
14 October 2005 - Case #23
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Gerard Abadjian, Hotel-Dieu de France, Beirut, Lebanon.
Case #23
Clinical history:
An 80 year old man was admitted for open biopsy of a lung nodule. 9 months previous, the patient noticed edema of the face and neck region, which disappeared 2 months later. Since that time, he had a generalized pruritis and a weight loss of 6 kg but no other symptoms.
A workup disclosed a positive PPD, multiple, diffusely enlarged mediastinal lymph nodes and a venous thrombosis extending to the left jugular vein.
Pulmonary endoscopy biopsy, bronchial washings and mediastinoscopy were nonconclusive. A surgical biopsy was performed.
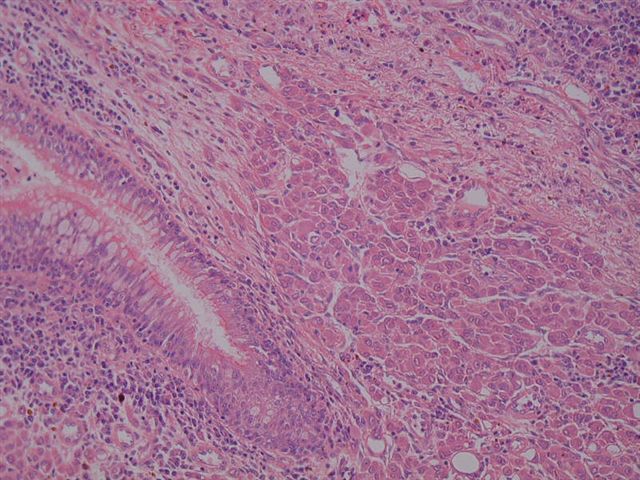
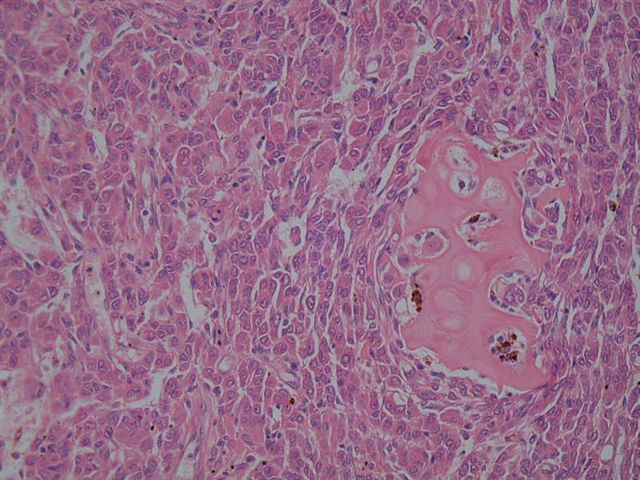
Microscopic images:

What is your diagnosis?
Diagnosis: Epithelioid angiosarcoma
Stains images:
Discussion:
Epithelioid angiosarcoma is characterized by sheets of tumor cells with vascular spaces lined by polygonal or oval cells with abundant eosinophilic cytoplasm and large, atypical nuclei. Vasoformative areas (irregular sinusoidal vascular channels) are less common than in classic angiosarcomas. There often is intra-arterial or lymphagitic spread (Arch Pathol Lab Med 2005;129:e7). The tumor is accompanied by hemorrhage, necrosis and mitotic figures. Focal hemangioendothelioma-like areas with intracytoplasmic lumina may be present. Tumor cells typically are immunoreactive for endothelial cell markers such as CD31, CD34 and factor VIII related antigen, although all vascular markers may not be immunoreactive. They are also immunoreactive for vimentin and often express cytokeratins.
Primary epithelioid angiosarcomas of the lung are unusual, with less than 20 cases reported and the differential diagnosis includes the much more common metastatic tumor (Arch Bronconeumol 2004;40:188). Metastatic angiosarcomas typically present with dyspnea, chest pain or hemoptysis, with multiple lung nodules identified radiologically. Among all angiosarcomas metastatic to the lung, the primary is only identified at presentation half of the time, often in skin, soft tissue or the right atrium (Mod Pathol 2001;14:1216).
The differential diagnosis also includes epithelioid hemangioendothelioma, a low grade sarcoma that typically affects middle aged women. These tumors tend to be acellular centrally and more cellular at the periphery. The tumor cells have eosinophilic and often vacuolated cytoplasm, with bland or only mildly atypical nuclei. The stroma may have myxochondroid features. Hemorrhage, necrosis and mitotic figures are not prominent. Melanoma and carcinoma may be differentiated based on immunostains, with the caveat that epithelioid angiosarcomas are often cytokeratin positive.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Gerard Abadjian, Hotel-Dieu de France, Beirut, Lebanon.
Case #23
Clinical history:
An 80 year old man was admitted for open biopsy of a lung nodule. 9 months previous, the patient noticed edema of the face and neck region, which disappeared 2 months later. Since that time, he had a generalized pruritis and a weight loss of 6 kg but no other symptoms.
A workup disclosed a positive PPD, multiple, diffusely enlarged mediastinal lymph nodes and a venous thrombosis extending to the left jugular vein.
Pulmonary endoscopy biopsy, bronchial washings and mediastinoscopy were nonconclusive. A surgical biopsy was performed.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Epithelioid angiosarcoma
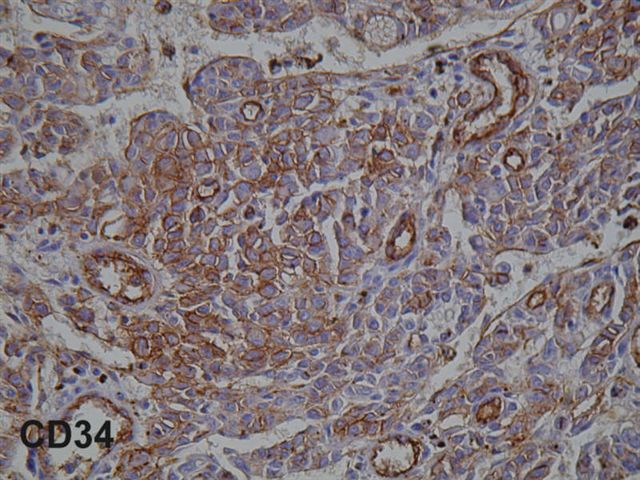
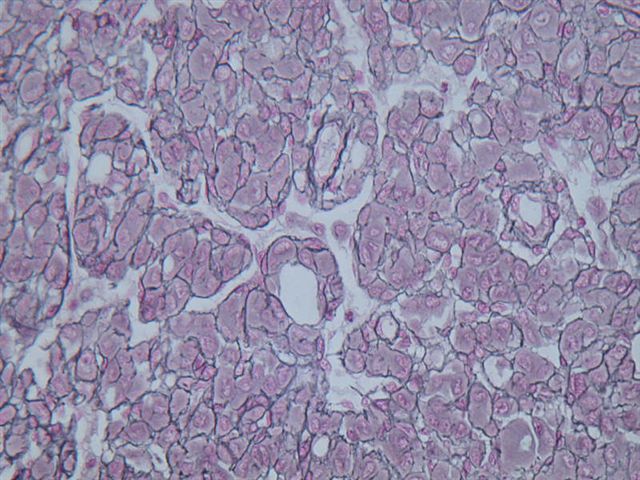
Stains images:
CD34
Reticulin
Discussion:
Epithelioid angiosarcoma is characterized by sheets of tumor cells with vascular spaces lined by polygonal or oval cells with abundant eosinophilic cytoplasm and large, atypical nuclei. Vasoformative areas (irregular sinusoidal vascular channels) are less common than in classic angiosarcomas. There often is intra-arterial or lymphagitic spread (Arch Pathol Lab Med 2005;129:e7). The tumor is accompanied by hemorrhage, necrosis and mitotic figures. Focal hemangioendothelioma-like areas with intracytoplasmic lumina may be present. Tumor cells typically are immunoreactive for endothelial cell markers such as CD31, CD34 and factor VIII related antigen, although all vascular markers may not be immunoreactive. They are also immunoreactive for vimentin and often express cytokeratins.
Primary epithelioid angiosarcomas of the lung are unusual, with less than 20 cases reported and the differential diagnosis includes the much more common metastatic tumor (Arch Bronconeumol 2004;40:188). Metastatic angiosarcomas typically present with dyspnea, chest pain or hemoptysis, with multiple lung nodules identified radiologically. Among all angiosarcomas metastatic to the lung, the primary is only identified at presentation half of the time, often in skin, soft tissue or the right atrium (Mod Pathol 2001;14:1216).
The differential diagnosis also includes epithelioid hemangioendothelioma, a low grade sarcoma that typically affects middle aged women. These tumors tend to be acellular centrally and more cellular at the periphery. The tumor cells have eosinophilic and often vacuolated cytoplasm, with bland or only mildly atypical nuclei. The stroma may have myxochondroid features. Hemorrhage, necrosis and mitotic figures are not prominent. Melanoma and carcinoma may be differentiated based on immunostains, with the caveat that epithelioid angiosarcomas are often cytokeratin positive.
