
22 April 2005 - Case of the Week #4
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case is sponsored by Vachette Pathology, who specializes in providing billing auditing, managed care contracting and marketing services for pathology practices.
This case was contributed by Dr. Hind Nassar, Wayne State University Department of Pathology, Detroit, Michigan (USA), who we thank for contributing to the education of pathologists worldwide.
Case of the Week #4
Clinical history:
The specific clinical information is unavailable for this patient but a typical patient is a 59 year old woman with a 2 cm breast mass, who underwent lumpectomy and axillary dissection. Gross images are not available.
Microscopic description:
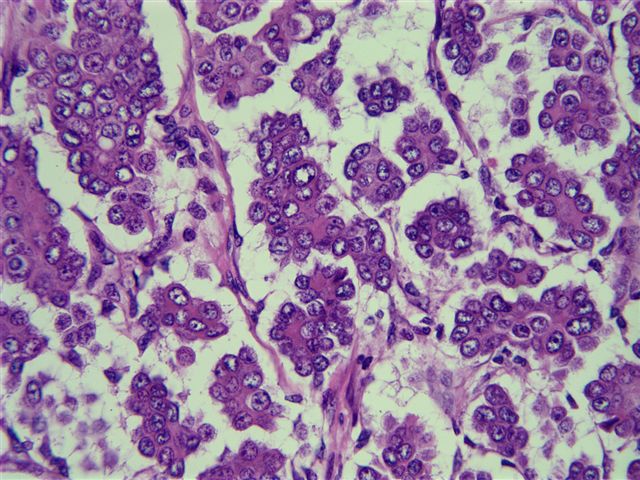
The tumor is composed of distinct clusters (micropapillae) of cells floating in clear spaces that resemble lymphatics, although no definite lining is identified. The tumor cells have abundant eosinophilic cytoplasm, round vesicular nuclei and prominent nucleoli. The clefting surrounding each cluster of tumor cells is particularly noteworthy but does not actually represent lymphovascular invasion in most cases. The MUC1 antibody stains the border of each cluster. A lymph node shows involvement of similar types of cells.
Microscopic images:



What is your diagnosis?
Diagnosis: Invasive micropapillary carcinoma of the breast (metastatic to lymph node)
Discussion:
Invasive micropapillary carcinoma of the breast is a rare tumor, representing < 2% of all invasive breast carcinomas. It was first described by Tavassoli (Mod Path 1993;6:660). The mean age of patients is 59 years, range 25 - 92 years. Similar tumors have been reported in the urinary bladder, lung and major salivary glands.
The tumor is composed of micropapillae or tight clusters of cells floating in well delineated clear spaces resembling lymphatics (although most are not actually lymphatics), separated by a fibrocollagenous or delicate fibrovascular stroma. The micropapillary structures themselves lack a true fibrovascular core. These tumors tend to be high grade, with a high rate of actual lymphovascular invasion and nodal metastases in 90 - 100% of cases. Psammoma bodies are often identified. Tumors have low rates of immunostaining for estrogen and progesterone receptors (20 - 35%) but high rates of HER2 overexpression (95%) and p53 expression (70%). MUC1 shows unusual immunoreactivity limited to the basal surface of the cells, accentuating the outlines of the micropapillary units. In conventional breast adenocarcinomas, MUC1 is usually intracytoplasmic or apical. This suggests that reversal of cell orientation is as an important factor in the morphogenesis and possibly the pathogenesis of invasive micropapillary carcinoma.
A micropapillary pattern occurs in 6% of all breast carcinomas, usually mixed with infiltrating ductal carcinoma or variants and only rarely occurs in a pure form. Clinicopathologic characteristics do not appear to depend on the amount of the micropapillary component. The micropapillary pattern is usually retained in metastatic foci and areas of recurrence.
Breast carcinomas with an invasive micropapillary component are very aggressive, with 95% of patients presenting with nodal metastases. Recurrences occur in 70% of patients and 50% of patients die of disease.
The differential diagnosis includes metastatic ovarian serous papillary carcinoma and extensive lymphovascular invasion by a primary or metastatic breast carcinoma.
Additional references: Adv Anat Path 2004;11:297, AJCP 2004;121:857, Mod Path 2004;17:1045, Mod Path 2001;14:836
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case is sponsored by Vachette Pathology, who specializes in providing billing auditing, managed care contracting and marketing services for pathology practices.
This case was contributed by Dr. Hind Nassar, Wayne State University Department of Pathology, Detroit, Michigan (USA), who we thank for contributing to the education of pathologists worldwide.
Case of the Week #4
Clinical history:
The specific clinical information is unavailable for this patient but a typical patient is a 59 year old woman with a 2 cm breast mass, who underwent lumpectomy and axillary dissection. Gross images are not available.
Microscopic description:
The tumor is composed of distinct clusters (micropapillae) of cells floating in clear spaces that resemble lymphatics, although no definite lining is identified. The tumor cells have abundant eosinophilic cytoplasm, round vesicular nuclei and prominent nucleoli. The clefting surrounding each cluster of tumor cells is particularly noteworthy but does not actually represent lymphovascular invasion in most cases. The MUC1 antibody stains the border of each cluster. A lymph node shows involvement of similar types of cells.
Microscopic images:
Low power
High power
MUC1 stain
Lymph node
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Invasive micropapillary carcinoma of the breast (metastatic to lymph node)
Discussion:
Invasive micropapillary carcinoma of the breast is a rare tumor, representing < 2% of all invasive breast carcinomas. It was first described by Tavassoli (Mod Path 1993;6:660). The mean age of patients is 59 years, range 25 - 92 years. Similar tumors have been reported in the urinary bladder, lung and major salivary glands.
The tumor is composed of micropapillae or tight clusters of cells floating in well delineated clear spaces resembling lymphatics (although most are not actually lymphatics), separated by a fibrocollagenous or delicate fibrovascular stroma. The micropapillary structures themselves lack a true fibrovascular core. These tumors tend to be high grade, with a high rate of actual lymphovascular invasion and nodal metastases in 90 - 100% of cases. Psammoma bodies are often identified. Tumors have low rates of immunostaining for estrogen and progesterone receptors (20 - 35%) but high rates of HER2 overexpression (95%) and p53 expression (70%). MUC1 shows unusual immunoreactivity limited to the basal surface of the cells, accentuating the outlines of the micropapillary units. In conventional breast adenocarcinomas, MUC1 is usually intracytoplasmic or apical. This suggests that reversal of cell orientation is as an important factor in the morphogenesis and possibly the pathogenesis of invasive micropapillary carcinoma.
A micropapillary pattern occurs in 6% of all breast carcinomas, usually mixed with infiltrating ductal carcinoma or variants and only rarely occurs in a pure form. Clinicopathologic characteristics do not appear to depend on the amount of the micropapillary component. The micropapillary pattern is usually retained in metastatic foci and areas of recurrence.
Breast carcinomas with an invasive micropapillary component are very aggressive, with 95% of patients presenting with nodal metastases. Recurrences occur in 70% of patients and 50% of patients die of disease.
The differential diagnosis includes metastatic ovarian serous papillary carcinoma and extensive lymphovascular invasion by a primary or metastatic breast carcinoma.
Additional references: Adv Anat Path 2004;11:297, AJCP 2004;121:857, Mod Path 2004;17:1045, Mod Path 2001;14:836
