
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Tim Bracey, Royal Cornwall Hospital (U.K.), for contributing this case.

Orchard Pathology is an all-inclusive CP/AP diagnostic information system designed to accommodate the complex workflow and reporting of clinical, cytology, anatomic, and molecular testing.
Orchard Pathology is used for AP only or as a single system that includes clinical and molecularno more need for two separate systems. The shared database provides access to the patients history and enables the consolidation of clinical results to the pathology report. Unlike legacy text-based AP systems, Orchard Pathology stores report information in structured data fields that enhance EMR integration and simplify data mining for evaluations; correlation studies; quality assurance; and other management reports.
Visit us at
http://www.OrchardSoft.com.
(1) We have updated the Molecular Pathology chapter with a section on DNA sequencing written by Rodney E. Shackelford, D.O., Ph.D., Tulane University, Louisiana.
(2) We have extensively updated the CD Markers CD1-CD49 chapter, which now has 68 topics, 479 images and 1092 references.
(3) For a "printer friendly page" of any part of our website, we recommend visiting http://www.printfriendly.com, which has options to print with or without images. As this works better than our "printer friendly" versions of chapters, we will remove the printer friendly versions as we update chapters.
Visit and follow our Blog to see recent updates to the website.
Case #197
Clinical history:
An 85 year old woman was admitted with shortness of breath and chest pain. She had been given a diagnosis of inoperable lung cancer several years previously on the basis of multiple lung nodules on chest Xray.
The postmortem examination revealed an acute myocardial infarction involving the posterior mitral valve papillary muscle and multiple waxy yellow-brown pulmonary nodules. A fine needle aspiration of the lung nodule was obtained, and stained with the Romanowsky method.
Microscopic images:
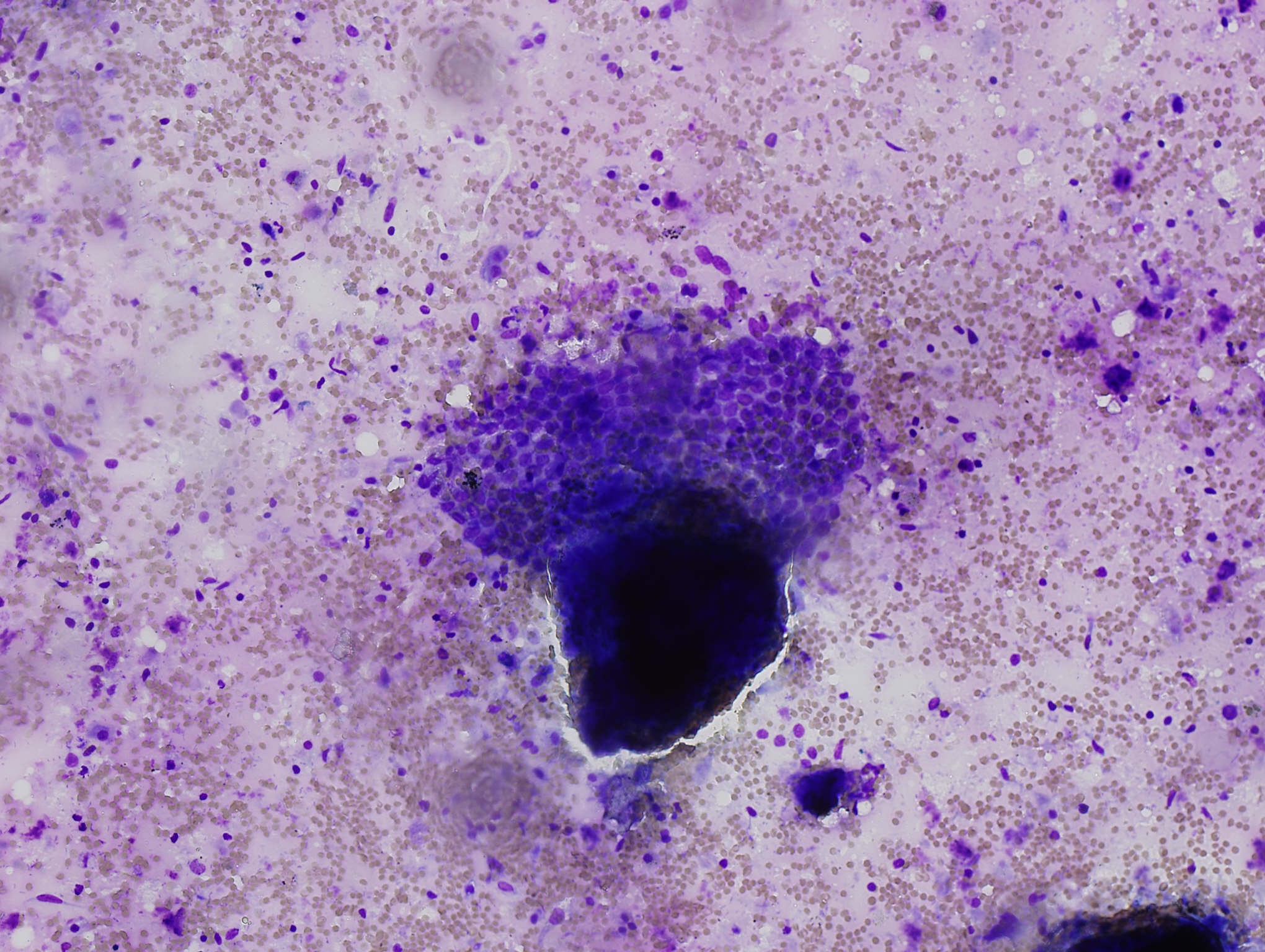

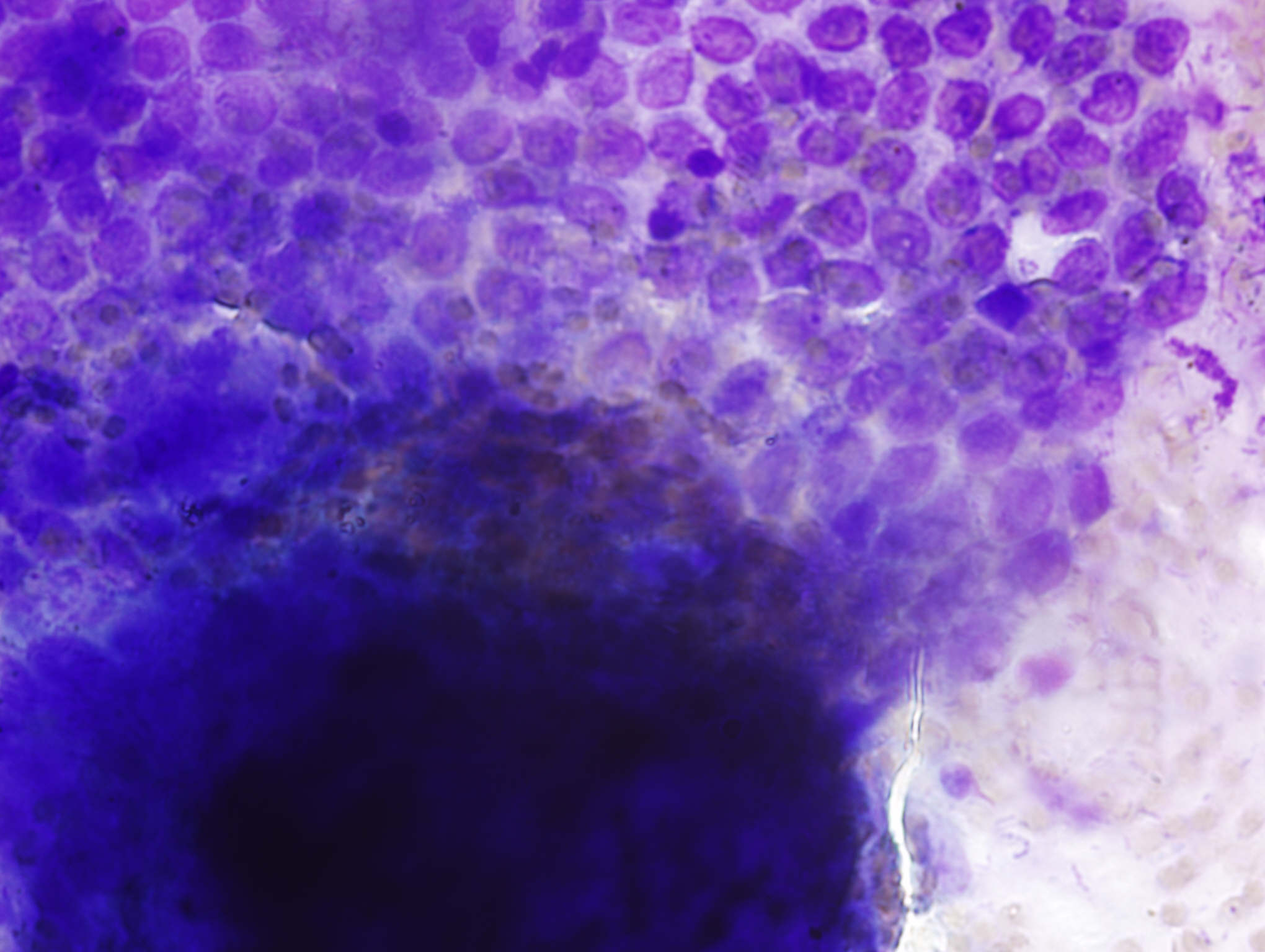
Fine needle aspiration of lung nodule
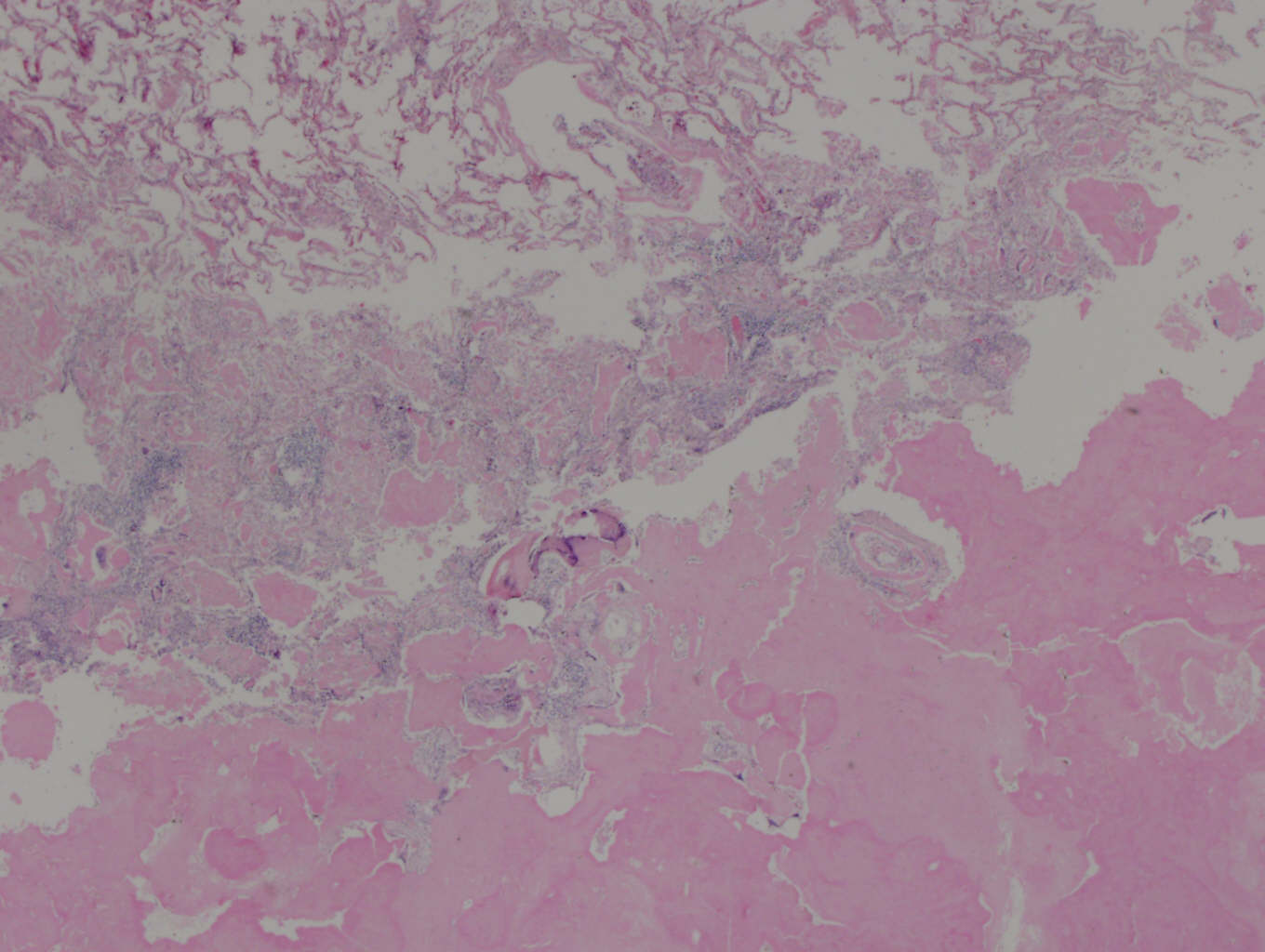
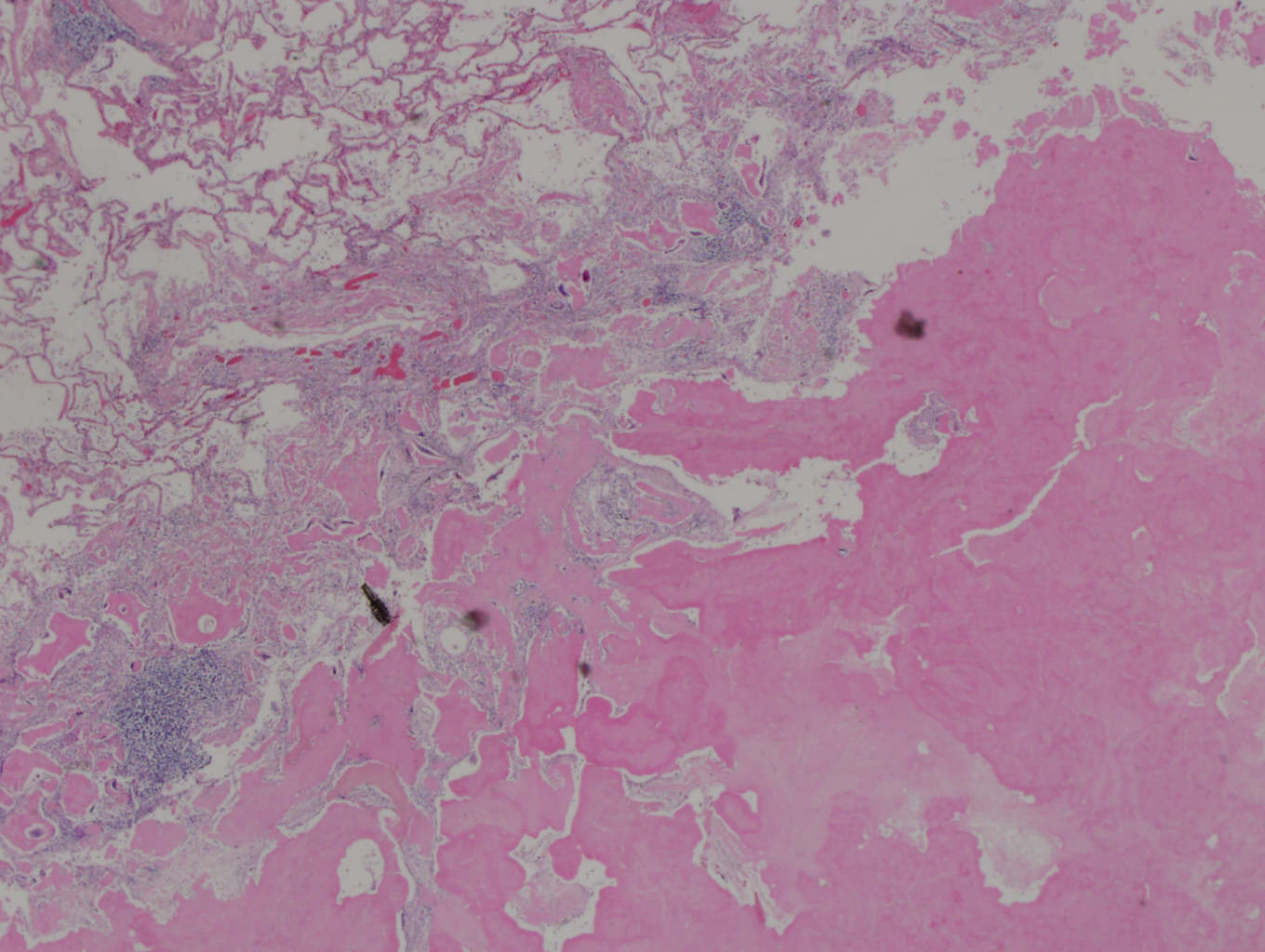
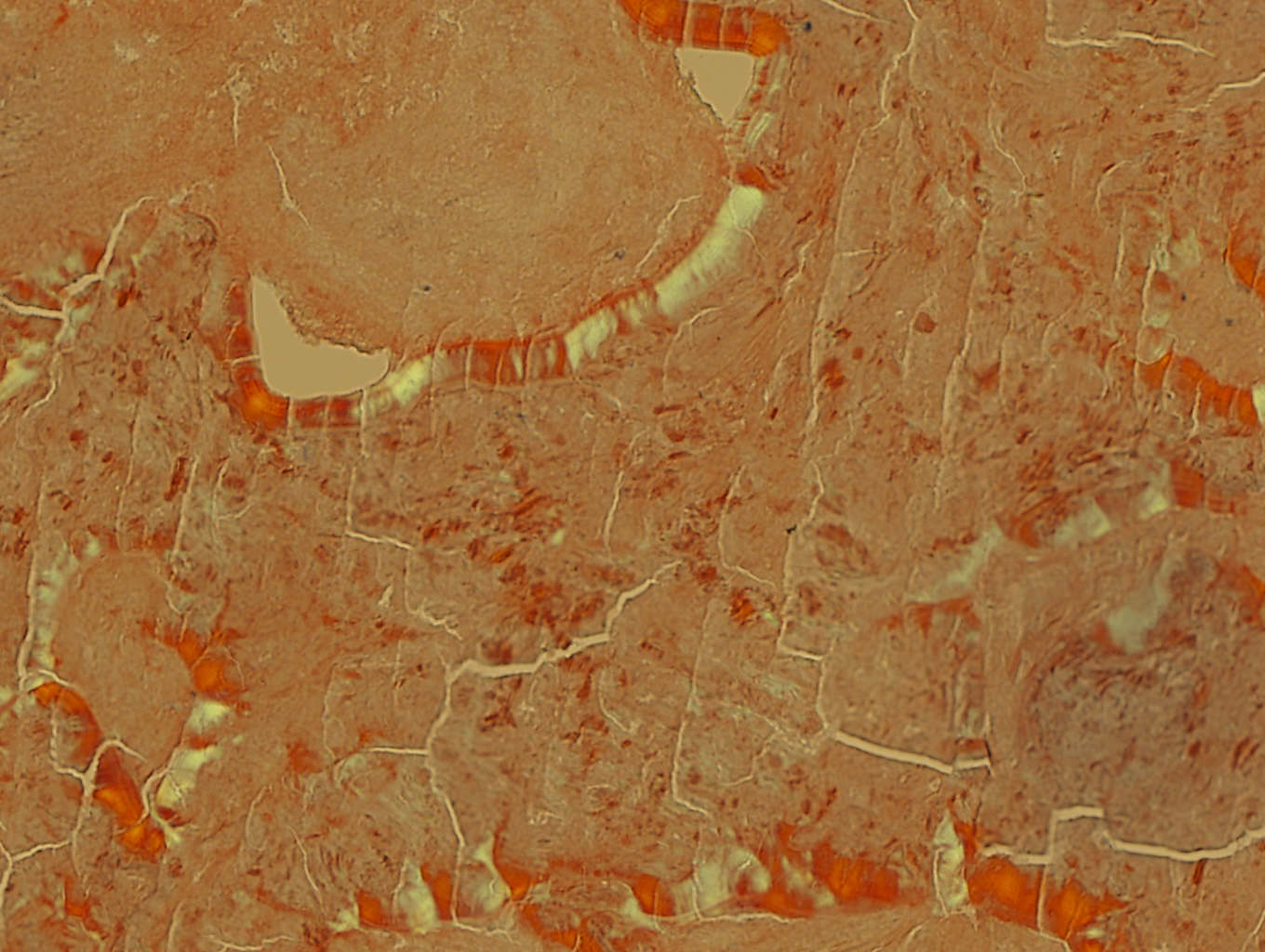
Lung nodules, H&E
What is your diagnosis?
Diagnosis: Nodular pulmonary amyloidosis
Immunostains:
Discussion:
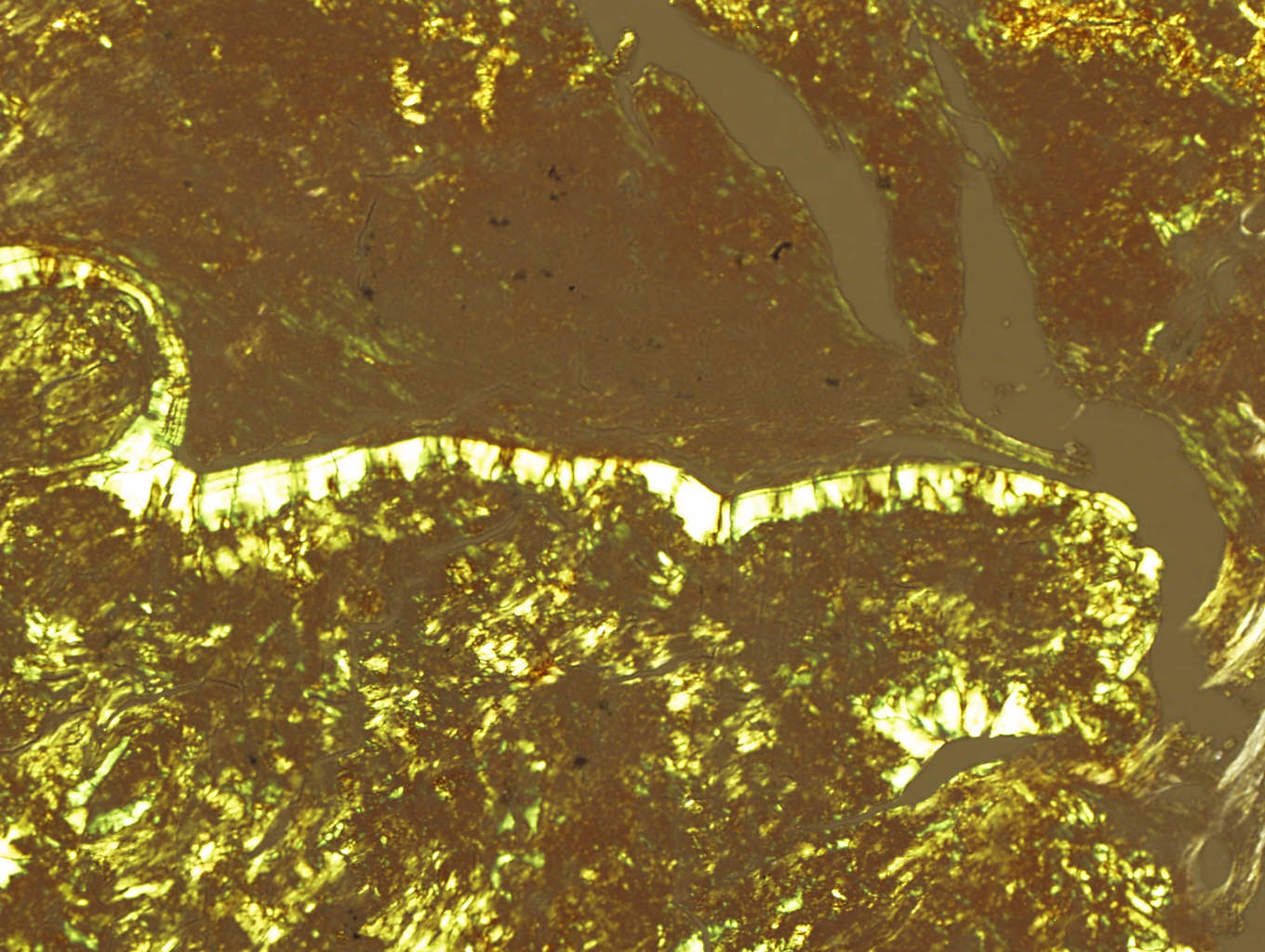
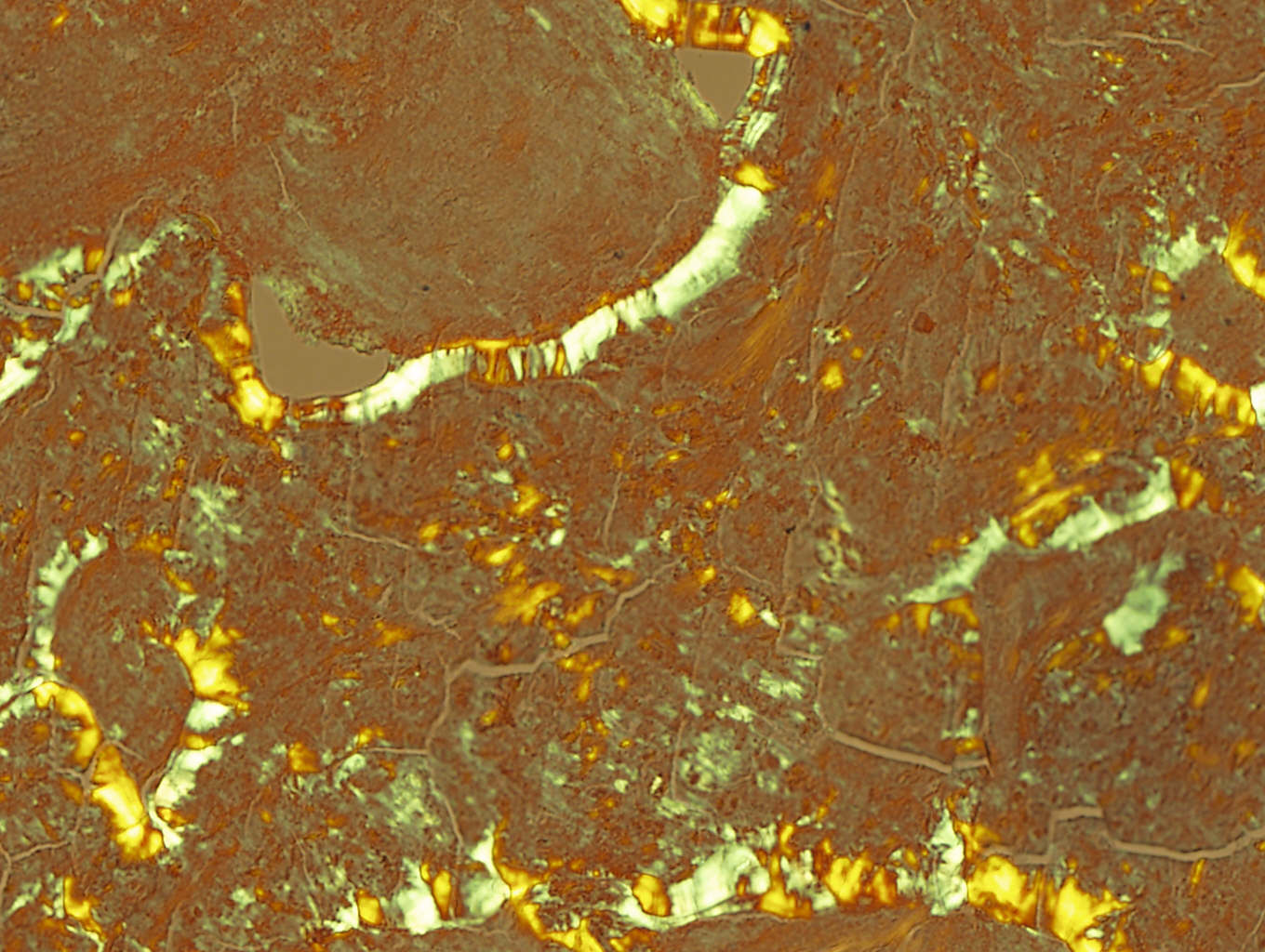
The fine needle aspirate showed a honeycomb arrangement of benign bronchial epithelial cells next to amorphous material. Sections with Congo red staining and polarized microscopy show colloid cracking and apple-green bifrefringence of the amorphous material, diagnostic of amyloid deposition.
Pulmonary amyloid often presents in an asymptomatic elderly patient with a nodule on chest Xray but no evidence of systemic disease. It may be due to a chronic inflammatory condition (TB, HIV, connective tissue disorder) or be associated with a plasma cell dyscrasia or lymphoproliferative disorder.
Pulmonary amyloid can be divided into 4 categories: vascular (not a serious clinical problem), nodular bronchial, nodular parenchymal or diffuse alveolar septal. The nodular types can have multiple lesions and may simulate malignancy, as in this case. Diffuse alveolar septal cases may cause severe pulmonary impairment with a poor prognosis. In all categories, the amyloid material is usually composed of AL type protein.
Histologically, the nodules are usually well circumscribed, with amorphous pink amyloid material. T cells, plasma cells and granulomatous inflammation are common. Calcification and ossification are also common.
The differential diagnosis includes marginal zone lymphoma / MALT or SLL with amyloid production as well as hyalinizing granuloma (no amyloid is actually present) (Mod Pathol 2000;13:934). Amyloid-like pulmonary nodules have been described with and without systemic light chain disease (Am J Clin Pathol 2004;121:200). Electron microscopy shows dense granular extracellular deposits but without the fibrillary characteristics of amyloid.
Patients with nodular amyloid, as in this case, typically have a good clinical course. Although treatment of associated conditions may be indicated, the amyloid nodules are typically indolent.
