
22 September 2005 - Case #21
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Shylashree Chikkamuniyappa Edalur, Hematopathology fellow, University of Texas Health Science Center, San Antonio, Texas, USA.
Case #21
Clinical history:
The patient is a 64 year old Japanese woman with a history of disseminated nocardial infection, with abscesses in the brain and lung and a facial herpetic infection. A complete blood count showed a hemogloblin of 12.2, platelet count of 313 and elevated white blood cell count of 45.6 with 73% lymphocytes.
A bone marrow biopsy was hypercellular for age with 15% large, atypical cells.
Flow cytometry of peripheral blood showed bright CD45 / LCA staining with 98% T cells. 98% of the T cells marked with CD2, CD3, CD4 and CD5 and 4% marked with CD8 and CD7.
Other lab tests were calcium of 8.4 mg/dl, LDH: 452 U/L (high), HTLV1: 2+ positive by ELISA, Western Blot: bands present at p16, gp21 and gp46-1.
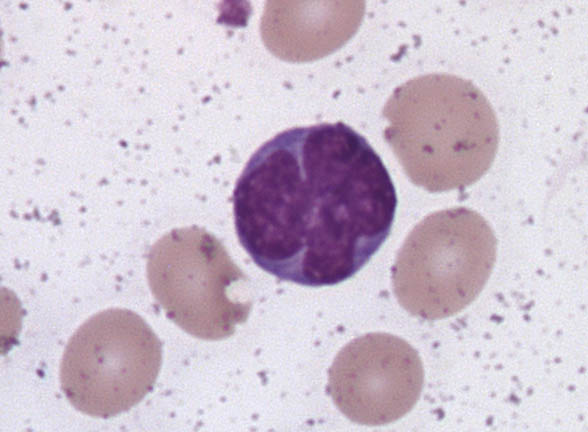
Peripheral blood images:



What is your diagnosis?
Diagnosis: Adult T cell leukemia / lymphoma
Discussion:
Adult T cell leukemia / lymphoma occurs most commonly where the HTLV1 retrovirus (human T cell leukemia virus 1) is endemic, namely in southwest Japan, western or central Africa, South America, the Caribbean and the southeast U.S. Infection is sexually transmitted or spreads from mother to child (through the placenta or breast milk), through intravenous drug abuse or blood transfusion. There is usually a delay of several decades before clinical features appear. Leukemia / lymphoma occurs in 1 - 5% of HTLV1 positive patients and usually affects adults. These patients also have defects of cell mediated immunity and are at risk for multiple opportunistic infections (Arch Pathol Lab Med 2000;124:1241). Of note, HTLV1 infection also causes tropical spastic parapesis, a chronic progressive demyelinating disease affecting the spinal cord and CNS white matter, causing weakness and spasticity, predominantly in the lower limbs (Medscape: Human T-Cell Lymphotropic Viruses (HTLV) [Accessed 20 October 2023]).
Adult T cell leukemia / lymphoma is divided into different subtypes. The most aggressive and most common is the acute subtype (55 - 65% of patients), in which greater than 50% of cells have characteristic morphology. Patients present with generalized lymphadenopathy, hepatosplenomegaly, bone marrow infiltration and skin lesions. Patients have a high white blood count with lymphocytosis and hypercalcemia. Cutaneous infiltrates may resemble mycosis fungoides due to epidermotropism with Pautrier microabscesses. Median survival is less than 1 year. The lymphomatous subtype (20 - 25% of patients) is characterized by prominent lymphadenopathy without significant peripheral blood involvement. The chronic subtype has an increased white blood count and absolute lymphocytosis but only 10 - 50% of white blood cells are abnormal. These patients may have mild lymphadenopathy or hepatosplenomegaly but no CNS, bone or GI involvement. The smoldering subtype has 5% or more malignant cells in the peripheral blood, with a normal total lymphocyte count and no lymphadenopathy, hepatosplenomegaly or marrow infiltrates. Patients with the chronic and smoldering subtypes may evolve into the acute subtype after years of indolent disease.
Microscopically, the most distinctive feature are cells with basophilic and agranular cytoplasm and multilobated nuclei that resemble cloverleafs or flowers (cloverleaf type cell). The nuclei have thick nuclear membranes and course chromatin, with small or absent nucleoli. Reed-Sternberg-like cells may be present.
By flow cytometry or immunohistochemistry, tumor cells are positive for CD2, CD3, CD4 and CD5, as well as CD25, CD52 and HLA-DR. They are usually negative for TdT, CD7, CD8 and CD30. Molecular studies demonstrate the HTLV1 provirus in tumor cells and a clonal T cell receptor rearrangement.
At present, no curative treatment or vaccine is available. Multiagent chemotherapy can cause complete remission but relapse is common. Antibodies to CD52, called Campath-1H, are currently undergoing investigational studies (ClinicalTrials.gov: Campath-1H for Treating Adult T-Cell Leukemia / Lymphoma [Accessed 20 October 2023]).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Shylashree Chikkamuniyappa Edalur, Hematopathology fellow, University of Texas Health Science Center, San Antonio, Texas, USA.
Case #21
Clinical history:
The patient is a 64 year old Japanese woman with a history of disseminated nocardial infection, with abscesses in the brain and lung and a facial herpetic infection. A complete blood count showed a hemogloblin of 12.2, platelet count of 313 and elevated white blood cell count of 45.6 with 73% lymphocytes.
A bone marrow biopsy was hypercellular for age with 15% large, atypical cells.
Flow cytometry of peripheral blood showed bright CD45 / LCA staining with 98% T cells. 98% of the T cells marked with CD2, CD3, CD4 and CD5 and 4% marked with CD8 and CD7.
Other lab tests were calcium of 8.4 mg/dl, LDH: 452 U/L (high), HTLV1: 2+ positive by ELISA, Western Blot: bands present at p16, gp21 and gp46-1.
Peripheral blood images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Adult T cell leukemia / lymphoma
Discussion:
Adult T cell leukemia / lymphoma occurs most commonly where the HTLV1 retrovirus (human T cell leukemia virus 1) is endemic, namely in southwest Japan, western or central Africa, South America, the Caribbean and the southeast U.S. Infection is sexually transmitted or spreads from mother to child (through the placenta or breast milk), through intravenous drug abuse or blood transfusion. There is usually a delay of several decades before clinical features appear. Leukemia / lymphoma occurs in 1 - 5% of HTLV1 positive patients and usually affects adults. These patients also have defects of cell mediated immunity and are at risk for multiple opportunistic infections (Arch Pathol Lab Med 2000;124:1241). Of note, HTLV1 infection also causes tropical spastic parapesis, a chronic progressive demyelinating disease affecting the spinal cord and CNS white matter, causing weakness and spasticity, predominantly in the lower limbs (Medscape: Human T-Cell Lymphotropic Viruses (HTLV) [Accessed 20 October 2023]).
Adult T cell leukemia / lymphoma is divided into different subtypes. The most aggressive and most common is the acute subtype (55 - 65% of patients), in which greater than 50% of cells have characteristic morphology. Patients present with generalized lymphadenopathy, hepatosplenomegaly, bone marrow infiltration and skin lesions. Patients have a high white blood count with lymphocytosis and hypercalcemia. Cutaneous infiltrates may resemble mycosis fungoides due to epidermotropism with Pautrier microabscesses. Median survival is less than 1 year. The lymphomatous subtype (20 - 25% of patients) is characterized by prominent lymphadenopathy without significant peripheral blood involvement. The chronic subtype has an increased white blood count and absolute lymphocytosis but only 10 - 50% of white blood cells are abnormal. These patients may have mild lymphadenopathy or hepatosplenomegaly but no CNS, bone or GI involvement. The smoldering subtype has 5% or more malignant cells in the peripheral blood, with a normal total lymphocyte count and no lymphadenopathy, hepatosplenomegaly or marrow infiltrates. Patients with the chronic and smoldering subtypes may evolve into the acute subtype after years of indolent disease.
Microscopically, the most distinctive feature are cells with basophilic and agranular cytoplasm and multilobated nuclei that resemble cloverleafs or flowers (cloverleaf type cell). The nuclei have thick nuclear membranes and course chromatin, with small or absent nucleoli. Reed-Sternberg-like cells may be present.
By flow cytometry or immunohistochemistry, tumor cells are positive for CD2, CD3, CD4 and CD5, as well as CD25, CD52 and HLA-DR. They are usually negative for TdT, CD7, CD8 and CD30. Molecular studies demonstrate the HTLV1 provirus in tumor cells and a clonal T cell receptor rearrangement.
At present, no curative treatment or vaccine is available. Multiagent chemotherapy can cause complete remission but relapse is common. Antibodies to CD52, called Campath-1H, are currently undergoing investigational studies (ClinicalTrials.gov: Campath-1H for Treating Adult T-Cell Leukemia / Lymphoma [Accessed 20 October 2023]).
