
5 July 2006 - Case #52
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Sungmi Jung, Mayo Clinic, Rochester, Minnesota, USA.

Case #52
Clinical history:
A 33 year old man had an asymptomatic hand mass, which was excised.
Gross images:

Microscopic images:
Cytogenetic images:
What is your diagnosis?
Diagnosis: Chondroid lipoma
Discussion:
Chondroid lipoma is a rare, benign soft tissue tumor first described as a distinct entity in 1993 (Am J Surg Path 1993;17:1103). They are slow growing, painless masses of subcutaneous or deep soft tissue. 80% occur in females and age varies from 14 to 70 years. They typically occur in the extremities and limb girdles but may be incidental findings at hip replacement surgery (J Surg Orthop Adv 2004;13:42). They may also occur within the oral cavity, trunk and at other sites (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:331, Skeletal Radiol 2004;33:666).
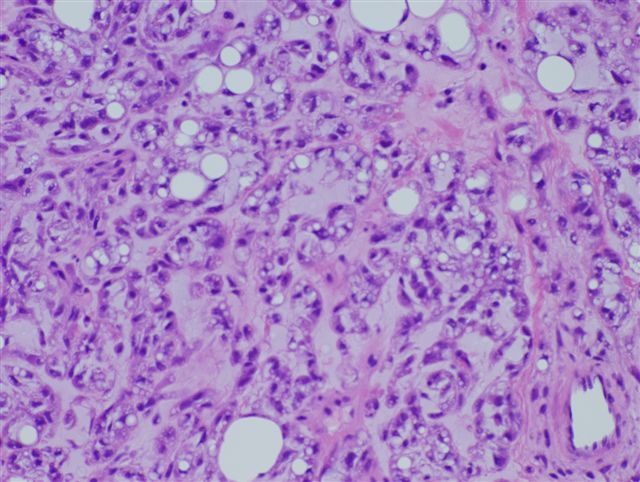
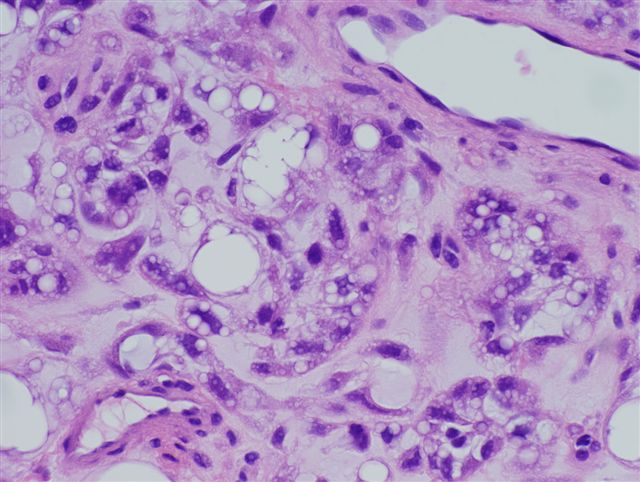
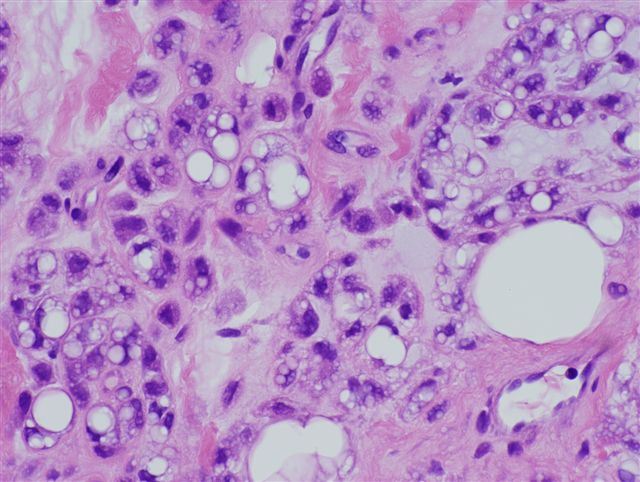
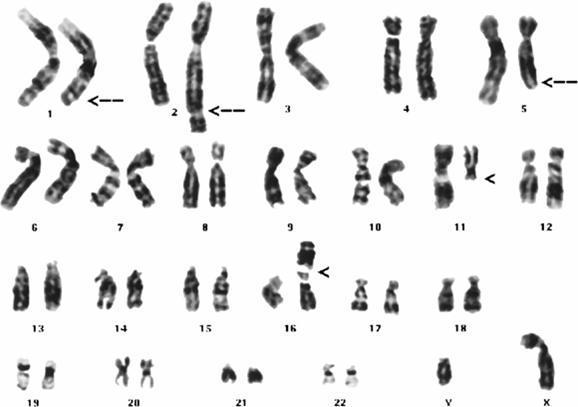
Grossly, these tumors range up to 11 cm, are encapsulated and yellow-white. Microscopically, they contain nests and cords of multivacuolated cells resembling lipoblasts within a prominent chondromyxoid matrix, with variable mature fat. Fine needle aspiration shows mixtures of mature lipocytes and lipoblast-like cells within a chondromyxoid matrix (Arch Path Lab Med 2001;125:1224). There is usually prominent vasculature with variable wall thickness. There is no pleomorphism, no atypia and no / rare mitotic activity. The tumor cells are immunoreactive for S100 and vimentin, with variable staining for CD68 and keratin (Hum Pathol 1995;26:706). They are negative for EMA, HMB45 and smooth muscle actin. Cytogenetics shows a t(11;16) translocation, which is also found in hibernomas (Am J Surg Path 1999;23:1300, Mod Pathol 1999;12:88). Electron microscopy shows abundant intracytoplasmic lipid and glycogen and numerous pinocytotic vesicles, characteristic of white adipocytes, which suggests that there is no true cartilaginous differentiation (Am J Surg Pathol 1995;19:1272).
Excision is curative. These tumors do not recur, metastasize or transform.
The differential diagnosis includes myxoid liposarcoma and extraskeletal myxoid chondrosarcoma. Myxoid liposarcoma contains a delicate, plexiform capillary matrix and true lipoblasts. Extraskeletal myxoid chondrosarcoma has fibrous septa and the chondroblasts typically lack intracytoplasmic vacuoles. It frequently contains mitotic figures and necrosis.
References: Radiographics 2004;24:1433 (benign musculoskeletal lipomatous lesions), Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Sungmi Jung, Mayo Clinic, Rochester, Minnesota, USA.
Website news:
(1) This case is sponsored by Sakura Finetek, USA. Leading the revolution in Pathology, the Tissue-Tek Xpress Rapid Tissue Processor is helping laboratories achieve new levels of productivity. Enabling a continuous flow of up to 40 cassettes every 15 minutes, this system can process up to 120 specimens per hour. The Xpress allows for a balanced distribution of work throughout the day, eliminating bottlenecks and batches common with overnight processing. Improved turnaround times, reduced waste and increased productivity are just a few benefits this technology can offer your lab. Results are the same or better than overnight processing. Help your lab reach its full potential with the Tissue-Tek Xpress Rapid Tissue Processor. For more information, contact Ms. Elise Green, Marketing Manager at 1-800-725-8723 extension 7873 or at egreen@sakuraus.com.
Visit and follow our Blog to see recent updates to the website.
(1) This case is sponsored by Sakura Finetek, USA. Leading the revolution in Pathology, the Tissue-Tek Xpress Rapid Tissue Processor is helping laboratories achieve new levels of productivity. Enabling a continuous flow of up to 40 cassettes every 15 minutes, this system can process up to 120 specimens per hour. The Xpress allows for a balanced distribution of work throughout the day, eliminating bottlenecks and batches common with overnight processing. Improved turnaround times, reduced waste and increased productivity are just a few benefits this technology can offer your lab. Results are the same or better than overnight processing. Help your lab reach its full potential with the Tissue-Tek Xpress Rapid Tissue Processor. For more information, contact Ms. Elise Green, Marketing Manager at 1-800-725-8723 extension 7873 or at egreen@sakuraus.com.
Visit and follow our Blog to see recent updates to the website.
Case #52
Clinical history:
A 33 year old man had an asymptomatic hand mass, which was excised.
Gross images:
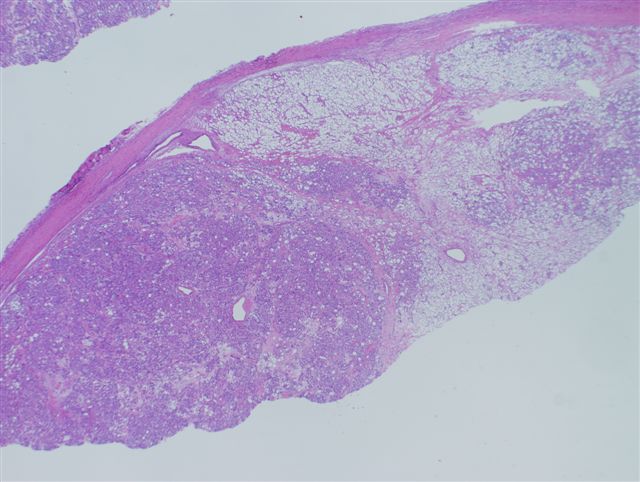
Microscopic images:
Low power
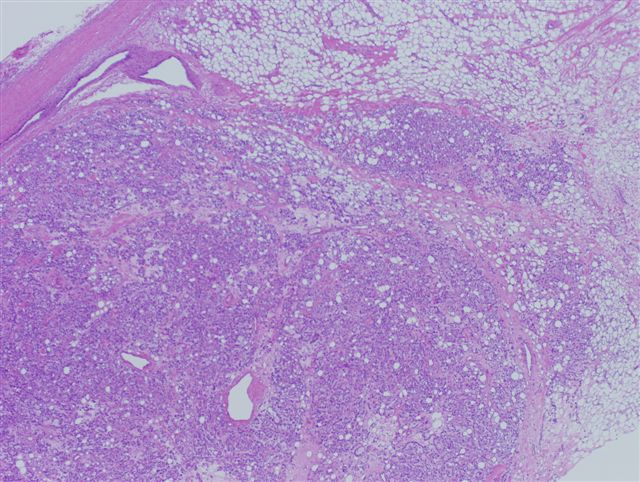
Medium power
Medium power
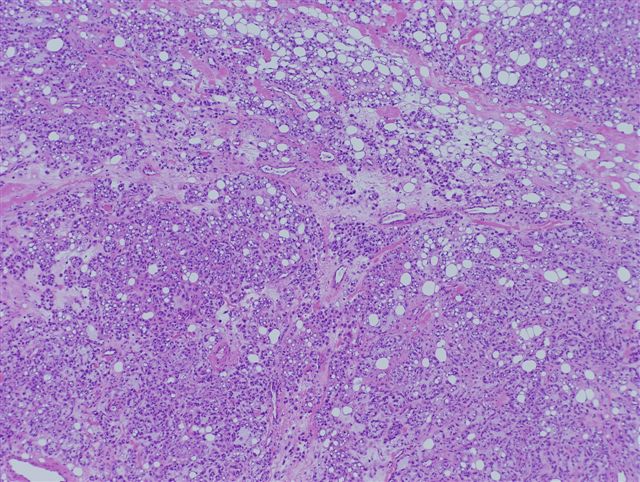
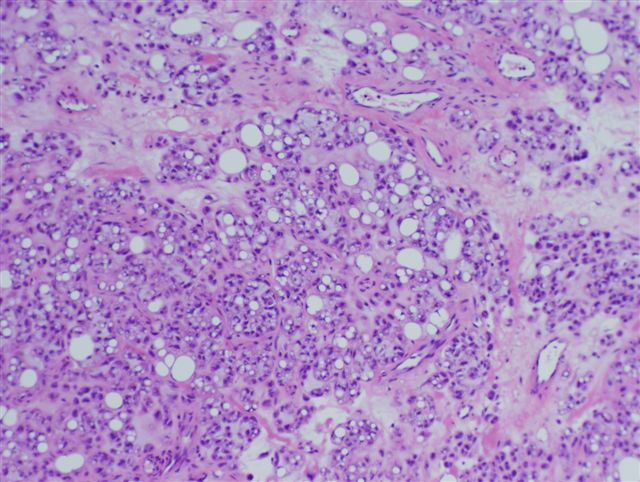
High power
High power
Cytogenetic images:
t(11;16)(q13;p12-13)
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Chondroid lipoma
Discussion:
Chondroid lipoma is a rare, benign soft tissue tumor first described as a distinct entity in 1993 (Am J Surg Path 1993;17:1103). They are slow growing, painless masses of subcutaneous or deep soft tissue. 80% occur in females and age varies from 14 to 70 years. They typically occur in the extremities and limb girdles but may be incidental findings at hip replacement surgery (J Surg Orthop Adv 2004;13:42). They may also occur within the oral cavity, trunk and at other sites (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:331, Skeletal Radiol 2004;33:666).
Grossly, these tumors range up to 11 cm, are encapsulated and yellow-white. Microscopically, they contain nests and cords of multivacuolated cells resembling lipoblasts within a prominent chondromyxoid matrix, with variable mature fat. Fine needle aspiration shows mixtures of mature lipocytes and lipoblast-like cells within a chondromyxoid matrix (Arch Path Lab Med 2001;125:1224). There is usually prominent vasculature with variable wall thickness. There is no pleomorphism, no atypia and no / rare mitotic activity. The tumor cells are immunoreactive for S100 and vimentin, with variable staining for CD68 and keratin (Hum Pathol 1995;26:706). They are negative for EMA, HMB45 and smooth muscle actin. Cytogenetics shows a t(11;16) translocation, which is also found in hibernomas (Am J Surg Path 1999;23:1300, Mod Pathol 1999;12:88). Electron microscopy shows abundant intracytoplasmic lipid and glycogen and numerous pinocytotic vesicles, characteristic of white adipocytes, which suggests that there is no true cartilaginous differentiation (Am J Surg Pathol 1995;19:1272).
Excision is curative. These tumors do not recur, metastasize or transform.
The differential diagnosis includes myxoid liposarcoma and extraskeletal myxoid chondrosarcoma. Myxoid liposarcoma contains a delicate, plexiform capillary matrix and true lipoblasts. Extraskeletal myxoid chondrosarcoma has fibrous septa and the chondroblasts typically lack intracytoplasmic vacuoles. It frequently contains mitotic figures and necrosis.
References: Radiographics 2004;24:1433 (benign musculoskeletal lipomatous lesions), Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
