
6 September 2006 - Case #58
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California, USA.
Case #58
Clinical history:
The patient is a term newborn with abnormal fetal ultrasound and MRI, leading to a lobectomy after birth.
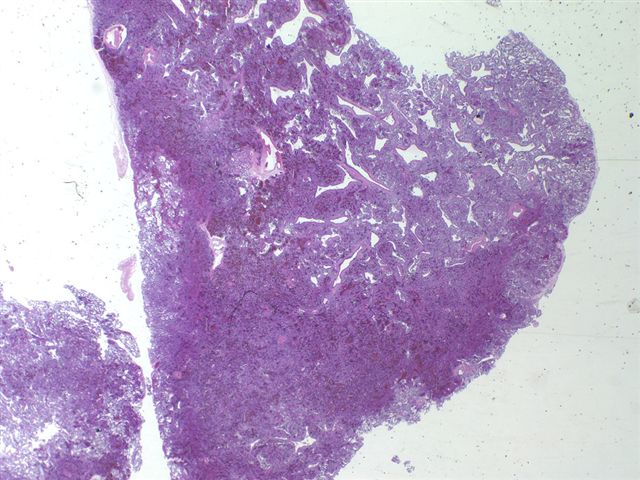
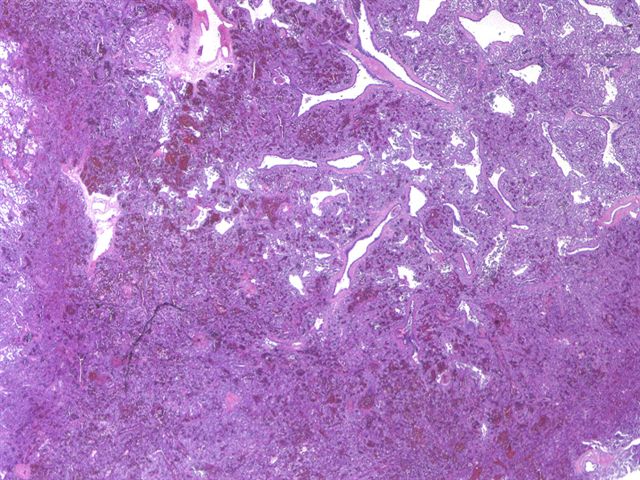
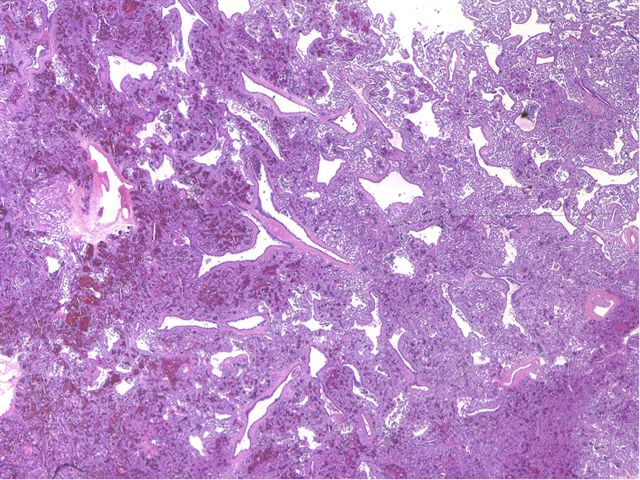
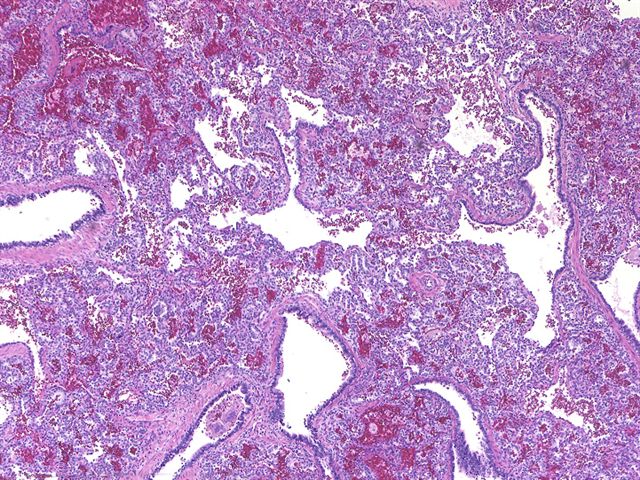
Microscopic images:

What is your diagnosis?
Diagnosis: Congenital cystic adenomatoid malformation, type II
Discussion:
Congenital cystic adenomatoid malformation is a rare hamartomatous disorder, affecting 1 per 25,000 births. It is characterized by variably sized cysts lined by columnar type (adenomatoid) epithelium. It may represent a maturation defect and is associated with neonatal distress, other lung conditions or stillbirth.
The current classification includes 5 types, discussed in more detail in the Lung chapter of PathologyOutlines.com. The present case contains small cysts up to 2 cm. On high power, these resemble dilated bronchioles lined by ciliated epithelium that are separated by normal alveoli. This type is associated with other malformations, not present in this case and a poor prognosis.
These entities appear to be developmental, not neoplastic. A recent study showed no karyotypic abnormalities and no p53 mutations (Pediatr Dev Pathol 2006;9:190).
Since some of these lesions regress spontaneously, current recommended treatment in asymptomatic infants is close follow up, with elective surgery for persistent lesions within the first year of life (Arch Dis Child Fetal Neonatal Ed 2006;91:F26, Int J Gynaecol Obstet 2005;89:99).
References: Arch Pathol Lab Med 2002;126:934, Am J Surg Pathol 2003;27:1139
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California, USA.
Case #58
Clinical history:
The patient is a term newborn with abnormal fetal ultrasound and MRI, leading to a lobectomy after birth.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Congenital cystic adenomatoid malformation, type II
Discussion:
Congenital cystic adenomatoid malformation is a rare hamartomatous disorder, affecting 1 per 25,000 births. It is characterized by variably sized cysts lined by columnar type (adenomatoid) epithelium. It may represent a maturation defect and is associated with neonatal distress, other lung conditions or stillbirth.
The current classification includes 5 types, discussed in more detail in the Lung chapter of PathologyOutlines.com. The present case contains small cysts up to 2 cm. On high power, these resemble dilated bronchioles lined by ciliated epithelium that are separated by normal alveoli. This type is associated with other malformations, not present in this case and a poor prognosis.
These entities appear to be developmental, not neoplastic. A recent study showed no karyotypic abnormalities and no p53 mutations (Pediatr Dev Pathol 2006;9:190).
Since some of these lesions regress spontaneously, current recommended treatment in asymptomatic infants is close follow up, with elective surgery for persistent lesions within the first year of life (Arch Dis Child Fetal Neonatal Ed 2006;91:F26, Int J Gynaecol Obstet 2005;89:99).
References: Arch Pathol Lab Med 2002;126:934, Am J Surg Pathol 2003;27:1139
