
26 January 2011 - Case #195
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. David Cohen, Herzliya Medical Center, Israel for contributing this case.
Case #195
Clinical history:
A 40 year old woman presented with a bladder tumor and had a TURBT.
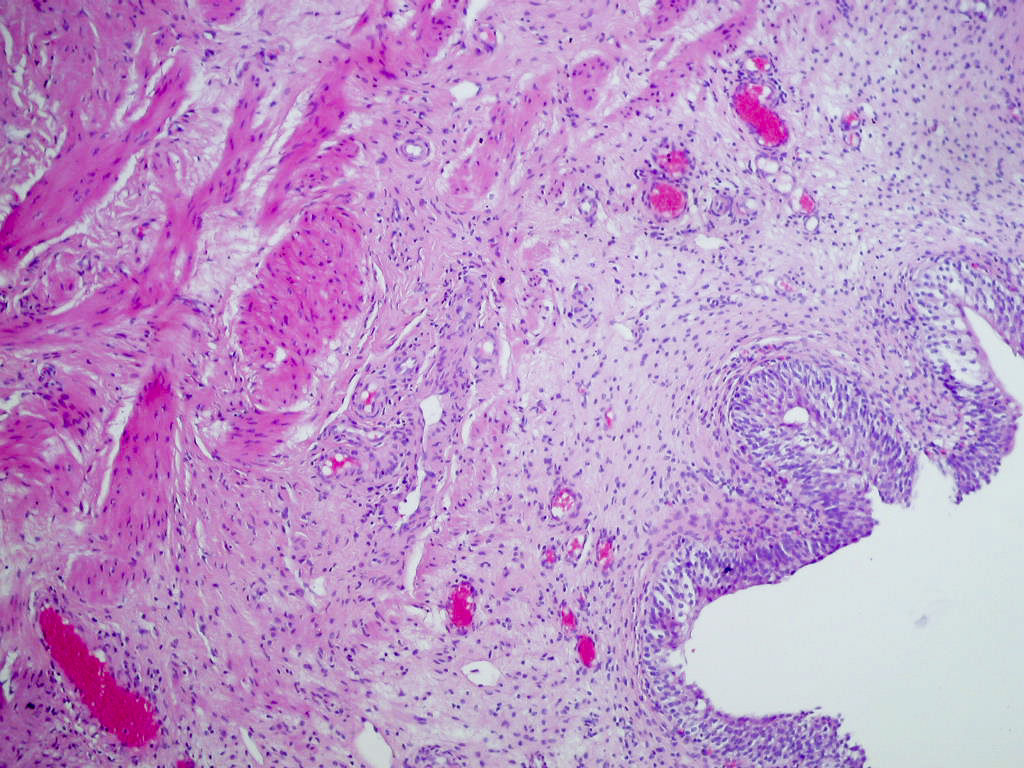
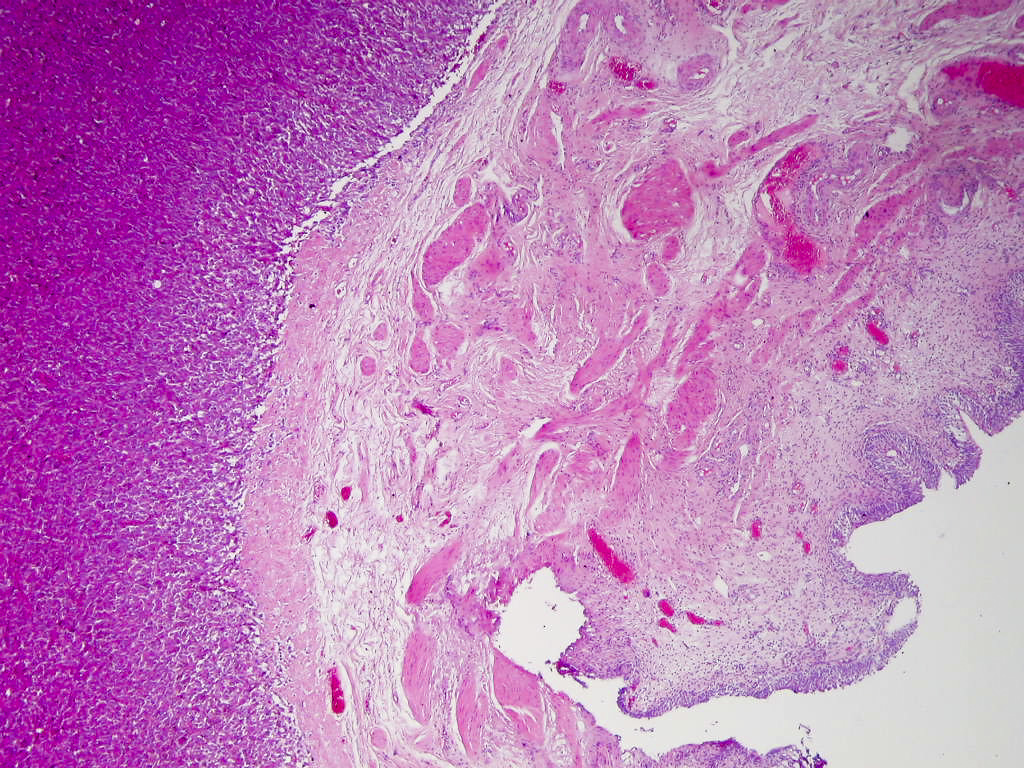
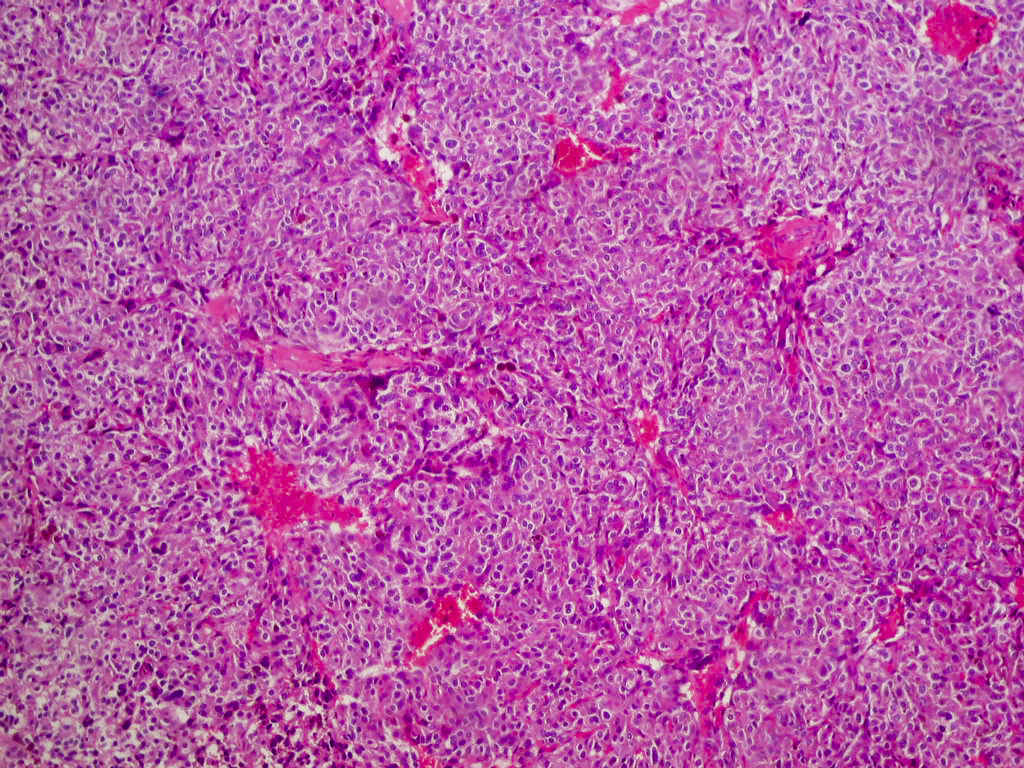
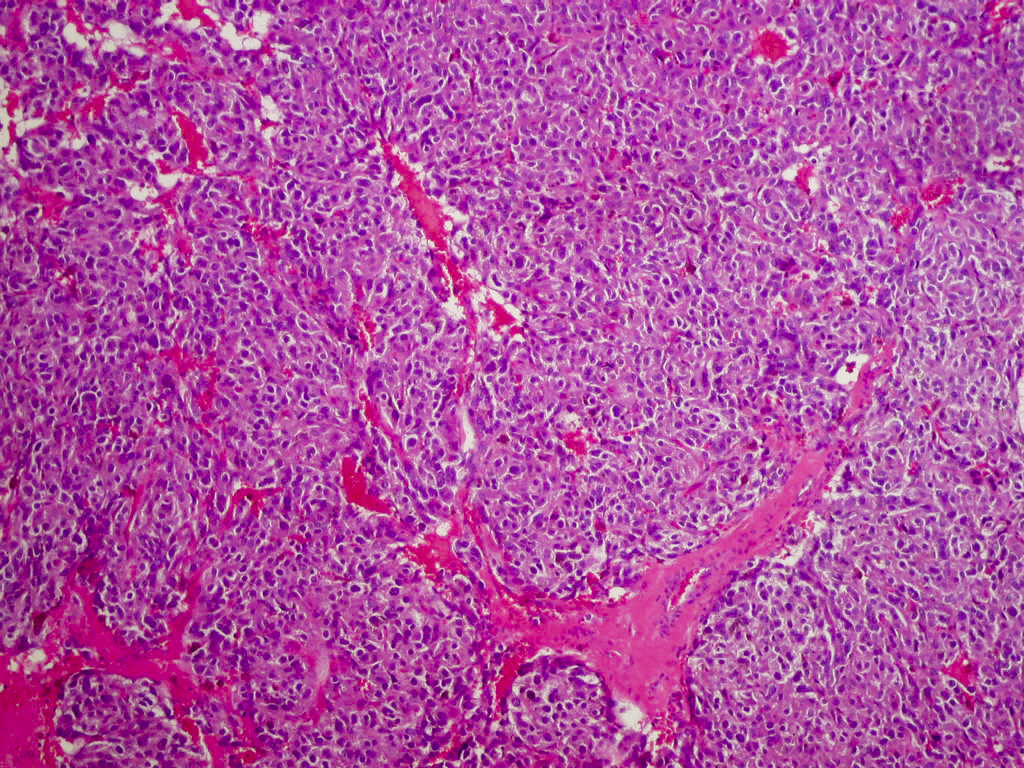
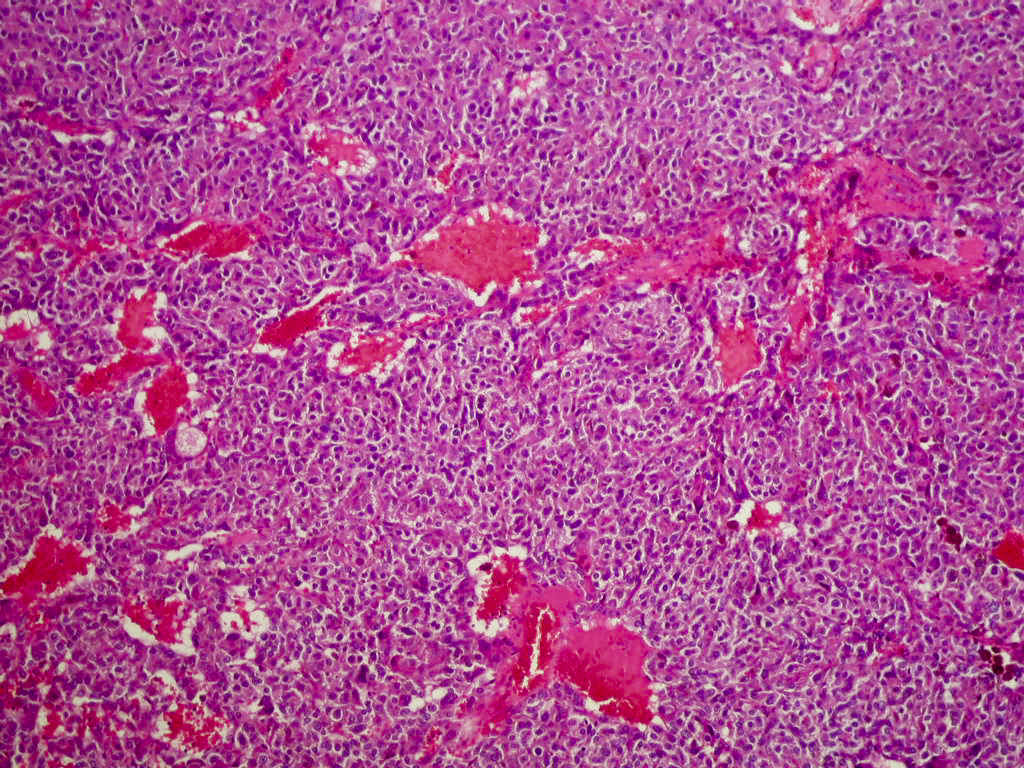
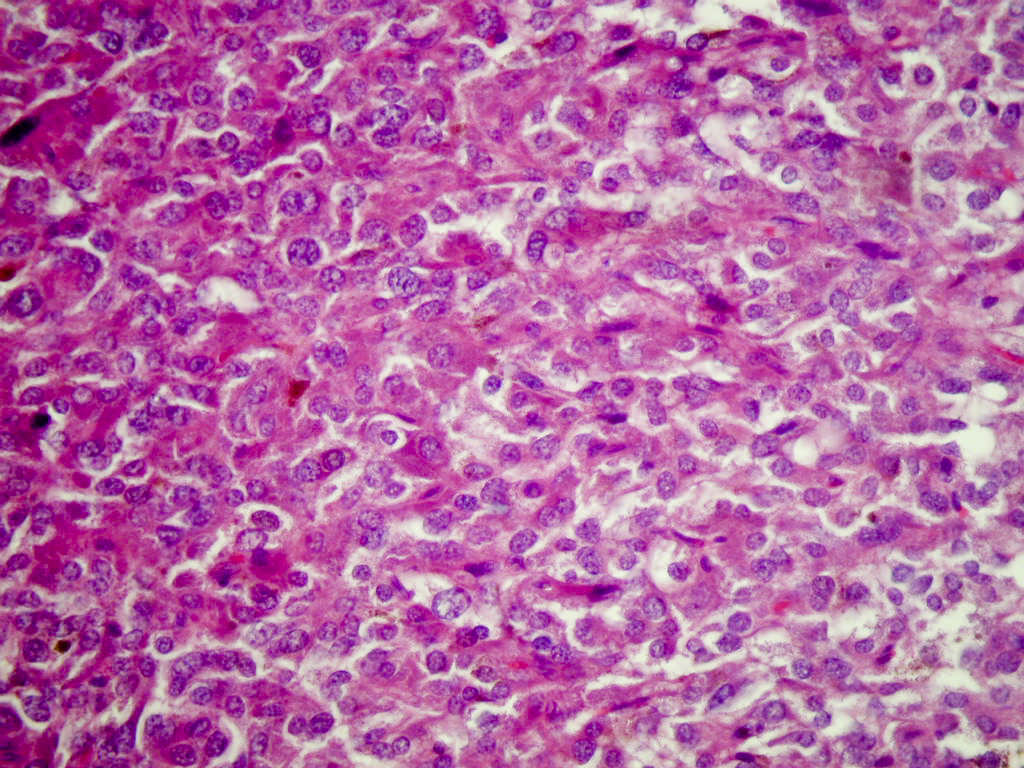
Microscopic images:

What is your diagnosis?
Diagnosis: Paraganglioma of bladder
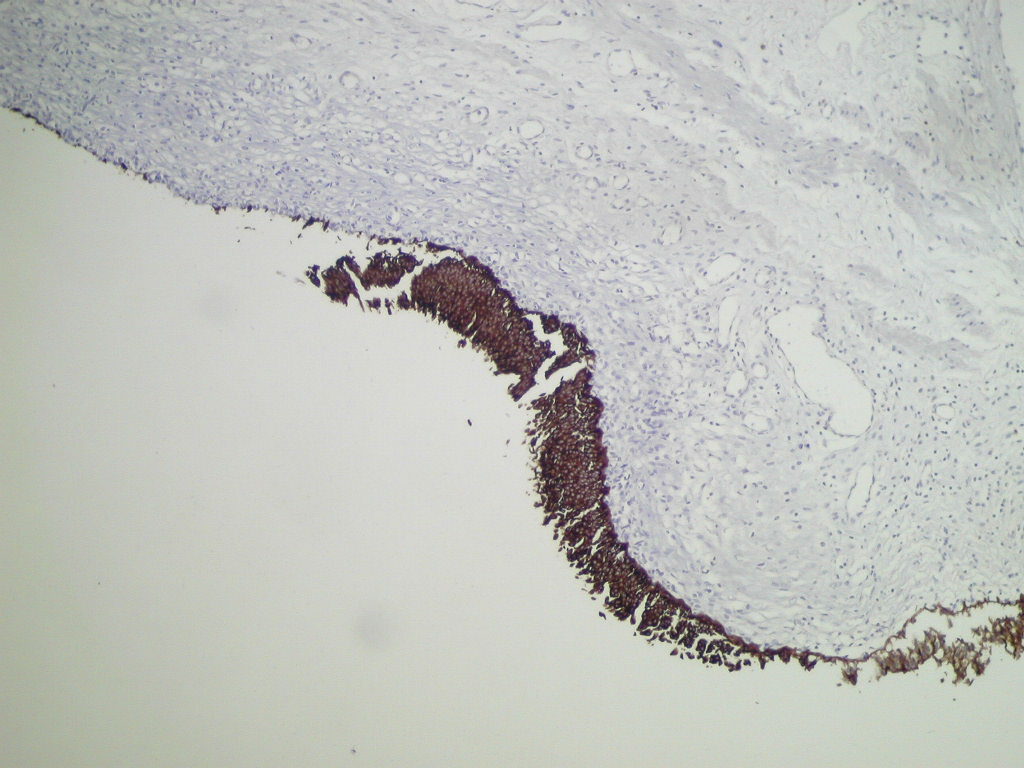
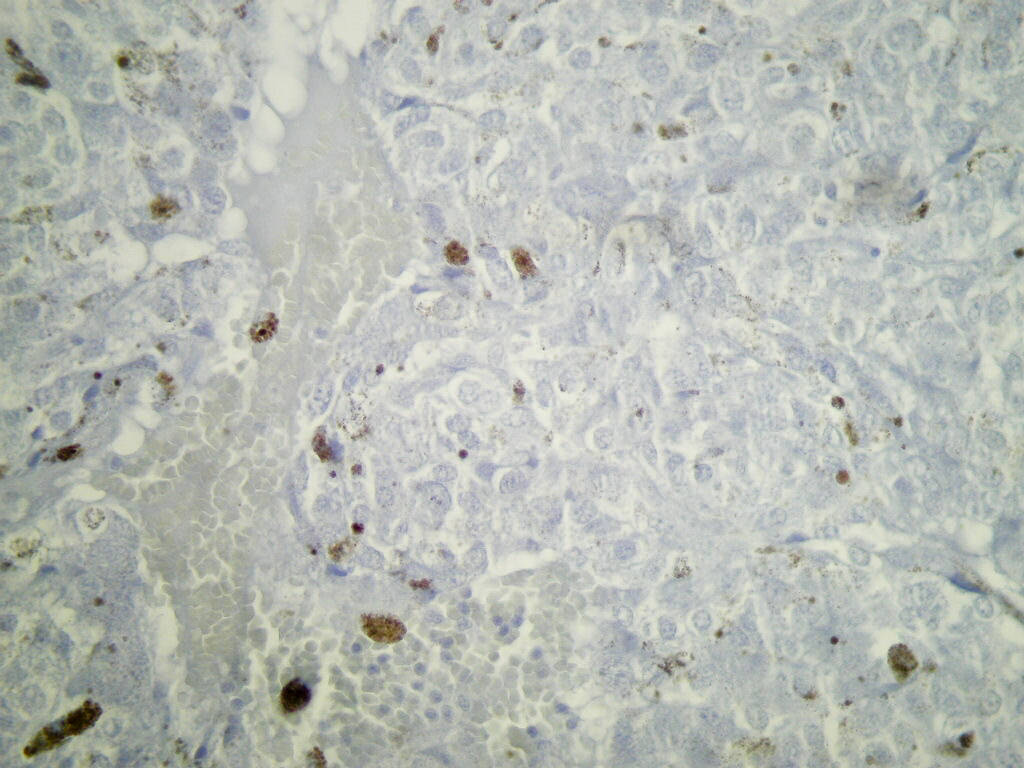
Immunostains:


Discussion:
The microscopic sections show a tissue mass with adjacent benign urothelium, lamina propria and muscularis propria. The mass contains occasional nests of cells (zellballen pattern) but primarily sheets of large, pleomorphic malignant cells with a vascular stroma. The tumor cells have abundant cytoplasm with brown melanin pigment and large vesicular nuclei but no prominent nucleoli and only rare mitotic figures. Immunostaining shows scattered staining for S100 protein but no HMB45 staining. There is also strong staining for chromogranin A and synaptophysin. Ki67 staining (not shown) revealed nuclear staining of 5% of tumor cells.
Paraganglioma, also called extra-adrenal pheochromocytoma, is uncommon in the bladder. It typically affects young women (median age 44 years), in contrast to urothelial carcinoma, which has a median age of 70 years.
Tumors have the classic zellballen pattern or diffuse patterns of large polygonal cells with abundant eosinophilic granular cytolasm. The nuclei are usually fairly uniform, and a delicate fibrovascular stroma is usually present. Although there may be involvement of muscularis propria, there is usually no desmoplasia. Melanin pigmentation is rare but does not appear to affect prognosis (Cancer 1997;79:398).
The differential diagnosis includes:
Treatment consists of excision (partial cystectomy). Tumors may recur or metastasize in 5 - 15%, although these cases often cannot be predicted.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. David Cohen, Herzliya Medical Center, Israel for contributing this case.
Website news:
(1) For a "printer friendly page" of any part of our website, we recommend visiting http://www.printfriendly.com, which has options to print with or without images. As this works better than the "printer friendly" versions of chapters that we created, we will remove the printer friendly versions as we update each chapter.
(2) We have about 15 pending Cases of the Week, so the next cases received and accepted should be posted within 6 - 7 months.
(3) Thanks for your support. In 2010, we had 2,999,616 visits, or over 88 million hits.
Visit and follow our Blog to see recent updates to the website.
(1) For a "printer friendly page" of any part of our website, we recommend visiting http://www.printfriendly.com, which has options to print with or without images. As this works better than the "printer friendly" versions of chapters that we created, we will remove the printer friendly versions as we update each chapter.
(2) We have about 15 pending Cases of the Week, so the next cases received and accepted should be posted within 6 - 7 months.
(3) Thanks for your support. In 2010, we had 2,999,616 visits, or over 88 million hits.
Visit and follow our Blog to see recent updates to the website.
Case #195
Clinical history:
A 40 year old woman presented with a bladder tumor and had a TURBT.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Paraganglioma of bladder
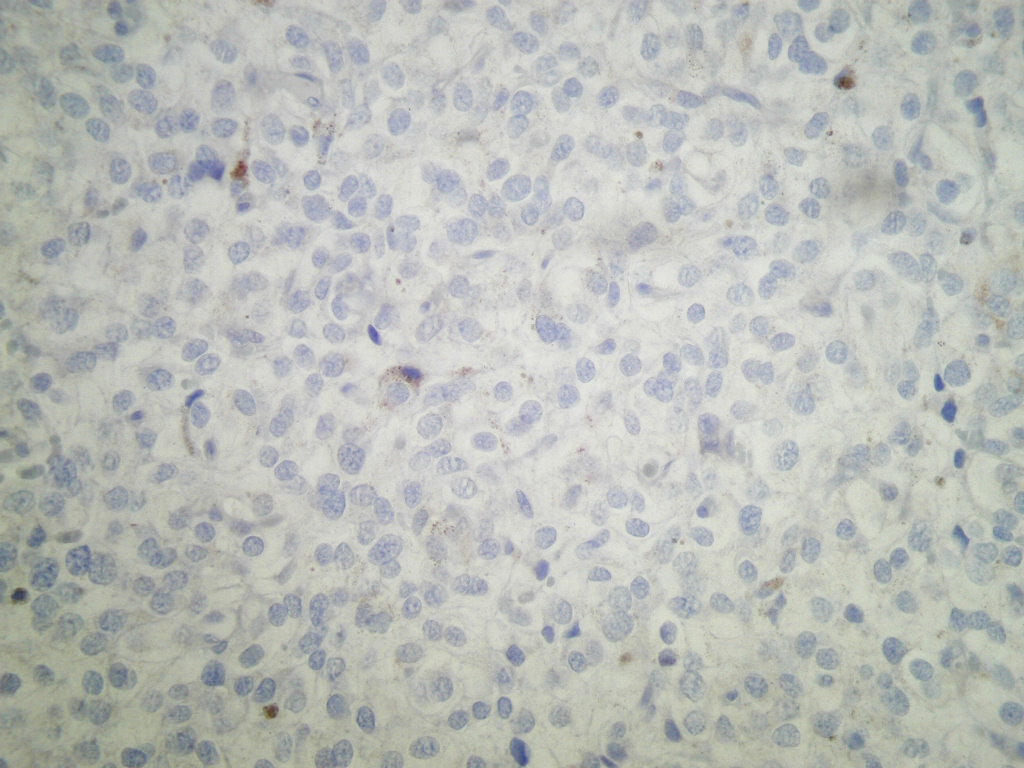
Immunostains:
Cytokeratin staining
S100 and HMB45 staining
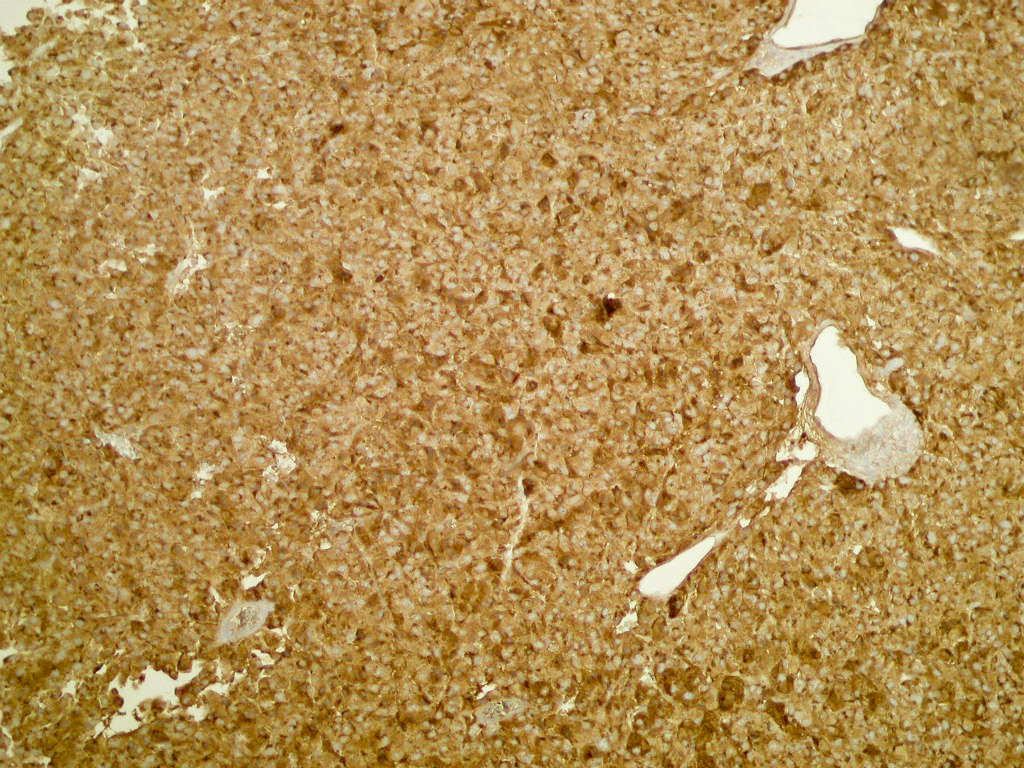
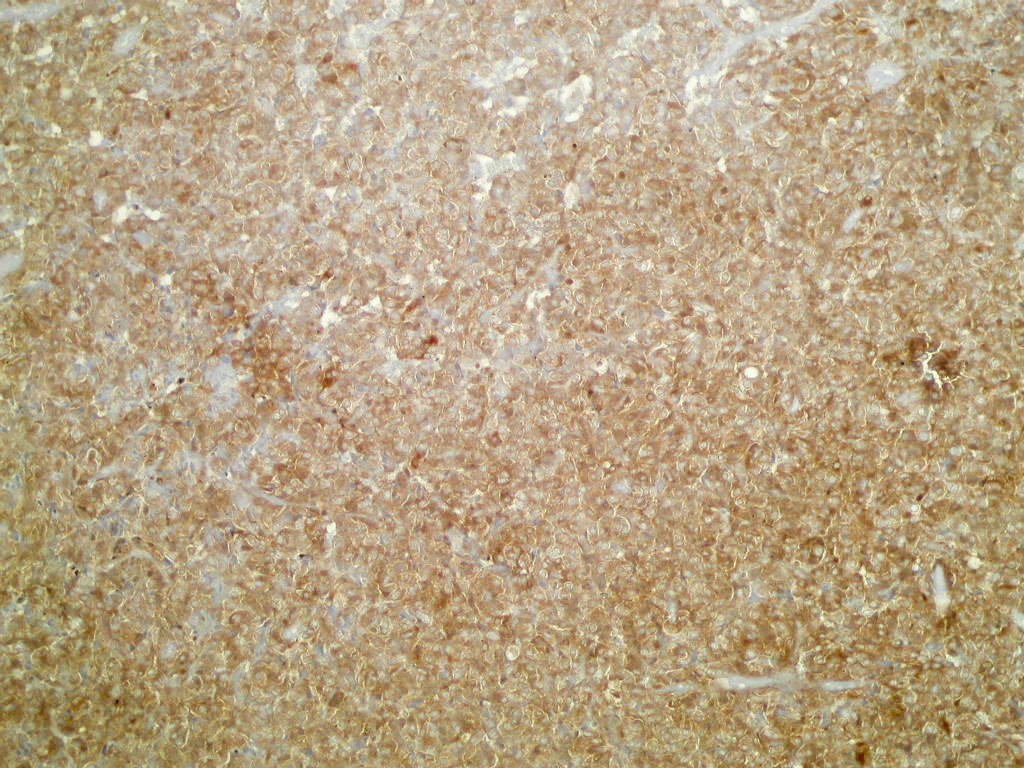
Chromogranin, synaptophysin and NSE staining
Discussion:
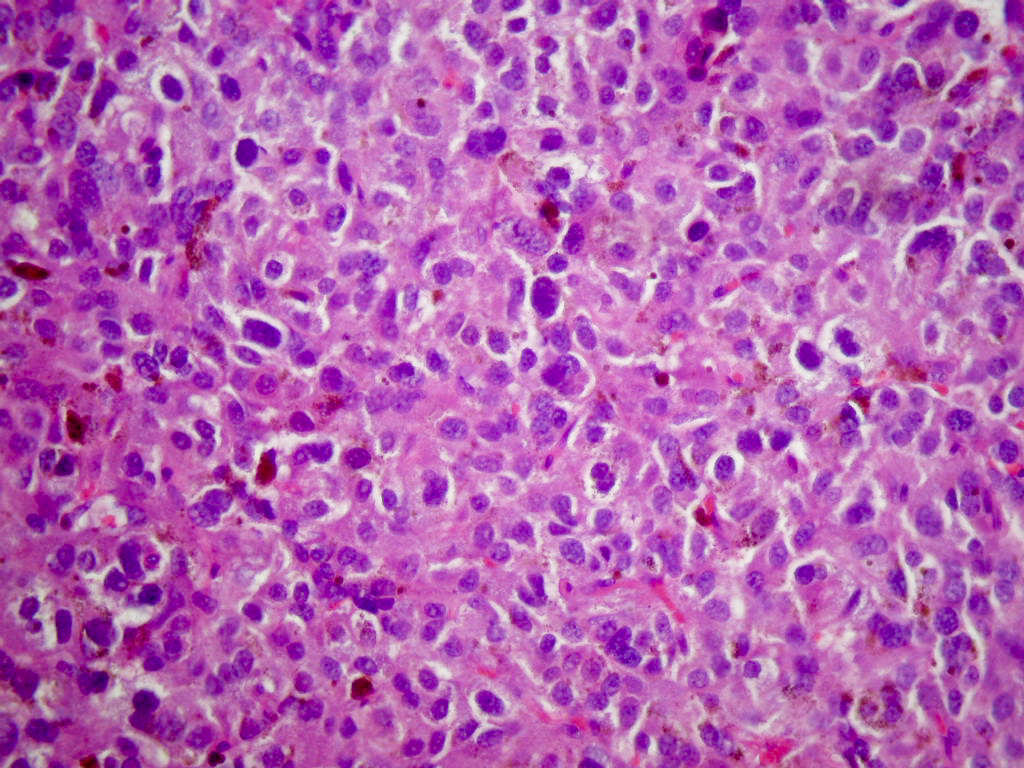
The microscopic sections show a tissue mass with adjacent benign urothelium, lamina propria and muscularis propria. The mass contains occasional nests of cells (zellballen pattern) but primarily sheets of large, pleomorphic malignant cells with a vascular stroma. The tumor cells have abundant cytoplasm with brown melanin pigment and large vesicular nuclei but no prominent nucleoli and only rare mitotic figures. Immunostaining shows scattered staining for S100 protein but no HMB45 staining. There is also strong staining for chromogranin A and synaptophysin. Ki67 staining (not shown) revealed nuclear staining of 5% of tumor cells.
Paraganglioma, also called extra-adrenal pheochromocytoma, is uncommon in the bladder. It typically affects young women (median age 44 years), in contrast to urothelial carcinoma, which has a median age of 70 years.
Tumors have the classic zellballen pattern or diffuse patterns of large polygonal cells with abundant eosinophilic granular cytolasm. The nuclei are usually fairly uniform, and a delicate fibrovascular stroma is usually present. Although there may be involvement of muscularis propria, there is usually no desmoplasia. Melanin pigmentation is rare but does not appear to affect prognosis (Cancer 1997;79:398).
The differential diagnosis includes:
- Carcinoid tumor: may have nesting pattern but is keratin+
- Urothelial carcinoma: usually older patients, much more common, usually more pleomorphism, also keratin+ (Am J Surg Pathol 2004;28:94)
- Melanoma: the great imitator may have a focal nesting pattern but has prominent mitotic figures; it is usually strongly S100+ and HMB45+, and negative for neuroendocrine markers
Treatment consists of excision (partial cystectomy). Tumors may recur or metastasize in 5 - 15%, although these cases often cannot be predicted.
