
3 November 2010 - Case #189
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Elaine Alt, Quest Diagnostics, New Jersey (USA) for contributing this case.
Advertisement
Case #189
Clinical history:
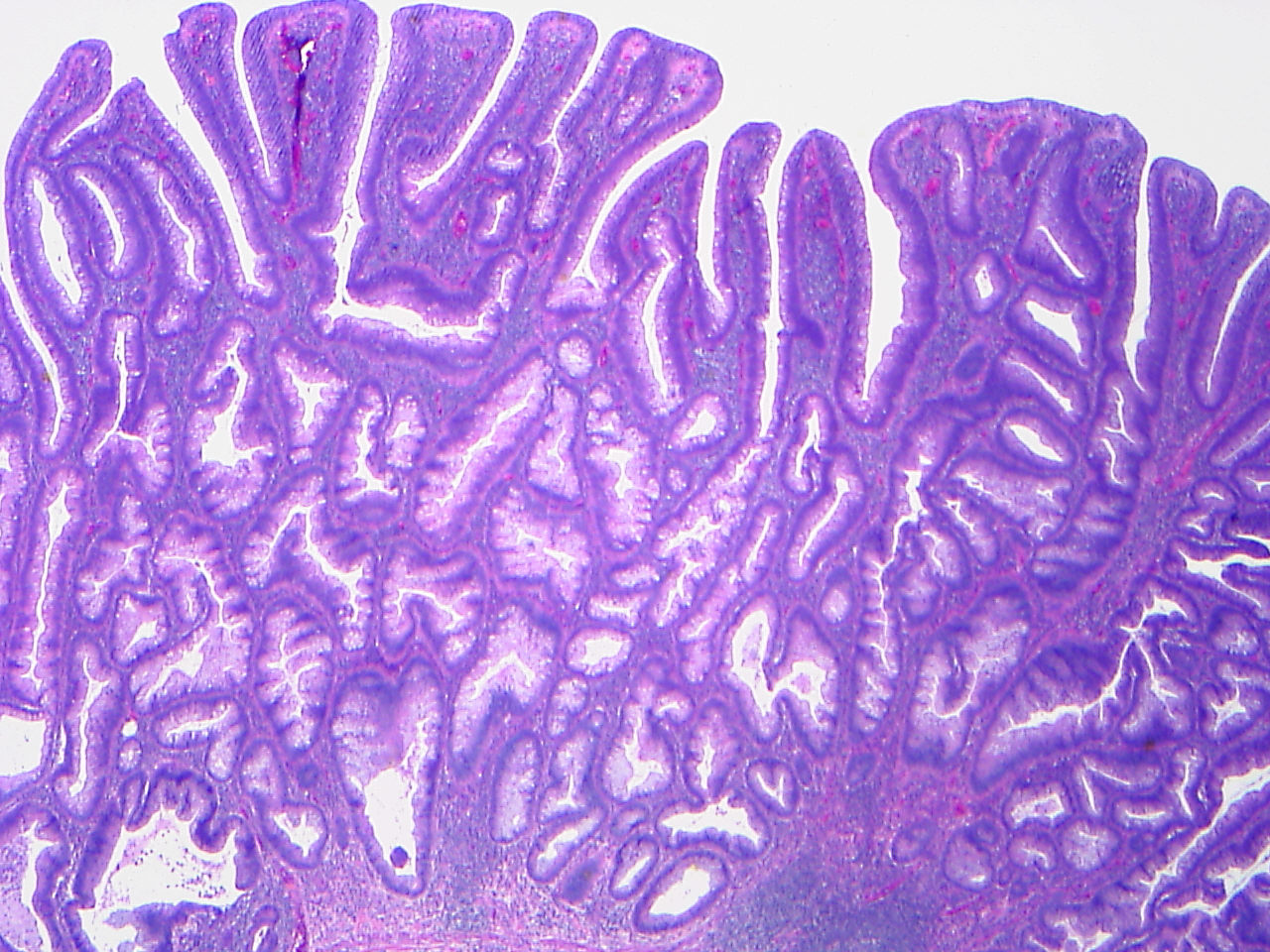
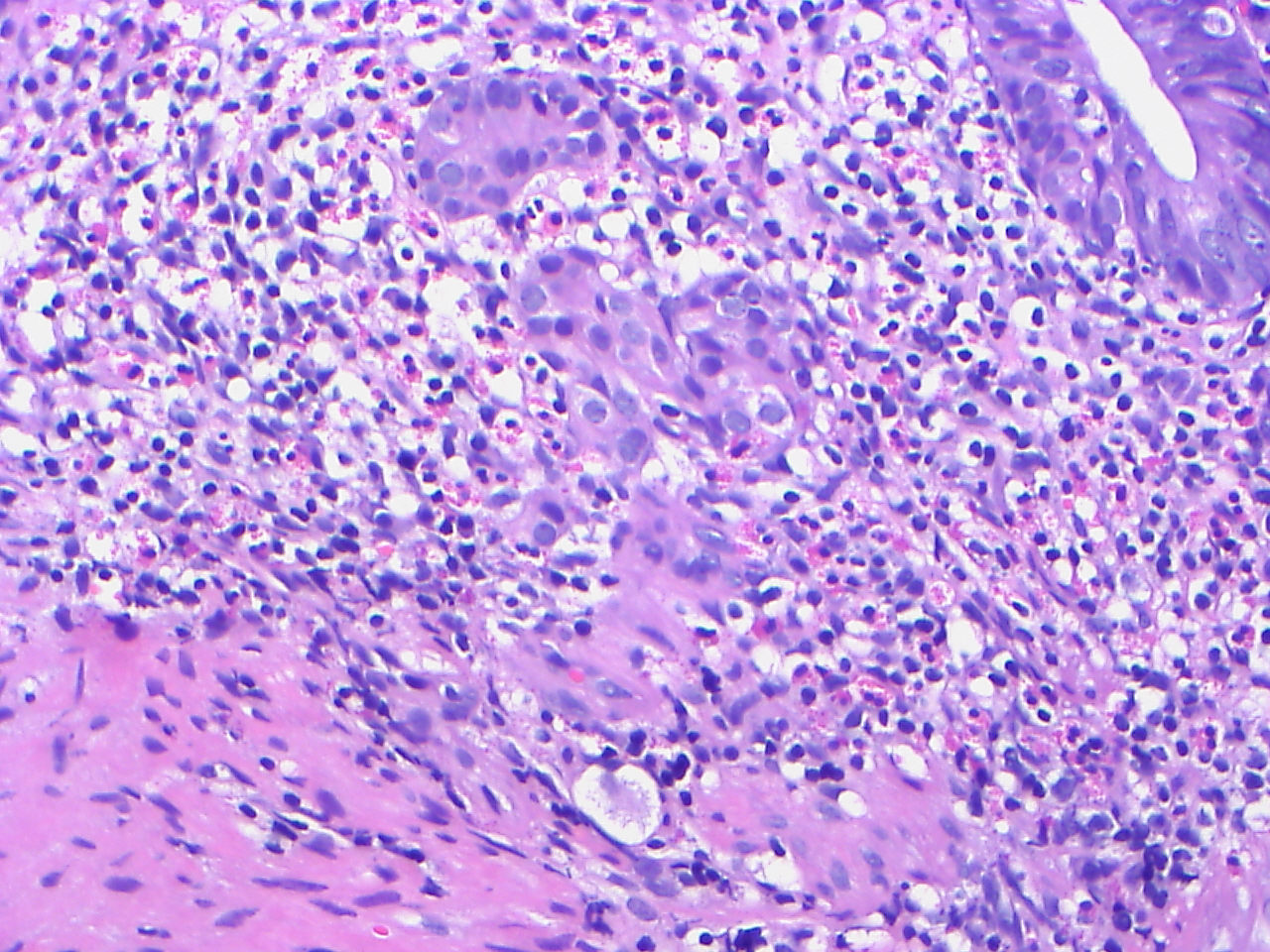
A 58 year old man had a large, rectosigmoid colonic polyp excised.
Microscopic images:

What is your diagnosis?
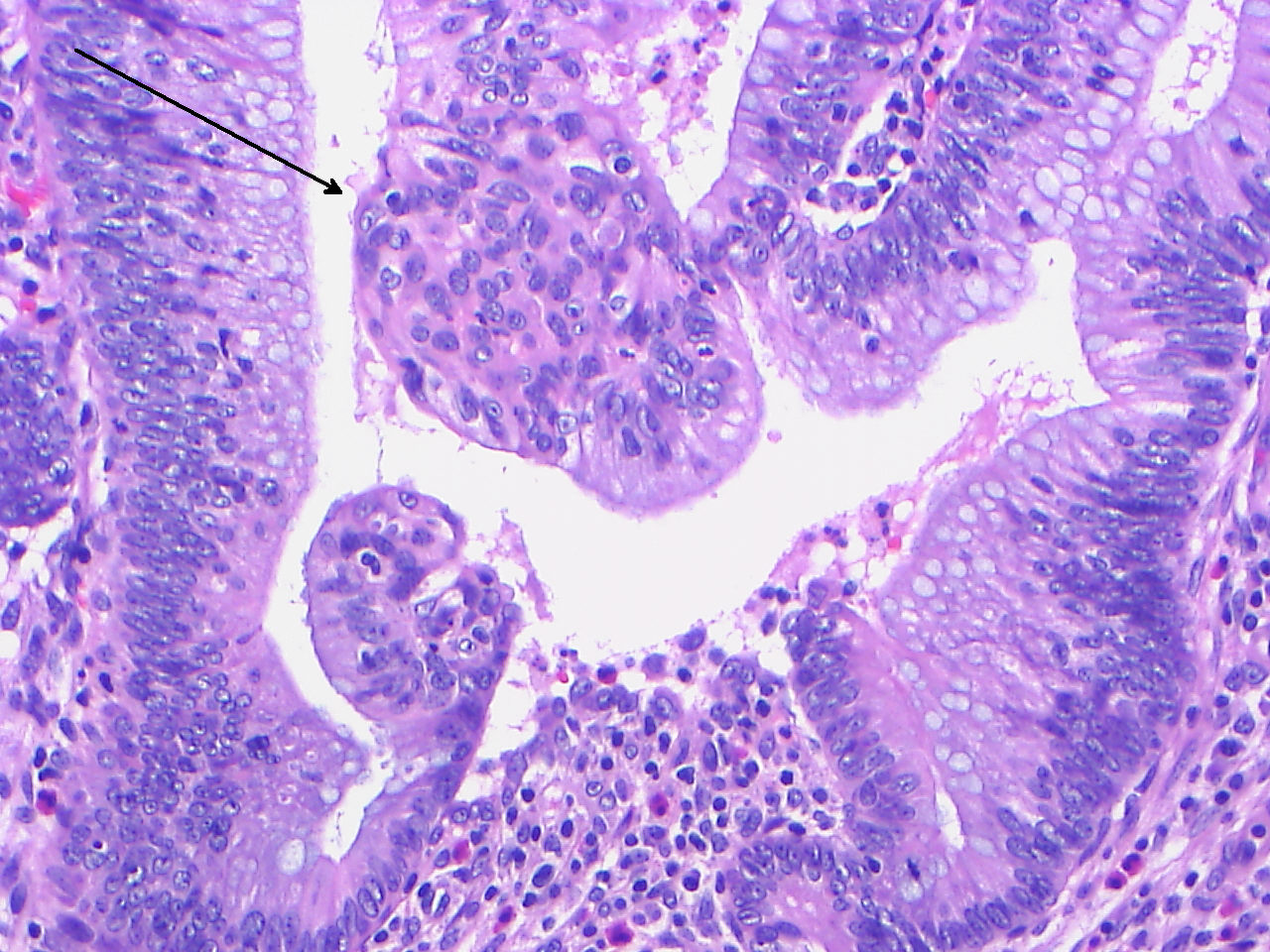
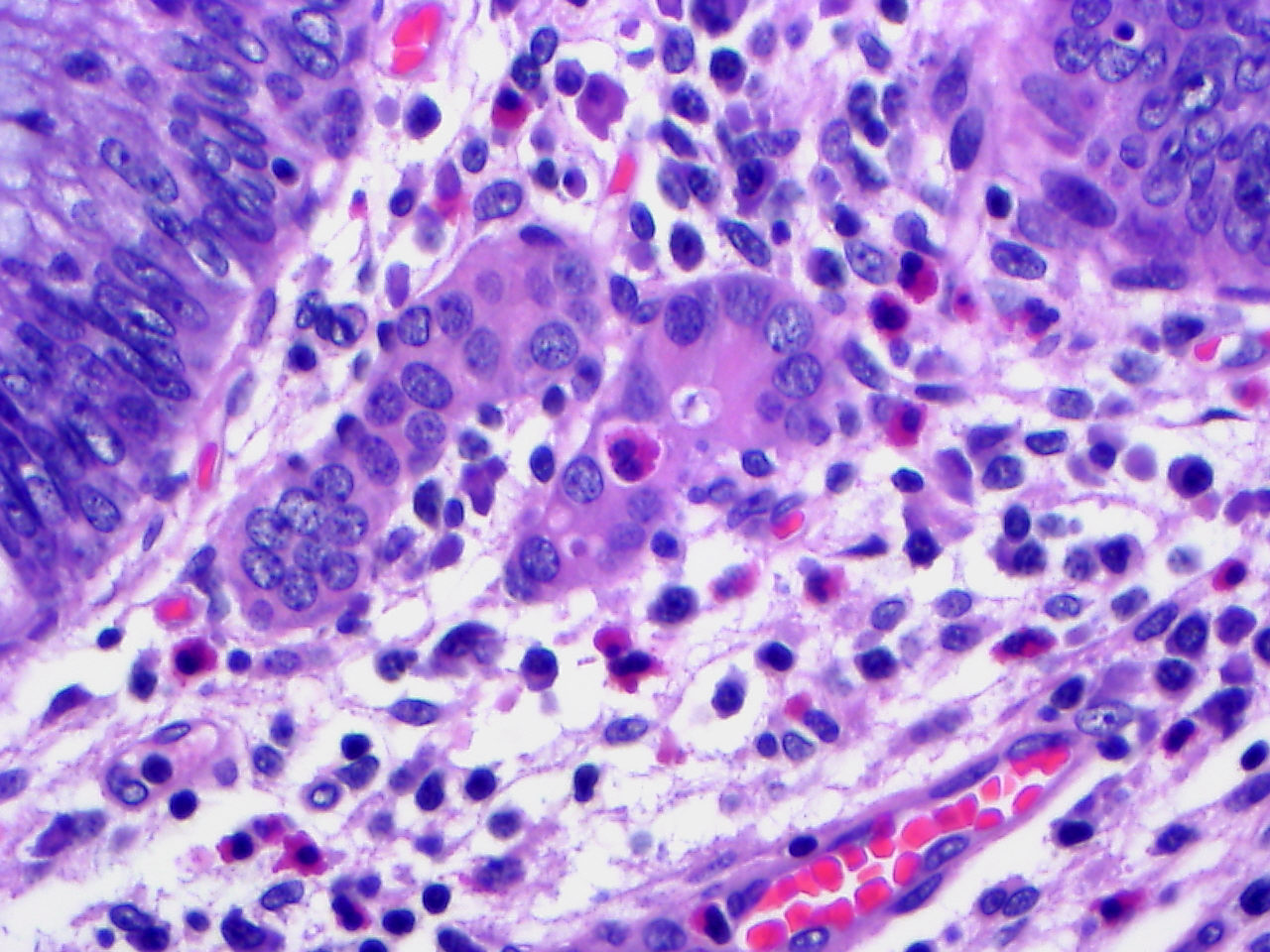
Diagnosis: Tubulovillous adenoma with microcarcinoids
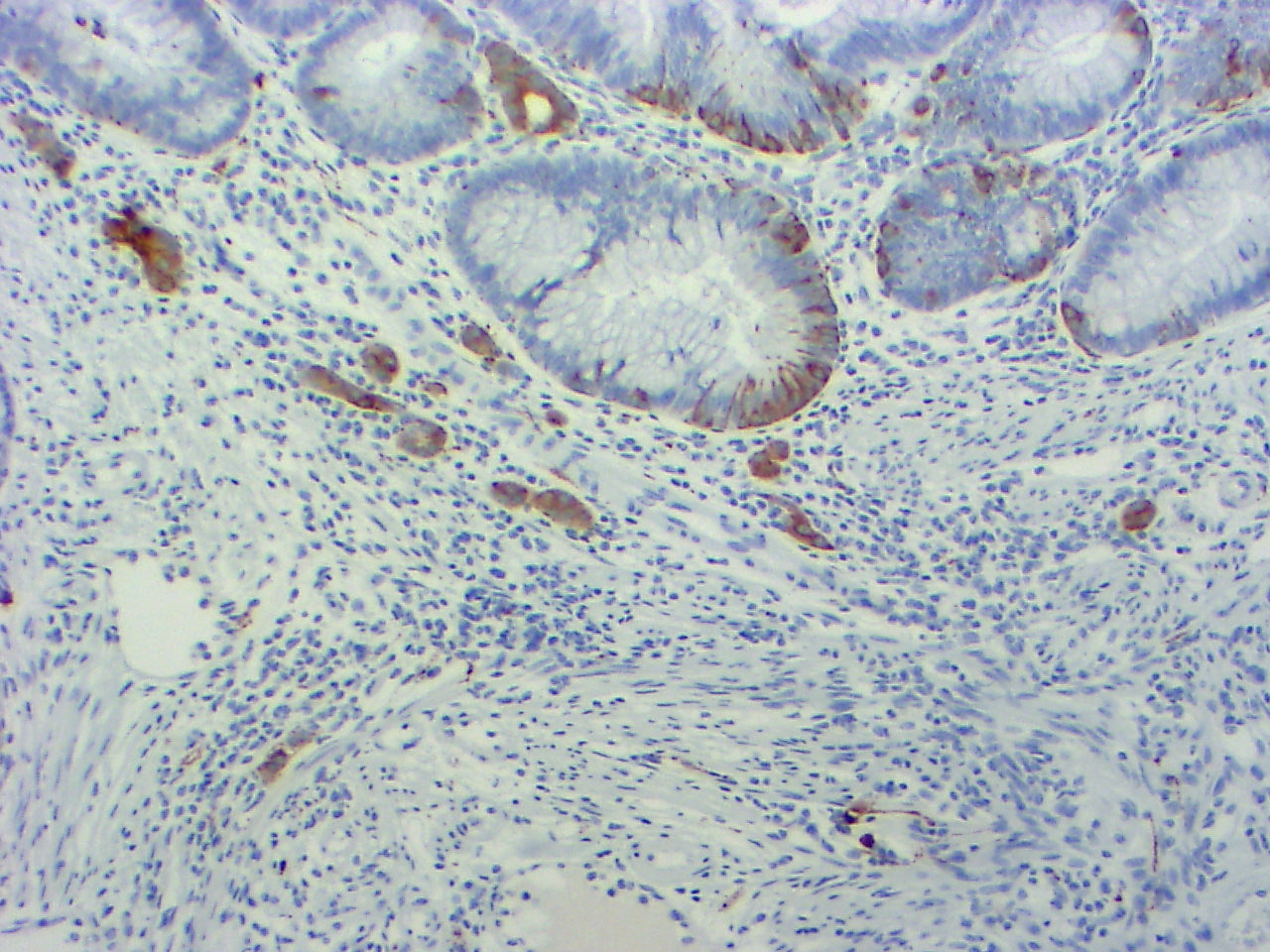
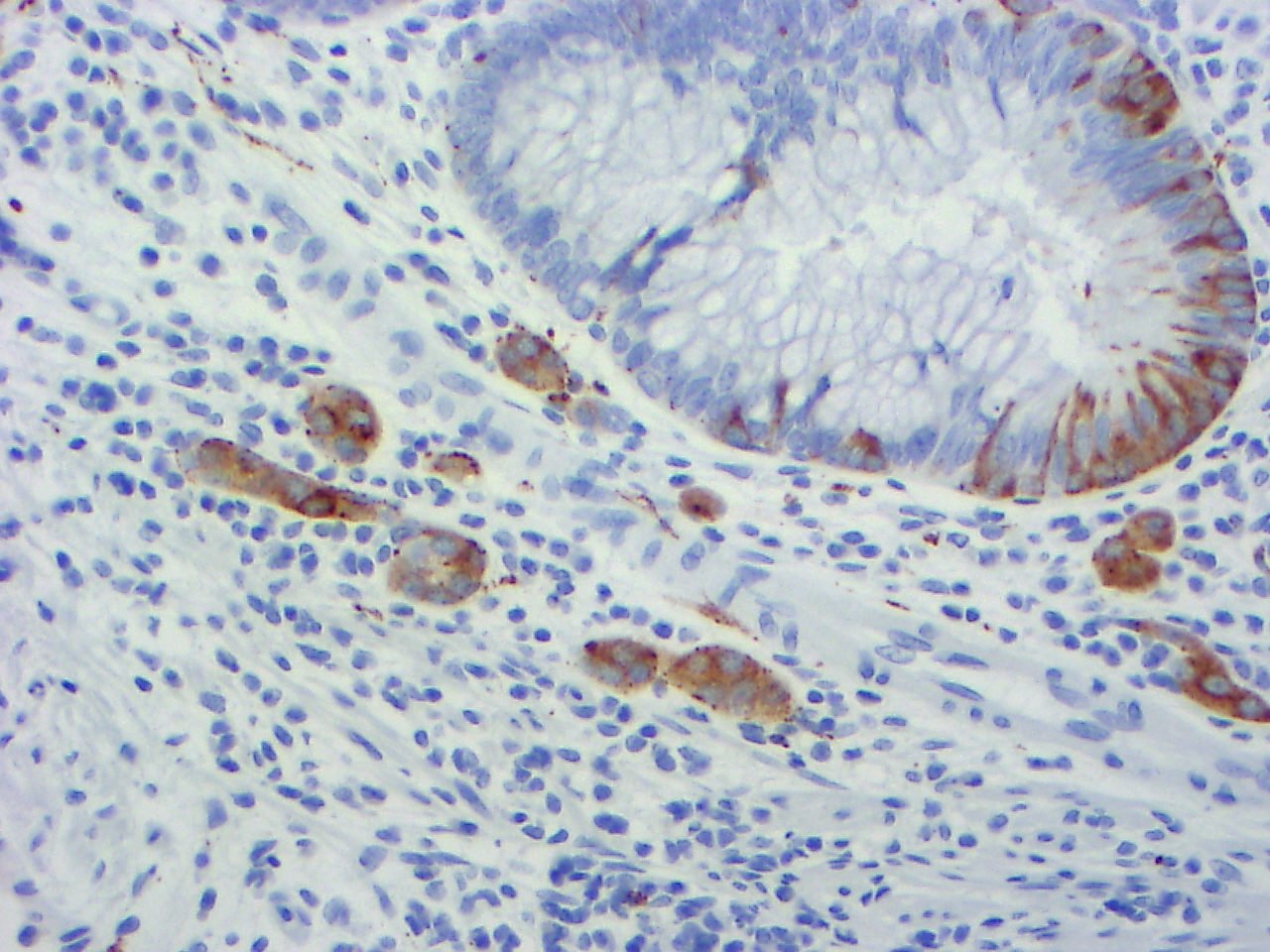
Immunostains:

Discussion:
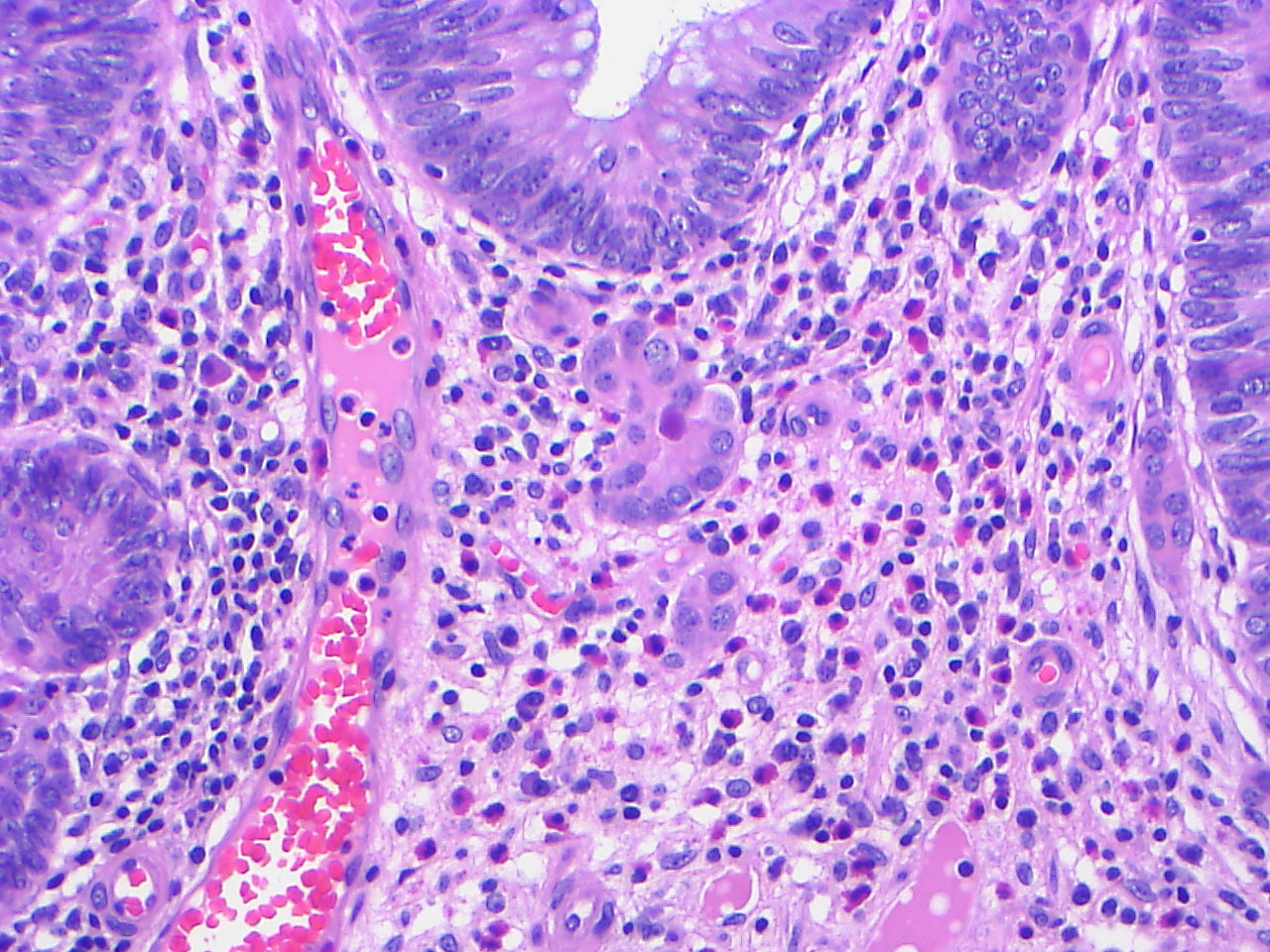
The small islands of cells were immunoreactive for synaptophysin.
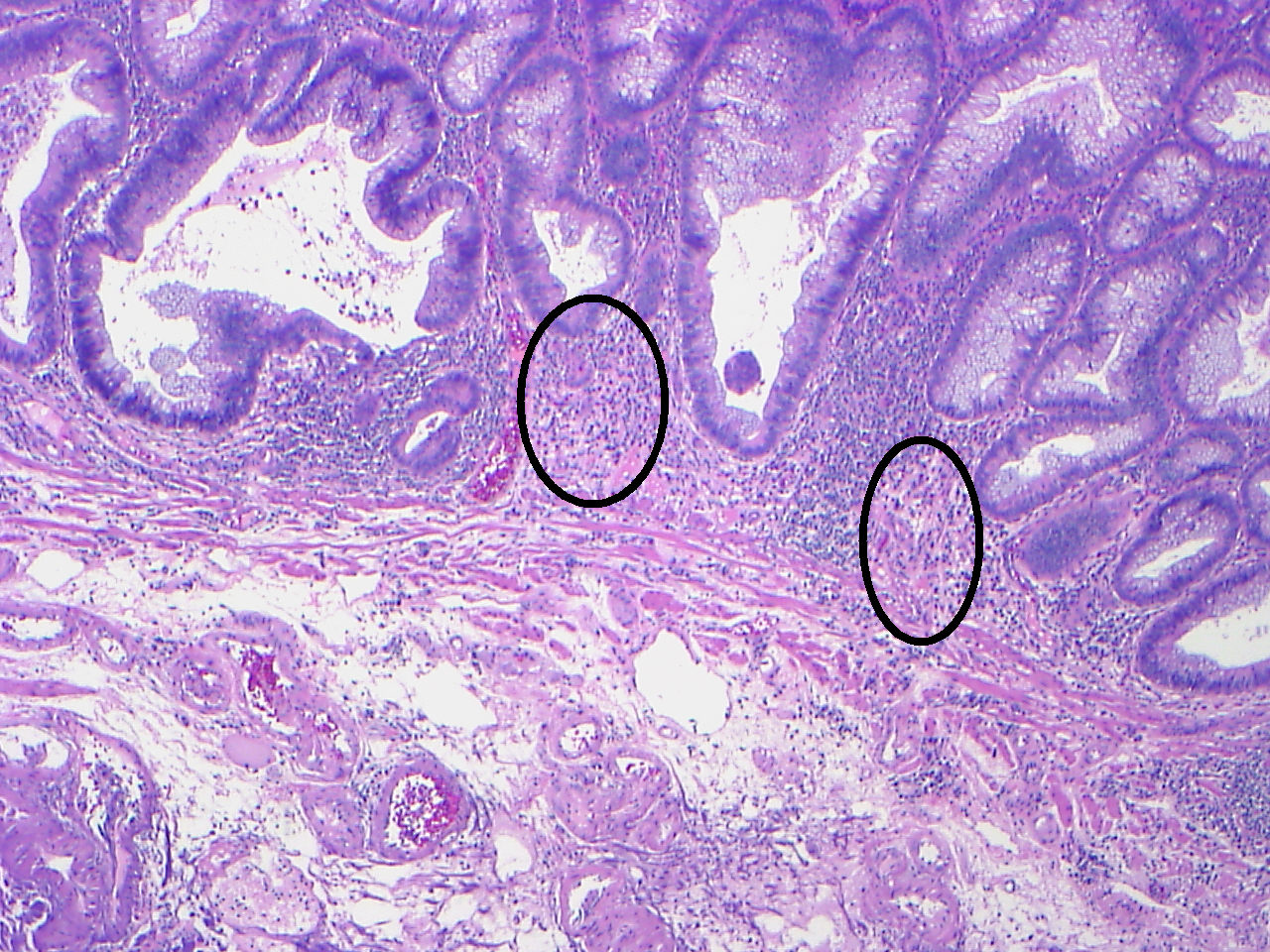
Microcarcinoids within adenomatous polyps of the colon have only recently been described (Am J Surg Pathol 2006;30:1531). They range up to 1.5 mm in size and are located between the crypts and the muscularis mucosae. They are composed of nests, cords, tubules and clusters of large epithelial cells with abundant cytoplasm, usually eosinophilic and granular and round central nuclei with stippled or dusty chromatin. There is no desmoplasia, no atypia and no mitotic activity. Tumor cells are immunoreactive for chromogranin, synaptophysin, neuron specific enolase or other neuroendocrine markers.
Microcarcinoids have previously been described in ulcerative colitis and other chronic inflammatory disorders, where they may be due to reactive hyperplasia of colonic endocrine cells (J Clin Pathol 2003;56:963).
The differential diagnosis includes mixed adenoma carcinoids. In these tumors, the carcinoid component is substantial, in contrast to the incidental microcarcinoid tumor in this case that did not alter the polyp architecture. Microcarcinoids may be interpreted as incipient adenocarcinoma, particularly if the polyp exhibits high grade dysplasia. Finally, due to their incidental nature, the microcarcinoids may not be identified.
These microcarcinoids appear to have benign behavior, with no recurrences identified to date.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Elaine Alt, Quest Diagnostics, New Jersey (USA) for contributing this case.

The Genomic Health OncotypeDX Breast Cancer Assay provides early-stage ER-positive breast cancer patients with an individualized Recurrence Score result that assesses the benefit of chemotherapy and the likelihood of 10-year distant recurrence.
The Recurrence Score is calculated using RT-PCR technology to assess the expression of 21 genes in a patients FPET core biopsy or surgical excision sample. The assay is precise, accurate, and highly reproducible over a wide dynamic range, with a success rate of >97%. The assay is validated in 13 clinical studies involving more than 4000 patients.
For more information, please visit www.oncotypedx.com.
Oncotype DX and Recurrence Score are registered trademarks of Genomic Health, Inc.
Website news:
(1) We are currently updating topics in the Bladder, Cervix-Cytology and Coagulation chapters and hope to have them completed soon.
Visit and follow our Blog to see recent updates to the website.
(1) We are currently updating topics in the Bladder, Cervix-Cytology and Coagulation chapters and hope to have them completed soon.
Visit and follow our Blog to see recent updates to the website.
Case #189
Clinical history:
A 58 year old man had a large, rectosigmoid colonic polyp excised.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Tubulovillous adenoma with microcarcinoids
Immunostains:
Discussion:
The small islands of cells were immunoreactive for synaptophysin.
Microcarcinoids within adenomatous polyps of the colon have only recently been described (Am J Surg Pathol 2006;30:1531). They range up to 1.5 mm in size and are located between the crypts and the muscularis mucosae. They are composed of nests, cords, tubules and clusters of large epithelial cells with abundant cytoplasm, usually eosinophilic and granular and round central nuclei with stippled or dusty chromatin. There is no desmoplasia, no atypia and no mitotic activity. Tumor cells are immunoreactive for chromogranin, synaptophysin, neuron specific enolase or other neuroendocrine markers.
Microcarcinoids have previously been described in ulcerative colitis and other chronic inflammatory disorders, where they may be due to reactive hyperplasia of colonic endocrine cells (J Clin Pathol 2003;56:963).
The differential diagnosis includes mixed adenoma carcinoids. In these tumors, the carcinoid component is substantial, in contrast to the incidental microcarcinoid tumor in this case that did not alter the polyp architecture. Microcarcinoids may be interpreted as incipient adenocarcinoma, particularly if the polyp exhibits high grade dysplasia. Finally, due to their incidental nature, the microcarcinoids may not be identified.
These microcarcinoids appear to have benign behavior, with no recurrences identified to date.
