
23 August 2006 - Case #57
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California, USA.
Case #57
Clinical history:
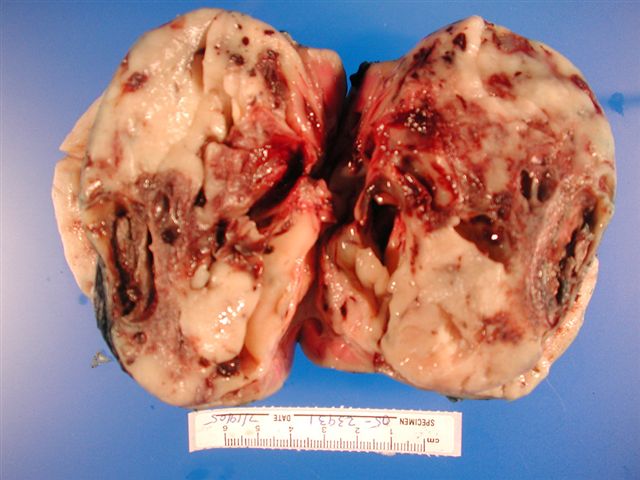
The patient is a 3 month old girl with a right kidney mass who underwent nephrectomy.
Gross images:
Microscopic images:

What is your diagnosis?
Diagnosis: Congenital mesoblastic nephroma, cellular type
Discussion:
Congenital mesoblastic nephroma, first described in 1967, is the most common kidney tumor of infancy (Pediatrics 1967;40:272).
There are 3 types of congenital mesoblastic nephroma, with slightly different clinical presentation. The classic type (24% of cases) presents at an average age of 2 - 3 weeks of life with a mean size of 100 g (Hum Pathol 1989;20:682). The cellular type (66% of cases), presents at 5 months of life and may weigh up to 1 kg. The mixed type (10%) of cases, has intermediate features. As most tumors present in infants, this diagnosis should be questioned if applied to patients over 2 years old (Murphy: Tumors of the Kidney, Bladder and Related Urinary Structures, 4th Edition, 2004).
Grossly, most congenital mesoblastic nephromas involve the renal sinus and it is important to report involvement of the medial resection margin by tumor. The classic type resembles leiomyoma with a whorled cut surface but also tongues of infiltrating tumor. The cellular type often has large cystic areas, hemorrhage and necrosis.
Microscopically, the classic type resembles infantile fibromatosis, with intersecting fascicles of bland spindle cells resembling myofibroblasts and interspersed thin collagen fibers. The cellular type resembles infantile fibrosarcoma. It has densely packed, plump atypical spindle cells with abundant cytoplasm, vesicular nuclei and nucleoli and often frequent mitotic figures.
Tumor cells in both types are immunoreactive for smooth muscle actin, desmin and vimentin and negative for keratin, except for entrapped epithelium.
The cellular type is often associated with t(12;15)(p13;q25), causing a ETV6::NTRK3 fusion gene, also seen in infantile fibrosarcoma involving infant soft tissues. The classic type lacks this translocation (Histopathology 2006;48:748).
Treatment consists of nephrectomy with wide margins. Chemotherapy is given for incomplete resection or tumor rupture during surgery. The cellular tumors may recur or rarely metastasize.
The differential diagnosis includes other tumors of infancy. Wilms tumor is common but typically involves older children. It has prominent blastema and often nephrogenic rests, although previous treated tumors may have a well differentiated spindle cell stroma. Clear cell sarcoma presents at a similar age but has a prominent chicken wire vasculature and clear cells. The tumor cells have fine nuclear chromatin and a low mitotic rate, compared to the coarse chromatin and higher mitotic rate of congenital mesoblastic nephroma. Clear cell sarcoma is negative for smooth muscle markers.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ankur Sangoi, Stanford University, Stanford, California, USA.
Case #57
Clinical history:
The patient is a 3 month old girl with a right kidney mass who underwent nephrectomy.
Gross images:
Microscopic images:
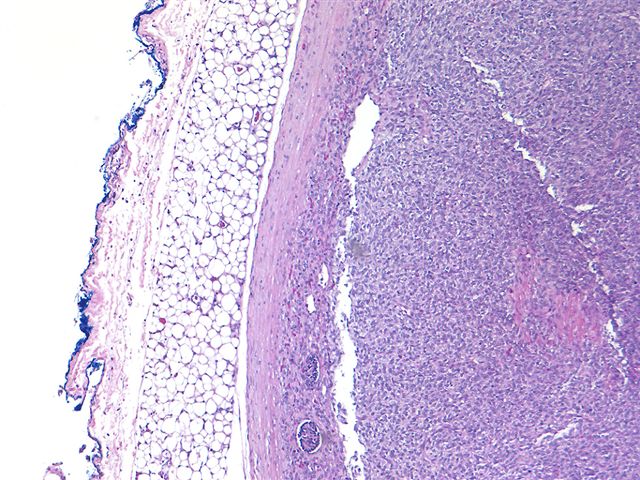
Well circumscribed
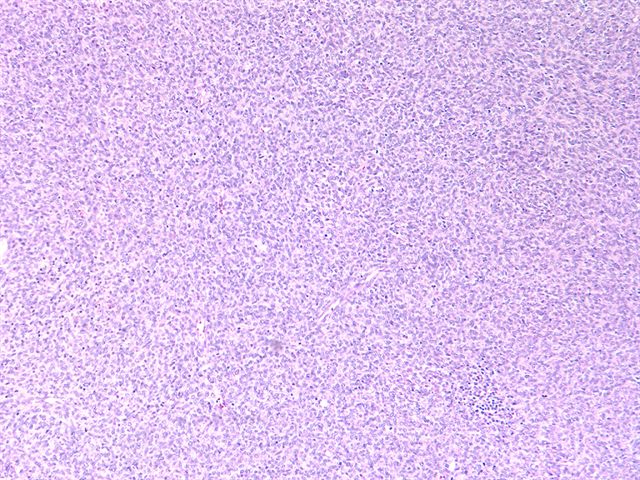
Medium power
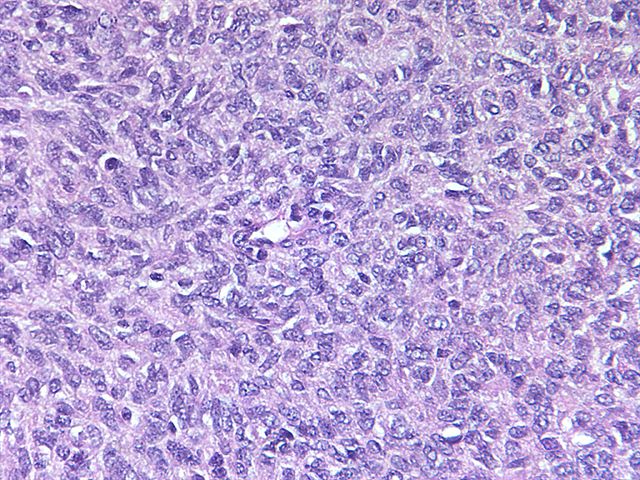
High power
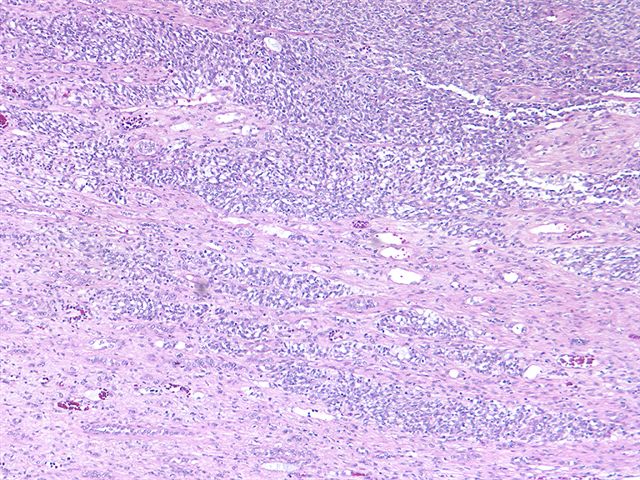
Infiltrative margin
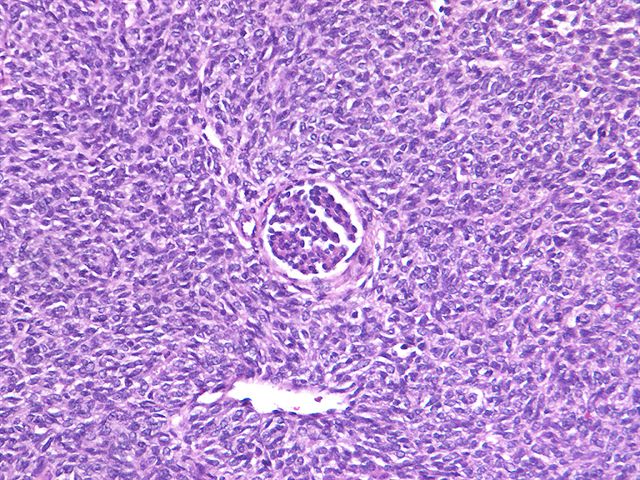
Glomerular entrapment
Angiomatoid area
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Congenital mesoblastic nephroma, cellular type
Discussion:
Congenital mesoblastic nephroma, first described in 1967, is the most common kidney tumor of infancy (Pediatrics 1967;40:272).
There are 3 types of congenital mesoblastic nephroma, with slightly different clinical presentation. The classic type (24% of cases) presents at an average age of 2 - 3 weeks of life with a mean size of 100 g (Hum Pathol 1989;20:682). The cellular type (66% of cases), presents at 5 months of life and may weigh up to 1 kg. The mixed type (10%) of cases, has intermediate features. As most tumors present in infants, this diagnosis should be questioned if applied to patients over 2 years old (Murphy: Tumors of the Kidney, Bladder and Related Urinary Structures, 4th Edition, 2004).
Grossly, most congenital mesoblastic nephromas involve the renal sinus and it is important to report involvement of the medial resection margin by tumor. The classic type resembles leiomyoma with a whorled cut surface but also tongues of infiltrating tumor. The cellular type often has large cystic areas, hemorrhage and necrosis.
Microscopically, the classic type resembles infantile fibromatosis, with intersecting fascicles of bland spindle cells resembling myofibroblasts and interspersed thin collagen fibers. The cellular type resembles infantile fibrosarcoma. It has densely packed, plump atypical spindle cells with abundant cytoplasm, vesicular nuclei and nucleoli and often frequent mitotic figures.
Tumor cells in both types are immunoreactive for smooth muscle actin, desmin and vimentin and negative for keratin, except for entrapped epithelium.
The cellular type is often associated with t(12;15)(p13;q25), causing a ETV6::NTRK3 fusion gene, also seen in infantile fibrosarcoma involving infant soft tissues. The classic type lacks this translocation (Histopathology 2006;48:748).
Treatment consists of nephrectomy with wide margins. Chemotherapy is given for incomplete resection or tumor rupture during surgery. The cellular tumors may recur or rarely metastasize.
The differential diagnosis includes other tumors of infancy. Wilms tumor is common but typically involves older children. It has prominent blastema and often nephrogenic rests, although previous treated tumors may have a well differentiated spindle cell stroma. Clear cell sarcoma presents at a similar age but has a prominent chicken wire vasculature and clear cells. The tumor cells have fine nuclear chromatin and a low mitotic rate, compared to the coarse chromatin and higher mitotic rate of congenital mesoblastic nephroma. Clear cell sarcoma is negative for smooth muscle markers.
