
28 April 2005 - Case of the Week #5
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case is sponsored by PSA, who invites you to attend its 2005 Pathology Business Retreat on May 12-14 in San Antonio, Texas. The meeting will be held at the Plaza San Antonio, just a few steps from the San Antonio Riverwalk and the historic Alamo. To succeed in today's environment, pathologists must be efficient, informed and competitive. To that end, PSA and Dennis Weissman, founder of Washington G-2 Reports and meeting moderator, have assembled a group of informed leaders for a powerful program on timely business and leadership issues.
This case was contributed by Dr. David S. Brenner, Assistant Medical Director, Department of Pathology and Director, Division of Microbiology, Bayhealth Medical Center in Dover, Delaware (USA).
Case of the Week #5
Clinical history:
A 20 year old woman presented to her surgeon for removal of what had been diagnosed previously as an extranumerary nipple on her left breast.
Microscopic description:
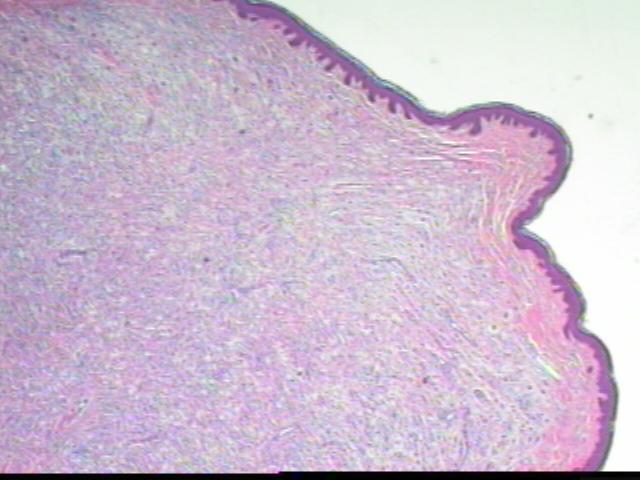
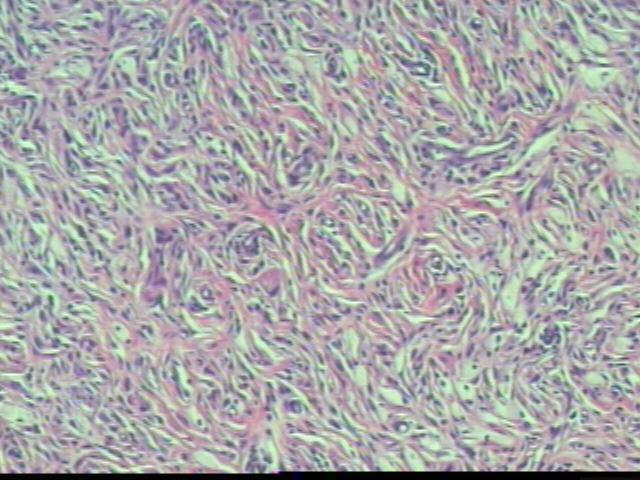
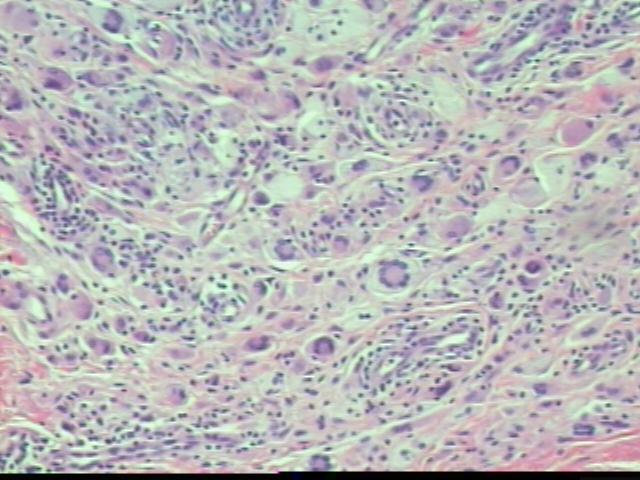
The dermis contains a fibrohistiocytic lesion with lymphocytes and numerous Touton giant cells. No epidermal involvement by tumor is noted. There are no mitotic figures and only occasional mild nuclear atypia, which appears to be degenerative.
Microscopic images:


What is your diagnosis?
Diagnosis: Juvenile xanthogranuloma
Discussion:
Juvenile xanthogranuloma, also called nevoxanthoendothelioma, is an uncommon (< 0.5% of pediatric tumors in one study), benign fibrohistiocytic lesion of infants or young adults. It often appears in the skin of the face or trunk, less commonly in the subcutis, skeletal muscle, eye, peripheral nerve or testis. Multiple lesions are present in 20% of patients, usually males. Some lesions involute spontaneously leaving a depressed and variably hyperpigmented area of skin. Treatment is conservative excision, with a relapse rate of 7% in one study. Neonates rarely develop systemic disease requiring chemotherapy to prevent death from hepatic failure (giant cell hepatitis and tumor in liver and viscera) or other causes.
Cutaneous lesions are usually small, from 0.1 - 2.0 cm, yellow-red and papulonodular. They contain a dense dermal infiltrate of lymphocytes, histiocytes, Touton giant cells (usually), eosinophils and neutrophils, which may extend into the subcutis. Over time, the epidermis thins out and the rete ridges become elongated. Extracutaneous lesions may lack the Touton giant cells.
Note: histiocytic giant cells may be Touton type (ring of nuclei surrounding foamy cytoplasm with cytoplasm usually also visible around the nuclei), Langhans type (nuclei form a horseshoe arrangement, not necessary a distinct category from Touton type) or foreign body type (haphazard nuclear arrangement).
Immunostains are usually not necessary for diagnosis. The Touton giant cells and histiocytes are CD68+, HAM56+ and Factor XIIIa+. These cells are negative for S100 and CD1a.
The differential diagnosis includes Langerhans cell histiocytosis, a more common disorder of childhood. These tumor cells have coffee bean nuclei (nuclear grooves) which are S100+ and CD1a+, and negative for CD68, HAM56 and Factor XIIIa. No Touton giant cells are present. Electron microscopy shows characteristic Birbeck granules. Xanthomas contain a uniform collection of foam cells and variable Touton giant cells but lack the other inflammatory cells of juvenile xanthogranuloma. They are often associated with hyperlipidemia. Benign fibrous histiocytoma usually has a storiform pattern.
Additional references: AAJSP 2003;27:579, AJSP 2005;29:21
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case is sponsored by PSA, who invites you to attend its 2005 Pathology Business Retreat on May 12-14 in San Antonio, Texas. The meeting will be held at the Plaza San Antonio, just a few steps from the San Antonio Riverwalk and the historic Alamo. To succeed in today's environment, pathologists must be efficient, informed and competitive. To that end, PSA and Dennis Weissman, founder of Washington G-2 Reports and meeting moderator, have assembled a group of informed leaders for a powerful program on timely business and leadership issues.
This case was contributed by Dr. David S. Brenner, Assistant Medical Director, Department of Pathology and Director, Division of Microbiology, Bayhealth Medical Center in Dover, Delaware (USA).
Case of the Week #5
Clinical history:
A 20 year old woman presented to her surgeon for removal of what had been diagnosed previously as an extranumerary nipple on her left breast.
Microscopic description:
The dermis contains a fibrohistiocytic lesion with lymphocytes and numerous Touton giant cells. No epidermal involvement by tumor is noted. There are no mitotic figures and only occasional mild nuclear atypia, which appears to be degenerative.
Microscopic images:
Low power
Medium power
High power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Juvenile xanthogranuloma
Discussion:
Juvenile xanthogranuloma, also called nevoxanthoendothelioma, is an uncommon (< 0.5% of pediatric tumors in one study), benign fibrohistiocytic lesion of infants or young adults. It often appears in the skin of the face or trunk, less commonly in the subcutis, skeletal muscle, eye, peripheral nerve or testis. Multiple lesions are present in 20% of patients, usually males. Some lesions involute spontaneously leaving a depressed and variably hyperpigmented area of skin. Treatment is conservative excision, with a relapse rate of 7% in one study. Neonates rarely develop systemic disease requiring chemotherapy to prevent death from hepatic failure (giant cell hepatitis and tumor in liver and viscera) or other causes.
Cutaneous lesions are usually small, from 0.1 - 2.0 cm, yellow-red and papulonodular. They contain a dense dermal infiltrate of lymphocytes, histiocytes, Touton giant cells (usually), eosinophils and neutrophils, which may extend into the subcutis. Over time, the epidermis thins out and the rete ridges become elongated. Extracutaneous lesions may lack the Touton giant cells.
Note: histiocytic giant cells may be Touton type (ring of nuclei surrounding foamy cytoplasm with cytoplasm usually also visible around the nuclei), Langhans type (nuclei form a horseshoe arrangement, not necessary a distinct category from Touton type) or foreign body type (haphazard nuclear arrangement).
Immunostains are usually not necessary for diagnosis. The Touton giant cells and histiocytes are CD68+, HAM56+ and Factor XIIIa+. These cells are negative for S100 and CD1a.
The differential diagnosis includes Langerhans cell histiocytosis, a more common disorder of childhood. These tumor cells have coffee bean nuclei (nuclear grooves) which are S100+ and CD1a+, and negative for CD68, HAM56 and Factor XIIIa. No Touton giant cells are present. Electron microscopy shows characteristic Birbeck granules. Xanthomas contain a uniform collection of foam cells and variable Touton giant cells but lack the other inflammatory cells of juvenile xanthogranuloma. They are often associated with hyperlipidemia. Benign fibrous histiocytoma usually has a storiform pattern.
Additional references: AAJSP 2003;27:579, AJSP 2005;29:21
