
4 June 2005 - Case #9
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Irving Dardick, Pathology Images, Inc., PathologyImagesInc.com, Ottawa, Ontario, Canada.
Case #9
Clinical history:
A 47 year old man complained of intermittent chest pain for some weeks and a chest Xray revealed a 2.5 cm pleural based lesion. Clinically, diagnoses such as fibroma, mesothelioma or carcinoma were considered.
A fine needle aspiration biopsy was performed. Adequate fragments of tissue were obtained and a cell block was prepared. Fragments from the needle rinse were also prepared for electron microscopy.
Cytology images:

Electron microscopy images:
Cytology description:
The FNA fragments consisted of cohesive spindle cells with indistinct cell membranes and fibrillar cytoplasm. There was focal palisading of the nuclei, which were oval and slender and either short or elongated with inconspicuous nucleoli. Chromatin was finely granular.
Electron microscopy description:
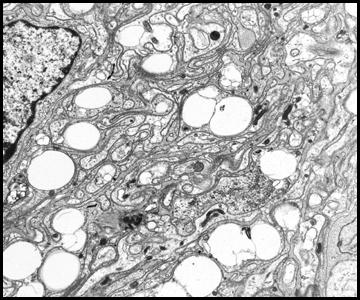
Image #1 shows compactly organized spindle cells with numerous cytoplasmic lipid droplets. Images #2 and 3 show numerous, narrow cytoplasmic processes, which were intricately associated and intertwined and had external lamina on their outer aspect (white arrows). The cytoplasmic processes contained only infrequent organelles.
What is your diagnosis?
Diagnosis: Schwannoma
Stain image:

Discussion:
This combination of features was diagnostic of a schwannoma, apparently developing from an intercostal nerve. The diagnosis was confirmed by S100 protein immunostaining of the cell block, which was diffusely positive (image). In this case, according to the contributor, the H&Es by themselves were not considered to be diagnostic and ultrastructural diagnosis saved the patient the discomfort and expense of a thoracotomy. When the benign nature of this small tumor was explained to the patient and the therapeutic treatments considered, he opted not to have the lesion resected. At follow up 3 years later, the patient was asymptomatic and the schwannoma had not substantially increased in size.
The diagnosis of schwannoma may be difficult from an FNA, due to hypocellularity that makes the FNA nondiagnostic, cellular material that resembles granulation tissue or granulomatous inflammation or the inability to rule out other spindle cell tumors (Cytopathology 1999;10:186).
The typical fine needle aspiration of schwannoma shows aggregates of spindle cells with indistinct cytoplasm, and elongate nuclei with blunt pointed ends. The chromatin is finely granular and uniformly distributed and nuclear inclusions may be present. Occasionally, nuclear palisading is found but Verocay bodies are only rarely present. Nucleoli are not prominent. No isolated tumor cells are seen. Schwannomas can have degenerative features (ancient schwannoma), resulting in nuclear pleomorphism and mimicking sarcoma. However, the chromatin of ancient schwannomas is homogenous and smudged. Mitotic figures are usually not seen.
In this case, the differential diagnosis should also include malignant peripheral nerve sheath tumor. MPNSTs are usually more cellular than schwannomas, with a higher proportion of individually dispersed tumor cells, particularly at the edge of the aggregate and more nuclear pleomorphism. For pleural based lesions, solitary fibrous tumor and fibrous mesothelioma should be considered. Near salivary glands, the differential diagnosis should include a pleomorphic adenoma with sparse epithelial areas (Diagn Cytopathol 2002;27:53).
Reference: Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Irving Dardick, Pathology Images, Inc., PathologyImagesInc.com, Ottawa, Ontario, Canada.
Website news:
(1) This week's case is sponsored by our Books page, which is revised weekly with new titles of interest to pathologists. You may need a book in a particular area of pathology, but how do you know what books are available? Our Books page lists all books of interest to pathologists available from Amazon.com, published since 2000, and organized by subspecialty topic and by author. Each book listed is accompanied by the publication date, a description, links to book reviews and links to Amazon.com or the publisher for purchase. Contact us to add any books that we missed or to post a book review that you wrote.
Visit and follow our Blog to see recent updates to the website.
(1) This week's case is sponsored by our Books page, which is revised weekly with new titles of interest to pathologists. You may need a book in a particular area of pathology, but how do you know what books are available? Our Books page lists all books of interest to pathologists available from Amazon.com, published since 2000, and organized by subspecialty topic and by author. Each book listed is accompanied by the publication date, a description, links to book reviews and links to Amazon.com or the publisher for purchase. Contact us to add any books that we missed or to post a book review that you wrote.
Visit and follow our Blog to see recent updates to the website.
Case #9
Clinical history:
A 47 year old man complained of intermittent chest pain for some weeks and a chest Xray revealed a 2.5 cm pleural based lesion. Clinically, diagnoses such as fibroma, mesothelioma or carcinoma were considered.
A fine needle aspiration biopsy was performed. Adequate fragments of tissue were obtained and a cell block was prepared. Fragments from the needle rinse were also prepared for electron microscopy.
Cytology images:
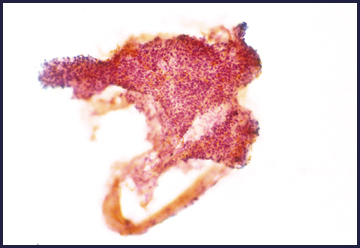
Fine needle aspirate biopsy
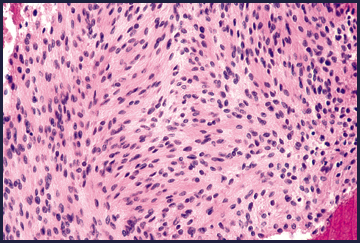
Cell block
Electron microscopy images:
Cytology description:
The FNA fragments consisted of cohesive spindle cells with indistinct cell membranes and fibrillar cytoplasm. There was focal palisading of the nuclei, which were oval and slender and either short or elongated with inconspicuous nucleoli. Chromatin was finely granular.
Electron microscopy description:
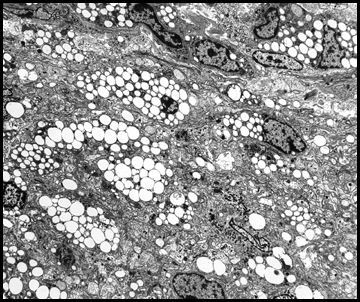
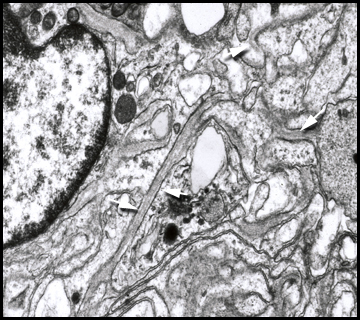
Image #1 shows compactly organized spindle cells with numerous cytoplasmic lipid droplets. Images #2 and 3 show numerous, narrow cytoplasmic processes, which were intricately associated and intertwined and had external lamina on their outer aspect (white arrows). The cytoplasmic processes contained only infrequent organelles.
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Schwannoma
Stain image:
S100
Discussion:
This combination of features was diagnostic of a schwannoma, apparently developing from an intercostal nerve. The diagnosis was confirmed by S100 protein immunostaining of the cell block, which was diffusely positive (image). In this case, according to the contributor, the H&Es by themselves were not considered to be diagnostic and ultrastructural diagnosis saved the patient the discomfort and expense of a thoracotomy. When the benign nature of this small tumor was explained to the patient and the therapeutic treatments considered, he opted not to have the lesion resected. At follow up 3 years later, the patient was asymptomatic and the schwannoma had not substantially increased in size.
The diagnosis of schwannoma may be difficult from an FNA, due to hypocellularity that makes the FNA nondiagnostic, cellular material that resembles granulation tissue or granulomatous inflammation or the inability to rule out other spindle cell tumors (Cytopathology 1999;10:186).
The typical fine needle aspiration of schwannoma shows aggregates of spindle cells with indistinct cytoplasm, and elongate nuclei with blunt pointed ends. The chromatin is finely granular and uniformly distributed and nuclear inclusions may be present. Occasionally, nuclear palisading is found but Verocay bodies are only rarely present. Nucleoli are not prominent. No isolated tumor cells are seen. Schwannomas can have degenerative features (ancient schwannoma), resulting in nuclear pleomorphism and mimicking sarcoma. However, the chromatin of ancient schwannomas is homogenous and smudged. Mitotic figures are usually not seen.
In this case, the differential diagnosis should also include malignant peripheral nerve sheath tumor. MPNSTs are usually more cellular than schwannomas, with a higher proportion of individually dispersed tumor cells, particularly at the edge of the aggregate and more nuclear pleomorphism. For pleural based lesions, solitary fibrous tumor and fibrous mesothelioma should be considered. Near salivary glands, the differential diagnosis should include a pleomorphic adenoma with sparse epithelial areas (Diagn Cytopathol 2002;27:53).
Reference: Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
