![]()
13 September 2006 Case of the Week #59
These cases can also be accessed by clicking on the Case of the Week button on the left hand side of our Home Page at www.PathologyOutlines.com. This email is sent only to those who subscribe in writing or by email. To view the images or references, you must click on the links in blue.
To subscribe or unsubscribe, email info@PathologyOutlines.com, indicating subscribe or unsubscribe to Case of the Week. We do not sell, share or use your email address for any other purpose. We also maintain two other email lists: to receive a biweekly update of new jobs added to our Jobs pages, and to receive a monthly update of changes made to the website. You must subscribe or unsubscribe separately to these email lists.
Check out our new Amazon.com link on the left side of the Home Page. If you buy online, we suggest you check out Amazons wide line of new and used goods that they either sell directly or through other companies, with varying prices and ever changing discounts. All purchases made through this link or through the Books pages help our website, without costing you anything.
We have split our Colon chapter into Colon-nontumor and Colon-tumor, and thoroughly updated the Colon-nontumor chapter. It now has more extensive text and over 600 image links and 500 references. The Colon-tumor chapter will be updated next. Since it takes only 15 seconds to look up information, many pathologists use these chapters to refresh their memory about a known entity, or to educate themselves about entities they rarely see.
We thank Dr. Jamie Shutter, George Washington University, Washington D.C. (USA) for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
The next case (Case #60) will be sent on September 27, 2006, as we will be at the IAP in Montreal next week.
Case of the Week #59
Clinical history
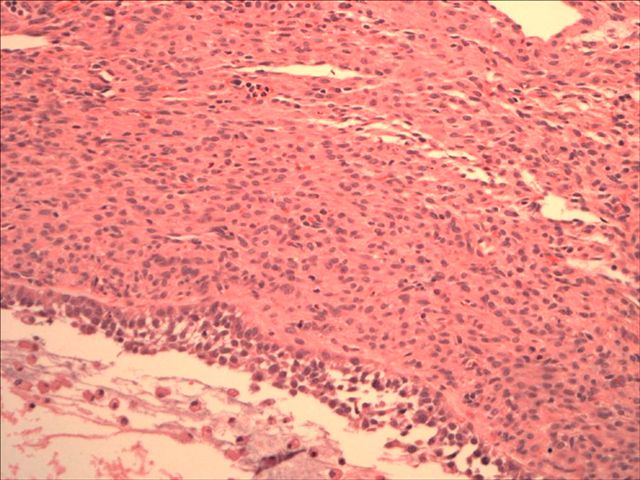
A seven year old girl presented with precocious puberty. Pelvic ultrasound revealed a left ovarian mass.
Microscopic images: image #1; #2; #3
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
(scroll down to continue)
Diagnosis:
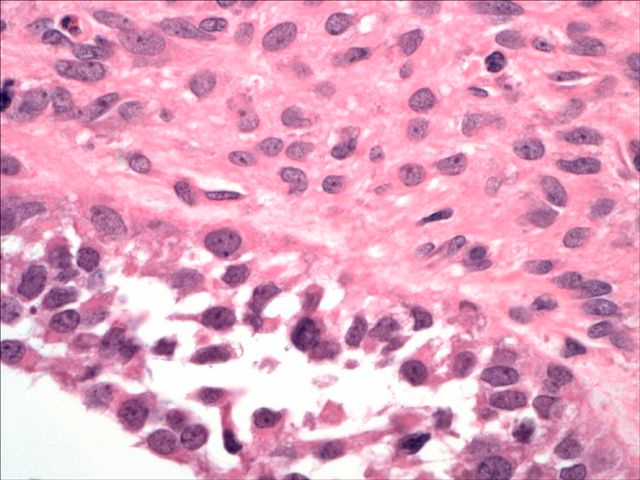
Juvenile granulosa cell tumor
Discussion
This tumor is composed of macrofollicles with eosinophilic secretions, and intervening tumor cells with abundant eosinophilic cytoplasm, round/oval hyperchromatic nuclei with small nucleoli, and mildly irregular nuclear contours. There are rare nuclear grooves. Other features often present include high mitotic activity, nuclear atypia and occasionally hobnail-like cells.
Grossly, these tumors are partially solid and cystic. Hemorrhage or necrosis may be present.
Juvenile granulosa cell tumors comprise only 5% of ovarian tumors of childhood or adolescence. Typically, they present as sexual precocity in prepubertal girls due to excessive estrogen production, although androgens may rarely be produced (J Endocrinol Invest 2006;29:653). Rarely, they are associated with an abnormal karyotype and ambiguous genitalia (AJSP 1985;9:737). Older patients may present with nonspecific abdominal swelling and pain.
Positive immunostains include inhibin and calretinin. They are not usually needed for diagnosis, but may be helpful in excluding germ cell tumors or melanoma.
The differential diagnosis includes adult granulosa cell tumors, thecoma and occasionally clear cell carcinoma. Adult granulosa cell tumors have more regularly shaped follicles that contain basement membrane material. Tumor cells have prominent nuclear grooves and less hyperchromasia.
Thecomas almost never occur in patients 30 years or younger, and usually lack mitotic activity. They also lack follicles, which are usually found in juvenile granulosa cell tumors with thorough sampling.
Finally, although hobnail-type cells may be seen in juvenile granulosa cell tumors, they are typically focal. In addition, patients with clear cell carcinoma are typically older, and their tumors lack follicles or areas of typical juvenile granulosa type cells.
Excision is usually adequate therapy for limited disease, although late recurrence may occur (Am J Obstet Gynecol 2004;191:366)
Additional references: Am J Surg Pathol 1984;8:575
Nat Pernick, M.D.
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Fax: 248/646-1736
Email: NPernick@PathologyOutlines.com