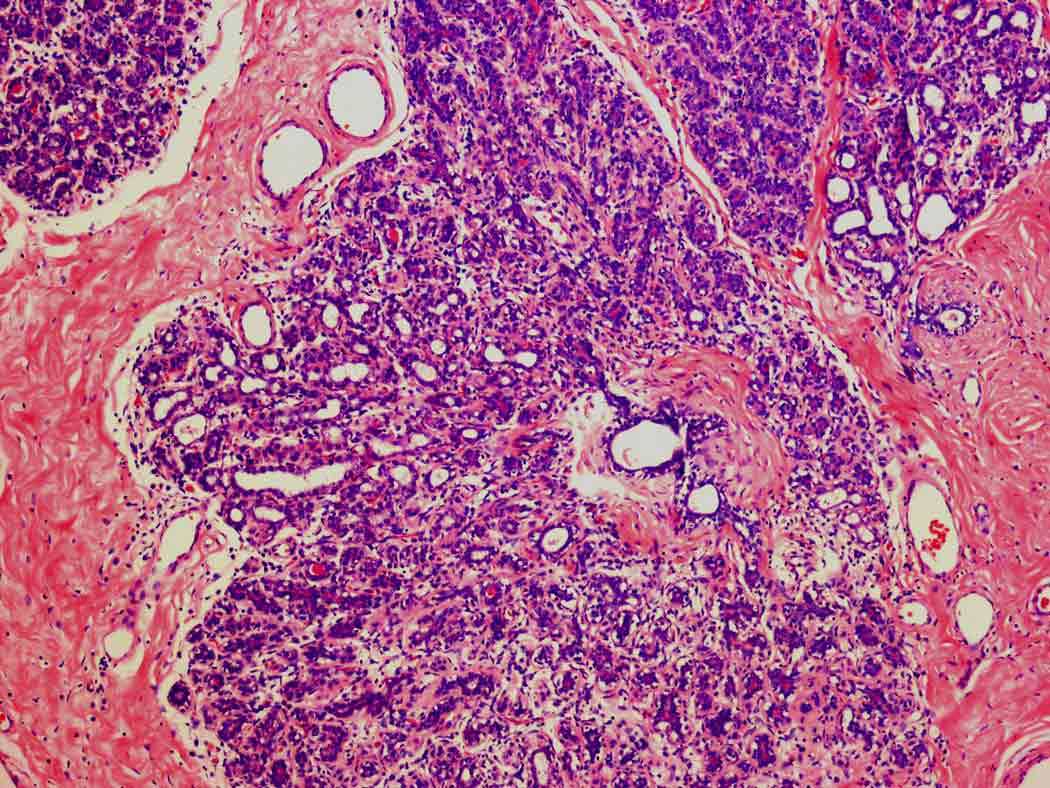
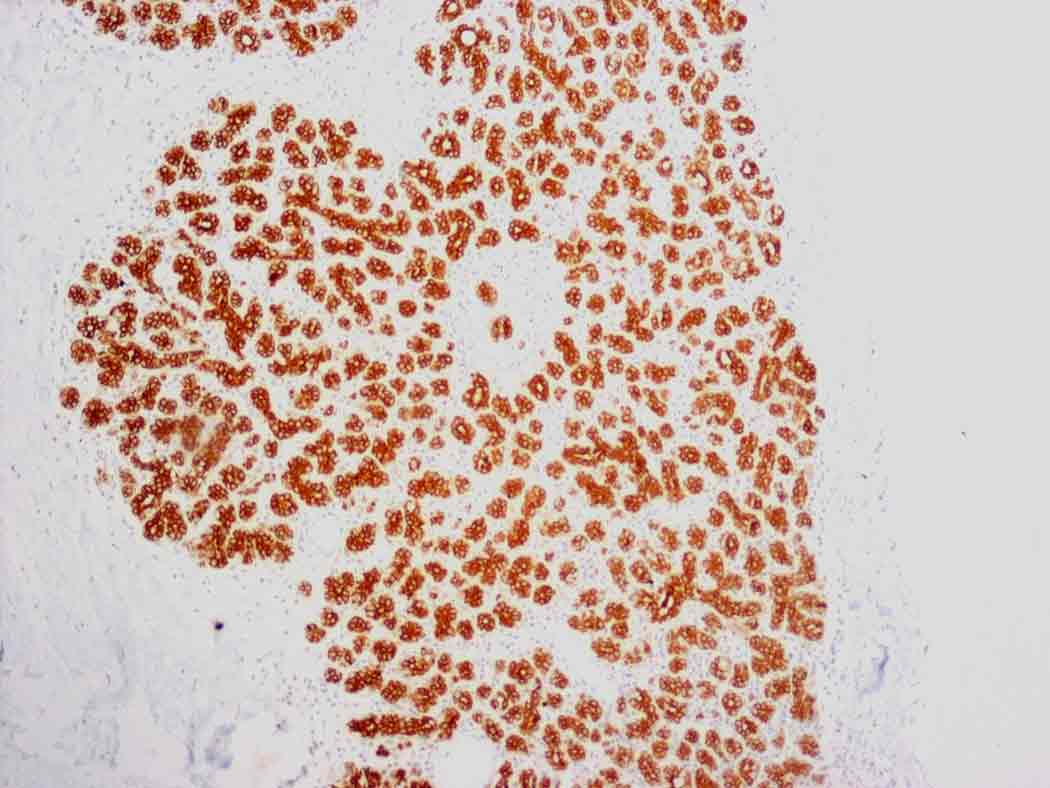
A 22 year old Caucasian woman had a 2 month history of an enlarging right breast mass. There was no nipple discharge and she denied use of hormones or other drugs. The mass was tender to palpation without any external signs of inflammation. The resected specimen was 540 grams, 14 x 11 x 4 cm, solid, ovoid and well circumscribed. The cut surface was white, firm and homogenous with a few scattered slit-like spaces (image 1, image 2). Low and medium power showed large hyperplastic lobules with a proliferation of ductules and acini. Few ducts were dilated (image 3, image 4, image 5). The enlarged lobules were strongly immunoreactive for cytokeratin 8 (image 6).
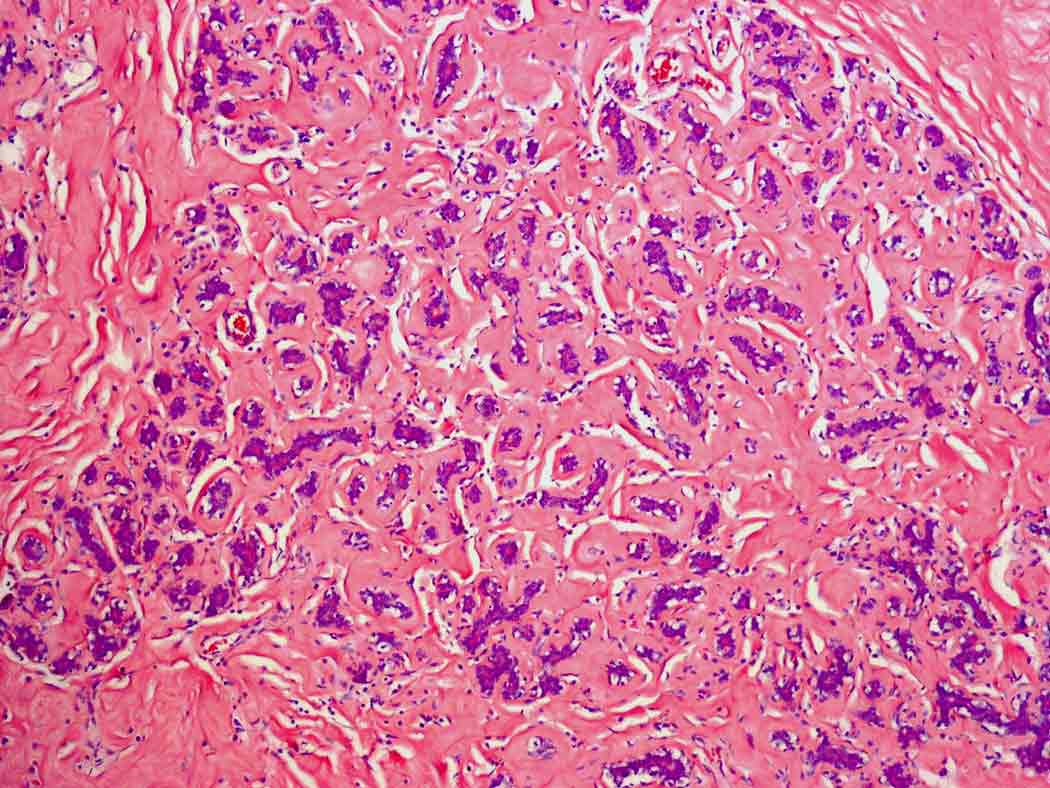
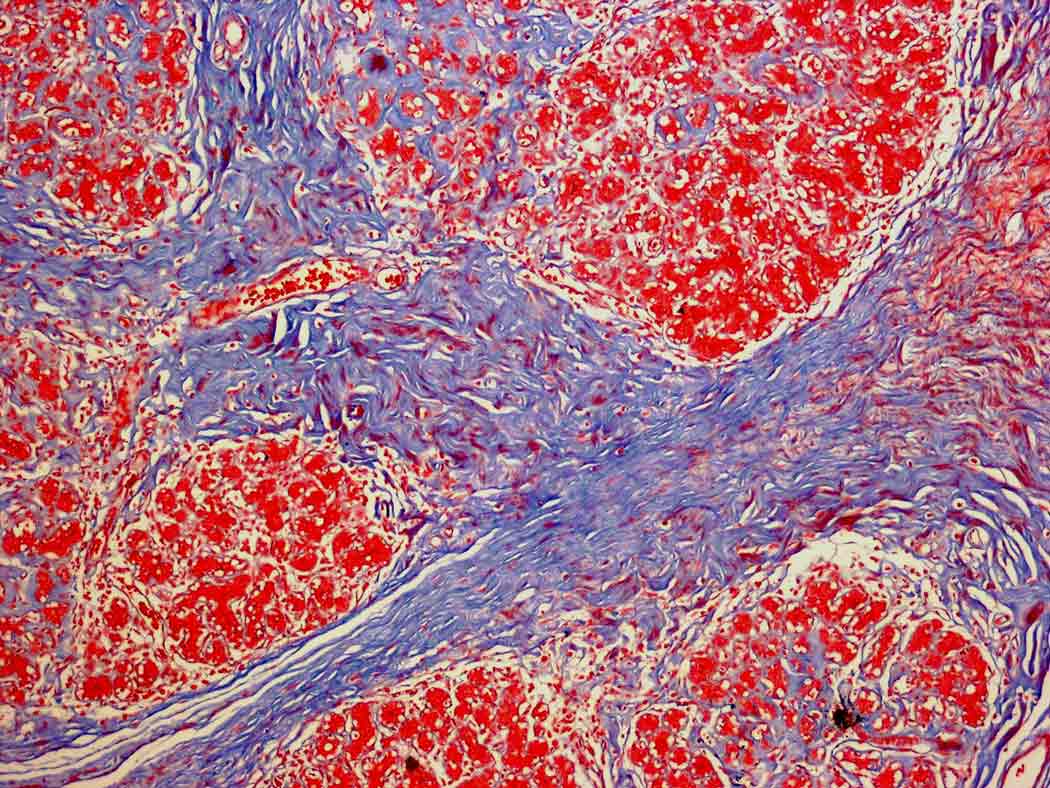
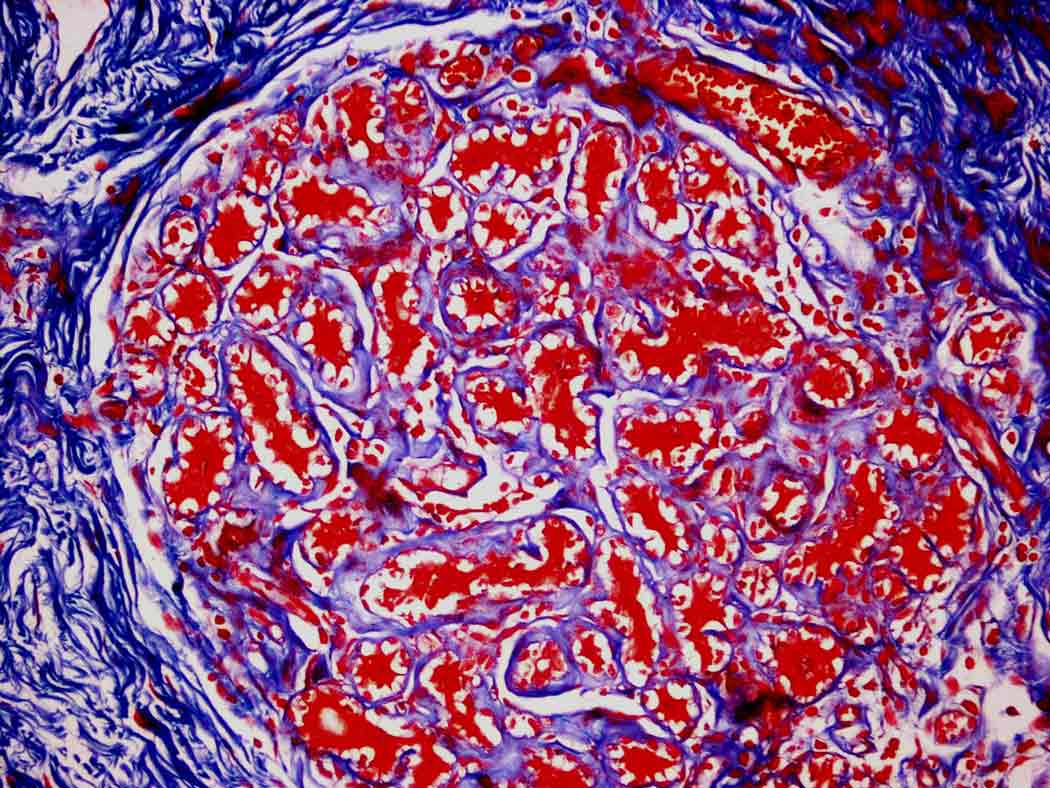
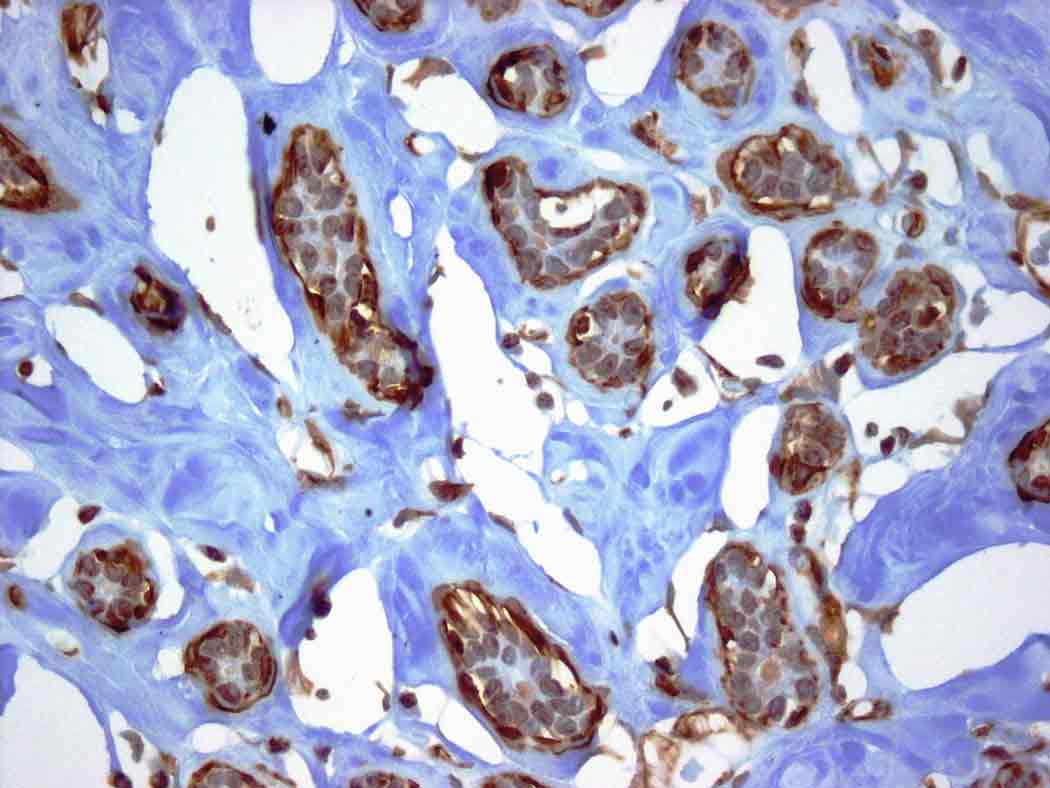
The sclerosis seemed to start at the center of the lobule and radiate towards the periphery, incarcerating the acini with severe fibrosis and atrophy (image 7, image 8). The trichrome stain highlighted dense interlobular fibrosis and a peculiar periacinar sclerosis with a glomeruloid pattern (image 9, image 10). The myoepithelial cells were prominent in these areas, as demonstrated by calponin immunoreactivity (image 11).
Gross images:


Microscopic images:



What is your diagnosis?
Diagnosis: Sclerosing lobular hyperplasia of the breast
Stain images:
Discussion:
Sclerosing lobular hyperplasia is an uncommon lesion of the female breast characterized by prominent hyperplasia of the lobules with severe and extensive fibrosis of the intralobular stroma and to a lesser degree, the interlobular parenchyma. It occurs almost exclusively in young women. Patients generally complain of a palpable, painless or slightly tender and well defined lump in the breast of short duration. This lesion was first reported by Kovi et al. who described it in a group of 18 patients, mainly young women (Hum Pathol 1984;15:336). It is possible that Cheatle in 1922 was referring to the same lesion (Br J Surg 1922;10:436). The mean age of patients is 28 to 32 years, with a range of 12 to 46 years (AJR Am Roentgenol 1995;165:291).
Its relation to fibroadenoma or fibroadenomatoid changes around the hyperplastic lobules was noted in the original article and some authors have redefined this lesion as fibroadenomatosis, fibroadenoid mastopathy or fibroadenomatoid hyperplasia (Hum Pathol 1984;15:336, Rosen: Rosen's Breast Pathology, 2nd Edition, 2001). In our case, this feature is not present.
The clinical differential diagnosis includes giant juvenile fibroadenoma and juvenile hypertrophy in younger patients and phyllodes tumor in older patients. None of these lesions have been associated with lobular sclerosis.
Pathologically, the resected specimens vary from small ovoid and white solid tumors of 1 cm up to large solid tumors. Fine needle aspiration findings are nonspecific and overlap with fibroadenoma, including flat sheets of oval ductal epithelial cells in an acinar arrangement, a few bare nuclei in a clean background and variable stromal fragments (CytoJournal 2006;3:8, Diagn Cytopathol 2004;31:340).
The natural course of sclerosing lobular hyperplasia is not known. However, no association with malignancy or recurrence has been documented.
References: Hum Pathol 1984;15:336, Br J Surg 1922;10:436, AJR Am Roentgenol 1995;165:291, Rosen: Rosen's Breast Pathology, 2nd Edition, 2001, CytoJournal 2006;3:8, Diagn Cytopathol 2004;31:340
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Juan Jose Segura Fonseca, Departamento de Patologia Hospital, San Juan de Dios, San Jose, Costa Rica.
Website news:
(1) We have transferred all of our files to our new, faster server. If you have any problems accessing pages in our website, please let us know.
(2) How can you find detailed pathology information in 15 seconds or less? Use our free online textbook. From the Home page at www.PathologyOutlines.com, click on the appropriate chapter, then on the topic in the Table of Contents and you will be directed to clinical information, gross and microscopic images, immunohistochemistry and other stain results, references and other pertinent information. This is a good way to quickly refresh your memory on any entity you have not seen in a while.
Visit and follow our Blog to see recent updates to the website.
(1) We have transferred all of our files to our new, faster server. If you have any problems accessing pages in our website, please let us know.
(2) How can you find detailed pathology information in 15 seconds or less? Use our free online textbook. From the Home page at www.PathologyOutlines.com, click on the appropriate chapter, then on the topic in the Table of Contents and you will be directed to clinical information, gross and microscopic images, immunohistochemistry and other stain results, references and other pertinent information. This is a good way to quickly refresh your memory on any entity you have not seen in a while.
Visit and follow our Blog to see recent updates to the website.
Case #62
Clinical history:
A 22 year old Caucasian woman had a 2 month history of an enlarging right breast mass. There was no nipple discharge and she denied use of hormones or other drugs. The mass was tender to palpation without any external signs of inflammation. The resected specimen was 540 grams, 14 x 11 x 4 cm, solid, ovoid and well circumscribed. The cut surface was white, firm and homogenous with a few scattered slit-like spaces (image 1, image 2). Low and medium power showed large hyperplastic lobules with a proliferation of ductules and acini. Few ducts were dilated (image 3, image 4, image 5). The enlarged lobules were strongly immunoreactive for cytokeratin 8 (image 6).
The sclerosis seemed to start at the center of the lobule and radiate towards the periphery, incarcerating the acini with severe fibrosis and atrophy (image 7, image 8). The trichrome stain highlighted dense interlobular fibrosis and a peculiar periacinar sclerosis with a glomeruloid pattern (image 9, image 10). The myoepithelial cells were prominent in these areas, as demonstrated by calponin immunoreactivity (image 11).
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Sclerosing lobular hyperplasia of the breast
Stain images:
Cytokeratin 8
Trichrome
Calponin
Discussion:
Sclerosing lobular hyperplasia is an uncommon lesion of the female breast characterized by prominent hyperplasia of the lobules with severe and extensive fibrosis of the intralobular stroma and to a lesser degree, the interlobular parenchyma. It occurs almost exclusively in young women. Patients generally complain of a palpable, painless or slightly tender and well defined lump in the breast of short duration. This lesion was first reported by Kovi et al. who described it in a group of 18 patients, mainly young women (Hum Pathol 1984;15:336). It is possible that Cheatle in 1922 was referring to the same lesion (Br J Surg 1922;10:436). The mean age of patients is 28 to 32 years, with a range of 12 to 46 years (AJR Am Roentgenol 1995;165:291).
Its relation to fibroadenoma or fibroadenomatoid changes around the hyperplastic lobules was noted in the original article and some authors have redefined this lesion as fibroadenomatosis, fibroadenoid mastopathy or fibroadenomatoid hyperplasia (Hum Pathol 1984;15:336, Rosen: Rosen's Breast Pathology, 2nd Edition, 2001). In our case, this feature is not present.
The clinical differential diagnosis includes giant juvenile fibroadenoma and juvenile hypertrophy in younger patients and phyllodes tumor in older patients. None of these lesions have been associated with lobular sclerosis.
Pathologically, the resected specimens vary from small ovoid and white solid tumors of 1 cm up to large solid tumors. Fine needle aspiration findings are nonspecific and overlap with fibroadenoma, including flat sheets of oval ductal epithelial cells in an acinar arrangement, a few bare nuclei in a clean background and variable stromal fragments (CytoJournal 2006;3:8, Diagn Cytopathol 2004;31:340).
The natural course of sclerosing lobular hyperplasia is not known. However, no association with malignancy or recurrence has been documented.
References: Hum Pathol 1984;15:336, Br J Surg 1922;10:436, AJR Am Roentgenol 1995;165:291, Rosen: Rosen's Breast Pathology, 2nd Edition, 2001, CytoJournal 2006;3:8, Diagn Cytopathol 2004;31:340
