
Home
Case
of Week Home
Jobs
Conferences
Fellowships
Books
25 March 2011 Case of the Week #200
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email
lists, click
here.
All cases are archived on our website. To view them sorted by number, diagnosis or category,
visit our Home Page and click on the Case of the Week button on the left hand side.
Thanks to Dr. Mohammed Sami Saeed, University of Mosul (Iraq), for contributing this case.
This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.


July 11-15, 2011
The Snow King Resort
Jackson, Wyoming (USA)
The 28th Annual Summer Update
in Clinical Immunology, Microbiology
and Infectious Disease
Course Topics:
This 24-hour review and update is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory including selection and interpretation of results.
This course will provide a forum for the exchange of ideas dealing with microbial infections as well as immunity to infectious diseases and immunologic disorders. Faculty consists of clinicians involved in patient care, pathologists, and clinical laboratory scientists. Discussion of timely topics by faculty and participants assures that this course will be informative, interesting, and relevant.
Course Directors:
Harry R. Hill MD, Larry G. Reimer MD, July Daly PhD
This course is approved for 24 AMA PRA Category I Credit(s)
Website
Schedule
Hotel
Register
[#2506]
Website news:
(1) We have posted two new articles on our Management Page, Dj vu all Over Again, by Mick Raich, Vachette Pathology, click here and Stories That Will Curl Your Hair Or Close To It!, by Michelle Miller, Vachette Pathology, click here.
(2) Per the suggestion of Dr. Thomas Dudley, we are now soliciting your "best practices" related to pathology. We will post them on a new Best Practices page, organized in a logical way, with a link from our website. We anticipate that this feature will be widely read. Email your pathology best practices to NatPernick@hotmail.com.
(3) Our jobs page now lists jobs by specialty, beginning March 1, 2011. The specialty "tags" are based on the content of the ad - please be aware that most jobs only describe the position in general - you may need cytopathology experience even if not indicated in the ad. The links are after "other countries" near the top of the page.
Case of the Week #200
Clinical History
A 2 month old girl presented with an ulcerated chest wall nodule. Two weeks later, she developed a neck nodule.
The chest wall nodule measured 1.3 x 1.0 cm, and had a hemorrhagic cut surface.
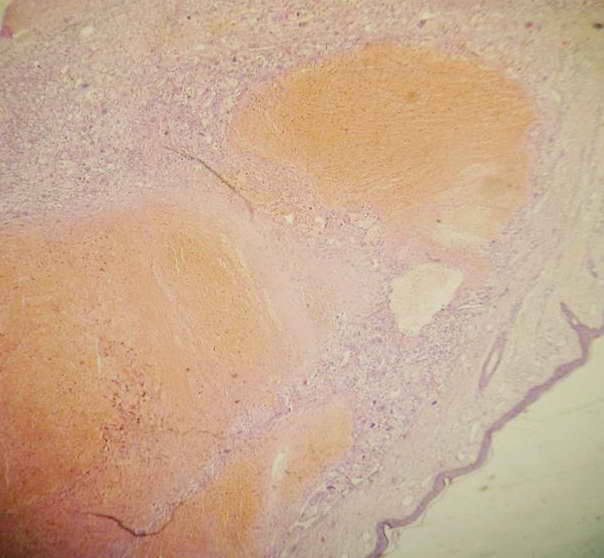
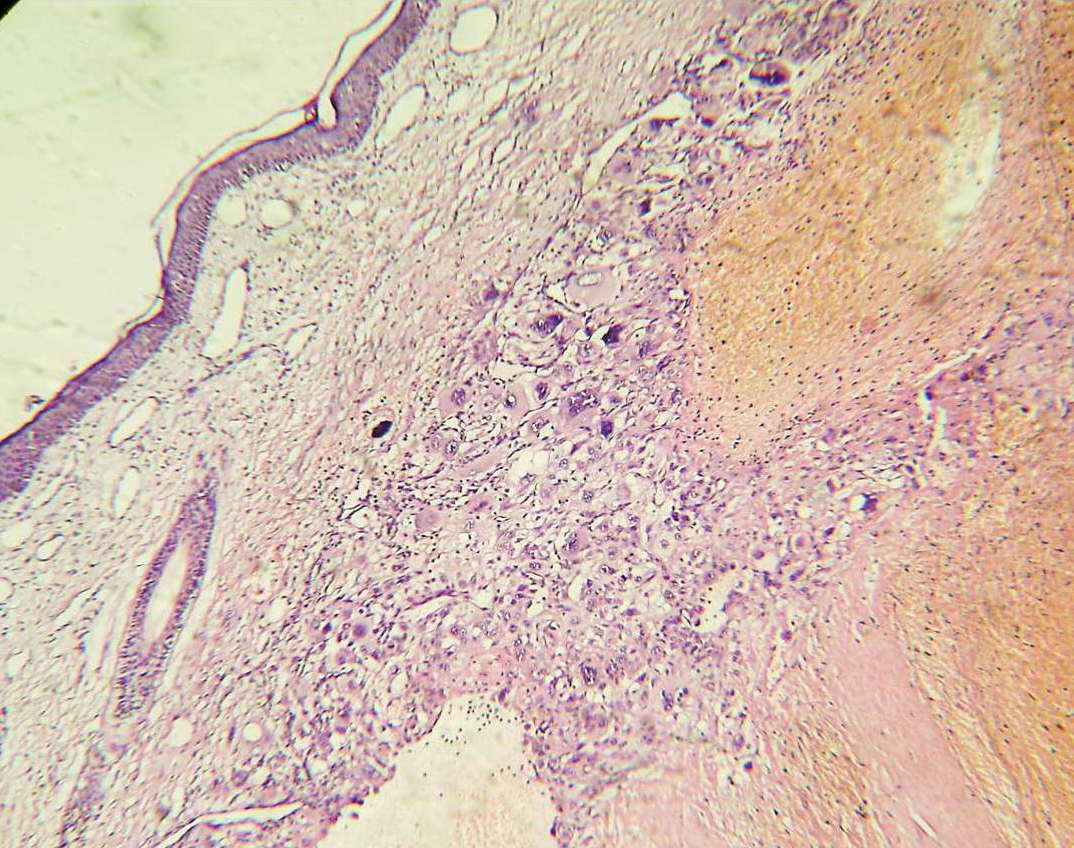
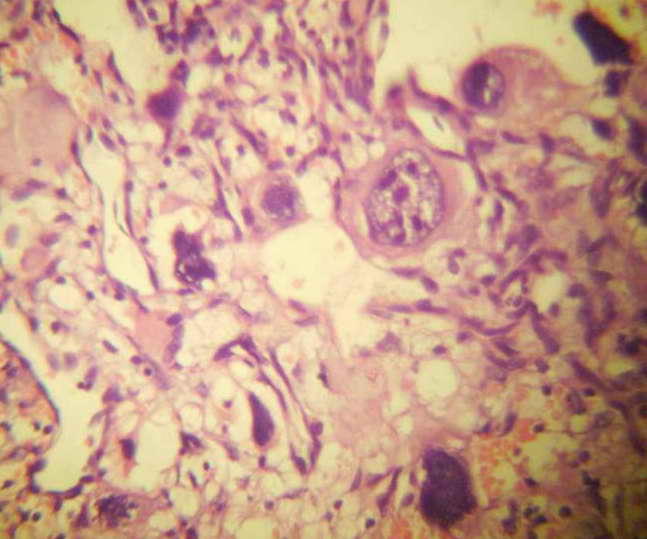
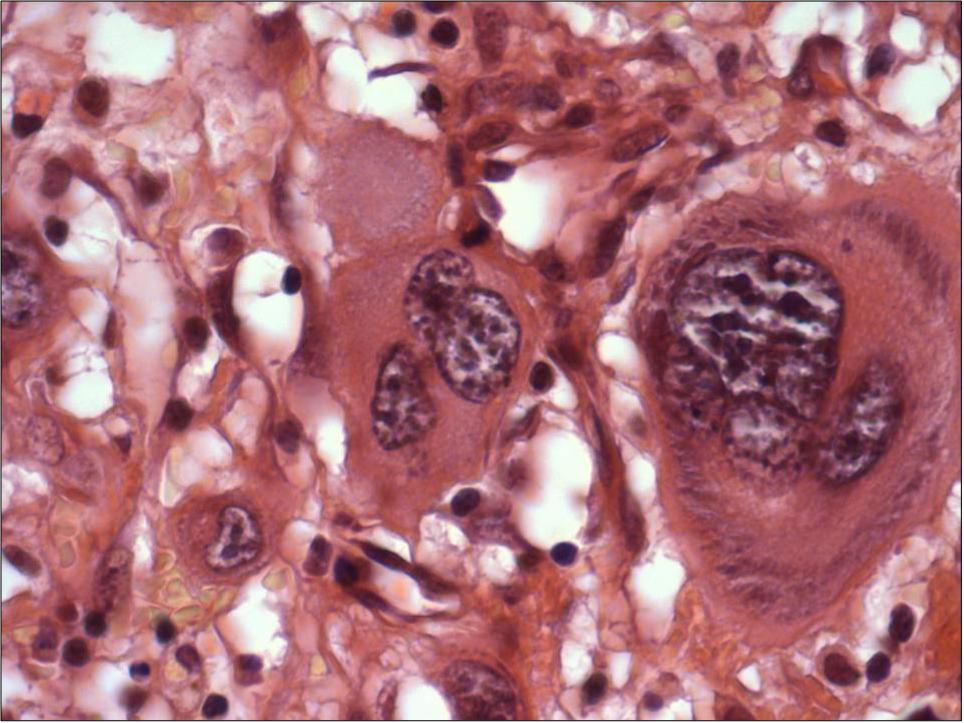
Micro images:
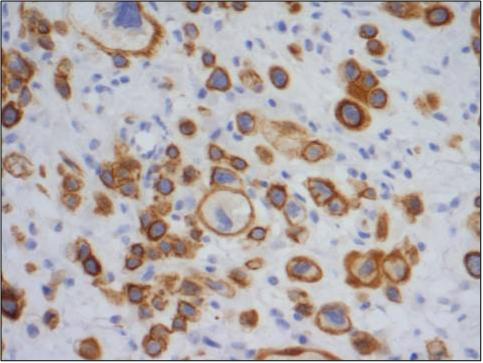

CAM5.2 and pan cytokeratin
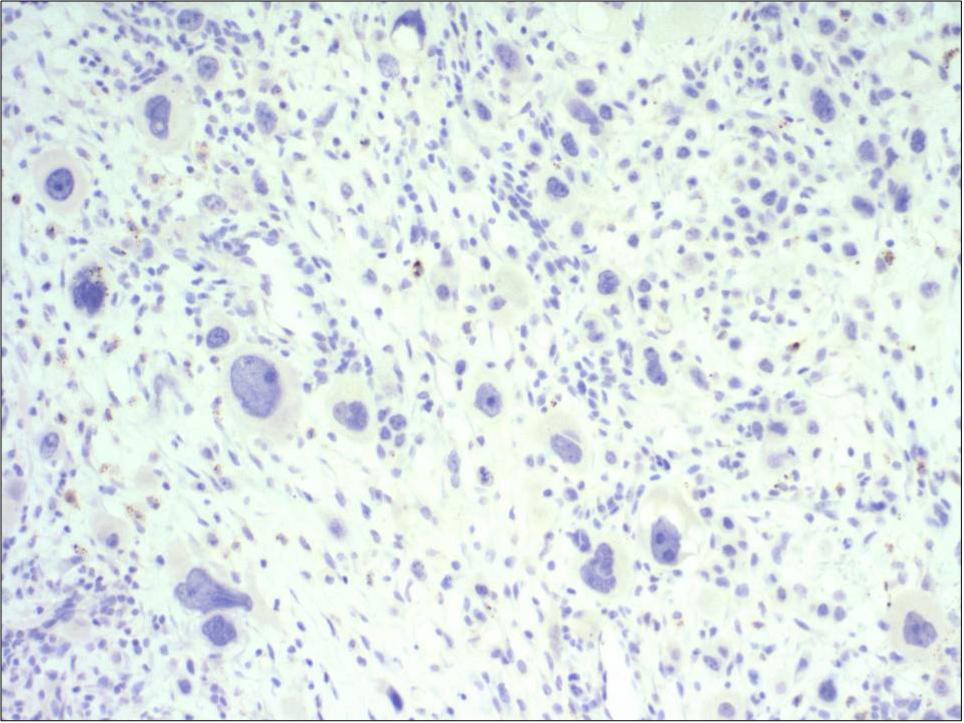
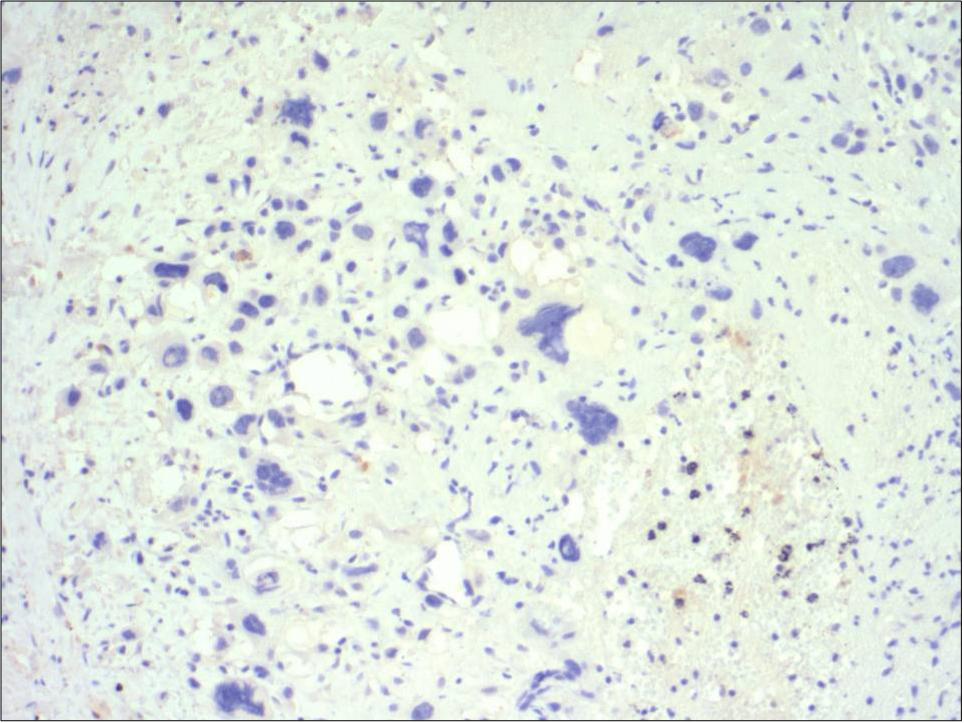
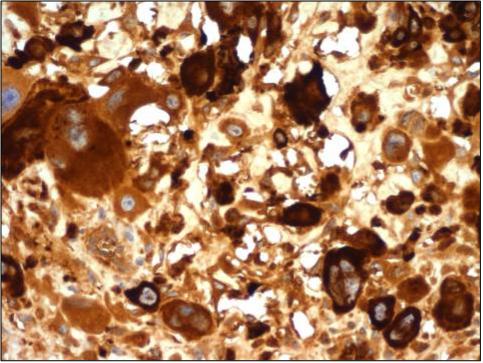
Desmin, myoglobin and hCG
What is your diagnosis?
Diagnosis:
Choriocarcinoma, metastatic, most likely from placental primary
Discussion:
Microscopic sections show a cellular tumor composed of large cells with clear or eosinophilic cytoplasm and bizarre, hyperchromatic and multiple nuclei. These cells, representing syncytiotrophoblasts, are mixed with cytotrophoblast-type cells. There are numerous mitotic figures, some atypical. Large foci of hemorrhage are identified. The bizarre tumor cells are immunoreactive for CAM5.2, pan-cytokeratin and hCG, and negative for desmin and myoglobin.
Infantile choriocarcinoma is very rare, and is presumed to be due to placental choriocarcinoma (Arch Pediatr 2005;12:1721). The mothers usually have a normal pregnancy and no history of gestational trophoblastic disease (Pediatr Dev Pathol 1998;1:380). The placenta usually appears grossly normal, and the area of tumor resembles a placental infarct (Fetal Pediatr Pathol 2005;24:21, J Radiol 2008;89:517).
Clinically, there usually are maternal metastases at diagnosis, but neonatal metastases of placental choriocarcinoma are rare (Gynecol Oncol 2006;103:1147). The clinical diagnosis is based on high maternal and pediatric serum or urinary levels of hCG or beta-hCG.
The histologic differential diagnosis includes anaplastic rhabdomyosarcoma (a variant of pleomorphic rhabdomyosarcoma, no placental findings, no cytotrophoblasts, positive for muscle markers, negative for hCG), or a metastatic testicular or ovarian germ cell tumor, which could be pure choriocarcinoma or have a choriocarcinomatous component. Although carcinomas may also have syncytiotrophoblastic components, they are unlikely in infants.
Without prompt treatment, infantile choriocarcinoma is highly fatal (Eur J Pediatr 2004;163:1). Treatment consists of aggressive chemotherapeutic regimens. Patients are often cured if the disease is treated early. In this case, the patient was severely ill, and no further studies were performed. Permission for an autopsy was denied. No information was available about the mother.
Nat Pernick, M.D., President
and Liz Parker, B.A., Associate Medical Editor
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email:
NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com