
9 August 2006 - Case #55
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Jamie Shutter, George Washington University Medical Center, Washington, D.C., USA. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case #55
Clinical history:
The patient is an asymptomatic 50 year old woman with a radiographic submucosal mass at the ileocecal junction suspicious for carcinoma. An ileocolectomy was performed.
Microscopic images:
What is your diagnosis?
Diagnosis: Endometriosis
Discussion:
Endometriosis may present clinically with pain or obstruction, as a mass lesion or be an incidental finding. In the bowel, it is rarely associated with neoplasms or premalignant change (Am J Surg Pathol 2000;24:513, Hum Pathol 2000;31:456, Am J Clin Pathol 1982;78:555).
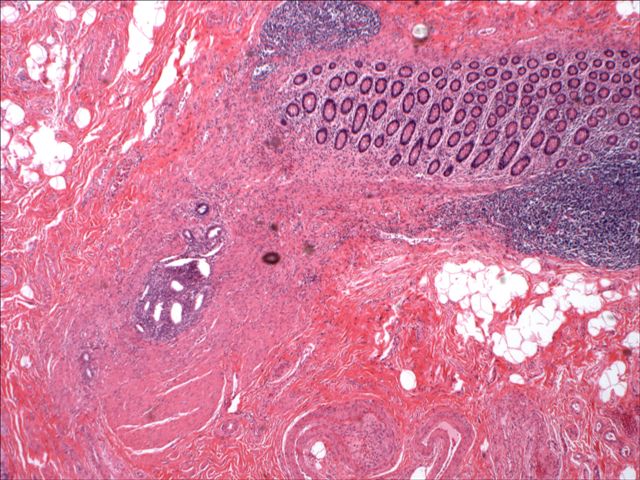
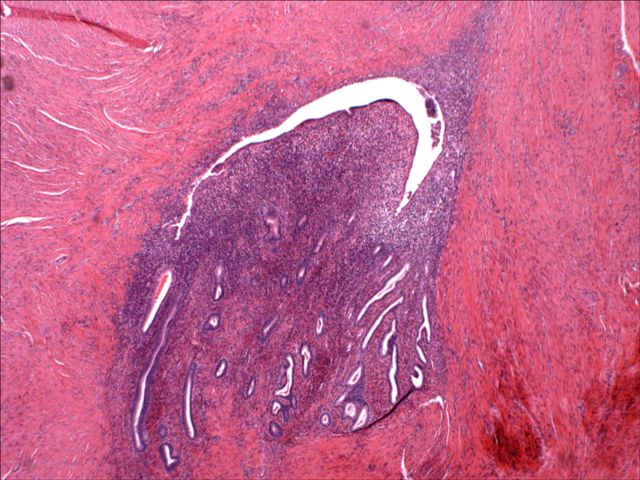
Grossly, endometriosis typically presents as serosal or subserosal nodules 5 cm or less in size. The cut surface is gray with small areas of hemorrhage. Microscopically, there are typical endometrial glands and stroma with hemosiderin in deeper layers. The lesion is often surrounded by smooth muscle. The overlying bowel epithelium may have inflammation and ulcers simulating inflammatory bowel disease or solitary rectal ulcer syndrome, but is otherwise normal. There may also be fibrosis of the bowel wall or neuronal hypertrophy.
The clinical differential diagnoses included diverticulitis, appendicitis, inflammatory bowel disease, irritable bowel syndrome, tubo-ovarian abscess and malignancy (Am J Surg Pathol 2001;25:445). The histologic diagnosis is usually not difficult as long as one thinks of the diagnosis. If necessary, the endometrial stroma tests immunoreactive for CD10 and the endometrial glands are negative for CEA.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Jamie Shutter, George Washington University Medical Center, Washington, D.C., USA. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Website news:
(1) Are you planning on buying any new pathology books? Check out our Books page. We list over 700 books of interest to pathologists sorted by subspecialty (liver pathology, cytopathology, etc.), book series, publisher and date posted.
Visit and follow our Blog to see recent updates to the website.
(1) Are you planning on buying any new pathology books? Check out our Books page. We list over 700 books of interest to pathologists sorted by subspecialty (liver pathology, cytopathology, etc.), book series, publisher and date posted.
Visit and follow our Blog to see recent updates to the website.
Case #55
Clinical history:
The patient is an asymptomatic 50 year old woman with a radiographic submucosal mass at the ileocecal junction suspicious for carcinoma. An ileocolectomy was performed.
Microscopic images:
Low power
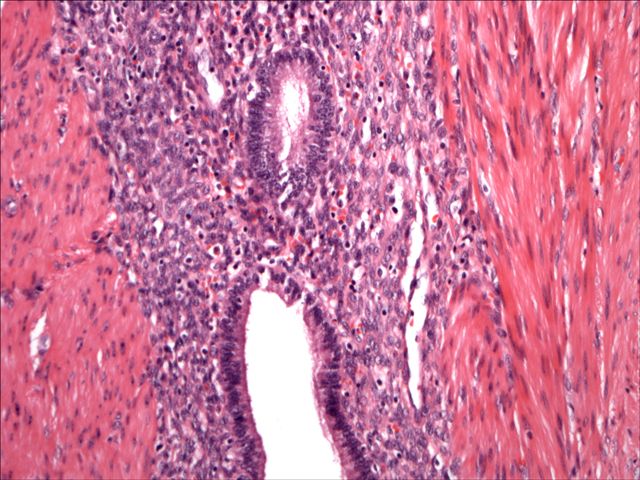
Medium power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Endometriosis
Discussion:
Endometriosis may present clinically with pain or obstruction, as a mass lesion or be an incidental finding. In the bowel, it is rarely associated with neoplasms or premalignant change (Am J Surg Pathol 2000;24:513, Hum Pathol 2000;31:456, Am J Clin Pathol 1982;78:555).
Grossly, endometriosis typically presents as serosal or subserosal nodules 5 cm or less in size. The cut surface is gray with small areas of hemorrhage. Microscopically, there are typical endometrial glands and stroma with hemosiderin in deeper layers. The lesion is often surrounded by smooth muscle. The overlying bowel epithelium may have inflammation and ulcers simulating inflammatory bowel disease or solitary rectal ulcer syndrome, but is otherwise normal. There may also be fibrosis of the bowel wall or neuronal hypertrophy.
The clinical differential diagnoses included diverticulitis, appendicitis, inflammatory bowel disease, irritable bowel syndrome, tubo-ovarian abscess and malignancy (Am J Surg Pathol 2001;25:445). The histologic diagnosis is usually not difficult as long as one thinks of the diagnosis. If necessary, the endometrial stroma tests immunoreactive for CD10 and the endometrial glands are negative for CEA.
