
22 February 2006 - Case #37
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Lisa A. Cerilli, University of New Mexico Health Sciences, Albuquerque, New Mexico, USA.
Case #37
Clinical history:
A 49 year old healthy woman underwent needle localization excision of a breast mass for biopsy proven low grade ductal carcinoma in situ. A 9 mm lesion was identified histologically adjacent to but not involved by multifocal DCIS. The epithelial component in the nodule showed the typical cytoarchitecture of fibroadenoma but also had some atypical cells. No mitotic figures were found.
Microscopic images:

What is your diagnosis?
Diagnosis: Fibroadenoma with bizarre stromal giant cells (for this portion of the specimen)
Discussion:
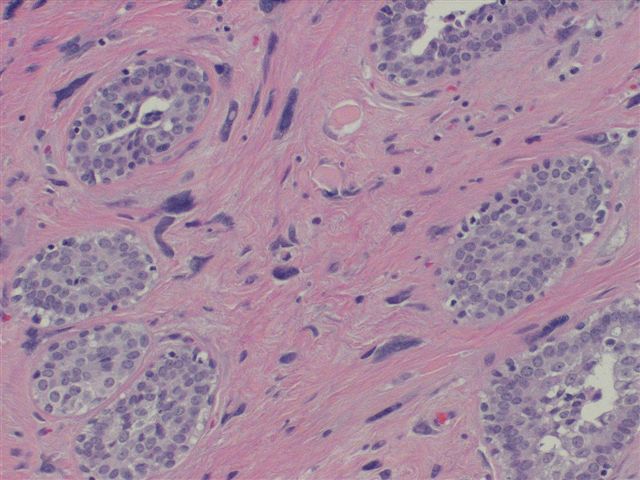
The microscopic images show stromal cells with markedly enlarged and hyperchromatic, pleomorphic nuclei. Many of the stromal cells showed multinucleated forms or prominent round, intranuclear pseudoinclusions. The remaining breast showed foci of DCIS with low grade nuclear features, which of course was included within the final diagnosis.
Well defined histological parameters typically are reliable indicators to differentiate benign from malignant entities. The presence of enlarged and pleomorphic nuclei is classically regarded as a feature of malignancy but may on occasion be evident in lesions with completely benign behavior. This discordance between nuclear atypia and behavior is characteristically encountered in uterine leiomyomas (referred to as symplastic change) or schwannomas (described as ancient change). Degenerative type atypia has also been described in osteoblastoma, chondromyxoid fibroma, fibrous dysplasia, renal oncocytoma, stromal hyperplasia of the prostate, endometrial polyps and salivary pleomorphic adenoma, as well as in endocrine neoplasms (Skeletal Radiol 2004;33:641, J Urol 2003;170:1951, Am J Surg Pathol 2002;26:505, Pathol Int 1999;49:993). Similar nuclear changes arising in mammary fibroadenomas are only seen rarely.
Architecturally, the overall pattern of fibroadenoma with bizarre stromal giant cells is that of the usual fibroadenoma but with diffuse striking nucleomegaly of the stromal cells, accompanied by adequate cytoplasm. Mitotic figures are notably absent. Other neoplastic lesions in the breast that show atypical stromal cells include phyllodes tumor, sarcoma and metaplastic breast carcinoma. Distinction from these other lesions can be made by recognition of the lack of stromal overgrowth, cellular crowding and mitotic figures and most importantly, the lack of crisp nuclear details (i.e., the chromatin is smudgy). The presence of multinucleated giant cells in combination with mitotic activity, necrosis, stromal overgrowth or hypercellularity raises the question of another lesion, usually phyllodes tumor (Pathology 2001;33:153). The degree of atypia in fibroadenoma with bizarre stromal giant cells actually exceeds that which typifies malignant processes in the breast, another diagnostic clue.
Bizarre nuclear alteration in the presence of abundant cytoplasm may also be seen following external beam radiation therapy. Due to radiation induced inhibition of cell division, the nucleus becomes enlarged, acquiring bizarre features including pseudoinclusions. Unlike radiation effect, fibroadenoma with bizarre stromal giant cells shows no epithelial or vascular abnormalities, the atypia is well localized and there is no history of radiation exposure.
Fibroadenoma with bizarre stromal cells is an uncommon benign entity in the breast which can be easily confused with phyllodes tumor or other lesions with malignant stromal cells, particularly in fine needle aspirations (Acta Cytol 2002;46:535). The bizarre nuclear changes are related to degenerative alterations and they do not indicate aggressive or malignant behavior. Treatment is conservative local excision, which is completely curative.
References: Skeletal Radiol 2004;33:641, J Urol 2003;170:1951, Am J Surg Pathol 2002;26:505, Pathol Int 1999;49:993, Pathology 2001;33:153, Acta Cytol 2002;46:535
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Lisa A. Cerilli, University of New Mexico Health Sciences, Albuquerque, New Mexico, USA.
Case #37
Clinical history:
A 49 year old healthy woman underwent needle localization excision of a breast mass for biopsy proven low grade ductal carcinoma in situ. A 9 mm lesion was identified histologically adjacent to but not involved by multifocal DCIS. The epithelial component in the nodule showed the typical cytoarchitecture of fibroadenoma but also had some atypical cells. No mitotic figures were found.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Fibroadenoma with bizarre stromal giant cells (for this portion of the specimen)
Discussion:
The microscopic images show stromal cells with markedly enlarged and hyperchromatic, pleomorphic nuclei. Many of the stromal cells showed multinucleated forms or prominent round, intranuclear pseudoinclusions. The remaining breast showed foci of DCIS with low grade nuclear features, which of course was included within the final diagnosis.
Well defined histological parameters typically are reliable indicators to differentiate benign from malignant entities. The presence of enlarged and pleomorphic nuclei is classically regarded as a feature of malignancy but may on occasion be evident in lesions with completely benign behavior. This discordance between nuclear atypia and behavior is characteristically encountered in uterine leiomyomas (referred to as symplastic change) or schwannomas (described as ancient change). Degenerative type atypia has also been described in osteoblastoma, chondromyxoid fibroma, fibrous dysplasia, renal oncocytoma, stromal hyperplasia of the prostate, endometrial polyps and salivary pleomorphic adenoma, as well as in endocrine neoplasms (Skeletal Radiol 2004;33:641, J Urol 2003;170:1951, Am J Surg Pathol 2002;26:505, Pathol Int 1999;49:993). Similar nuclear changes arising in mammary fibroadenomas are only seen rarely.
Architecturally, the overall pattern of fibroadenoma with bizarre stromal giant cells is that of the usual fibroadenoma but with diffuse striking nucleomegaly of the stromal cells, accompanied by adequate cytoplasm. Mitotic figures are notably absent. Other neoplastic lesions in the breast that show atypical stromal cells include phyllodes tumor, sarcoma and metaplastic breast carcinoma. Distinction from these other lesions can be made by recognition of the lack of stromal overgrowth, cellular crowding and mitotic figures and most importantly, the lack of crisp nuclear details (i.e., the chromatin is smudgy). The presence of multinucleated giant cells in combination with mitotic activity, necrosis, stromal overgrowth or hypercellularity raises the question of another lesion, usually phyllodes tumor (Pathology 2001;33:153). The degree of atypia in fibroadenoma with bizarre stromal giant cells actually exceeds that which typifies malignant processes in the breast, another diagnostic clue.
Bizarre nuclear alteration in the presence of abundant cytoplasm may also be seen following external beam radiation therapy. Due to radiation induced inhibition of cell division, the nucleus becomes enlarged, acquiring bizarre features including pseudoinclusions. Unlike radiation effect, fibroadenoma with bizarre stromal giant cells shows no epithelial or vascular abnormalities, the atypia is well localized and there is no history of radiation exposure.
Fibroadenoma with bizarre stromal cells is an uncommon benign entity in the breast which can be easily confused with phyllodes tumor or other lesions with malignant stromal cells, particularly in fine needle aspirations (Acta Cytol 2002;46:535). The bizarre nuclear changes are related to degenerative alterations and they do not indicate aggressive or malignant behavior. Treatment is conservative local excision, which is completely curative.
References: Skeletal Radiol 2004;33:641, J Urol 2003;170:1951, Am J Surg Pathol 2002;26:505, Pathol Int 1999;49:993, Pathology 2001;33:153, Acta Cytol 2002;46:535
