
28 May 2010 - Case #180
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. David Cohen, Herzliyah Medical Center, Israel, for contributing this case.

The Genomic Health Oncotype DX Breast Cancer Assay provides early-stage ER-positive breast cancer patients with an individualized Recurrence Score result that assesses the benefit of chemotherapy and the likelihood of 10-year distant recurrence.
The Recurrence Score is calculated using RT-PCR technology to assess the expression of 21 genes in a patient's FPET core biopsy or surgical excision sample. The assay is precise, accurate, and highly reproducible over a wide dynamic range, with a success rate of >97%. The assay is validated in 13 clinical studies involving more than 4000 patients.
For more information, please visit www.oncotypedx.com.
Oncotype DX and Recurrence Score are registered trademarks of Genomic Health, Inc.
Advertisement
Case #180
Clinical history:
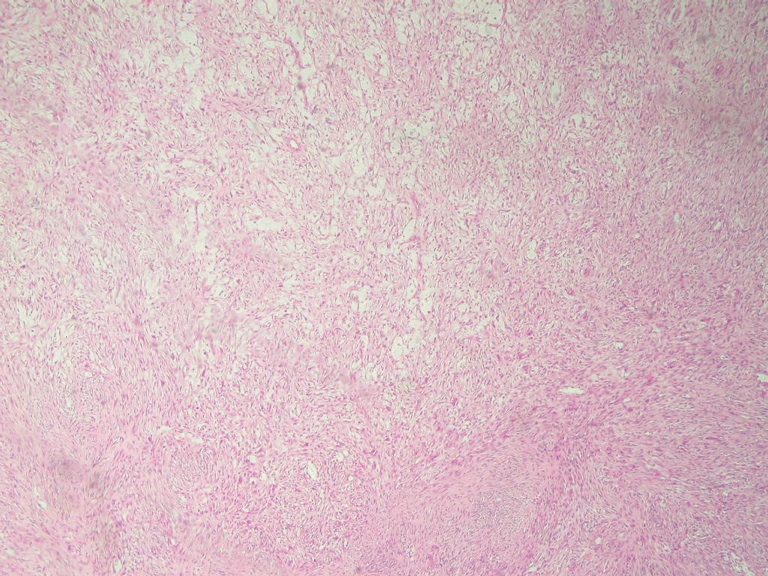
A 29 year old woman presented with a soft, friable, mildly tender subcutaneous occipital mass, which was excised. It was 3 x 2 cm, gray-tan, solid and nodular.
The tumor cells were negative for keratin, S100, MelanA, HMB45 and CD34.
Microscopic images:



What is your diagnosis?
Diagnosis: Plexiform fibrohistiocytic tumor
Immunohistochemistry images:


Discussion:
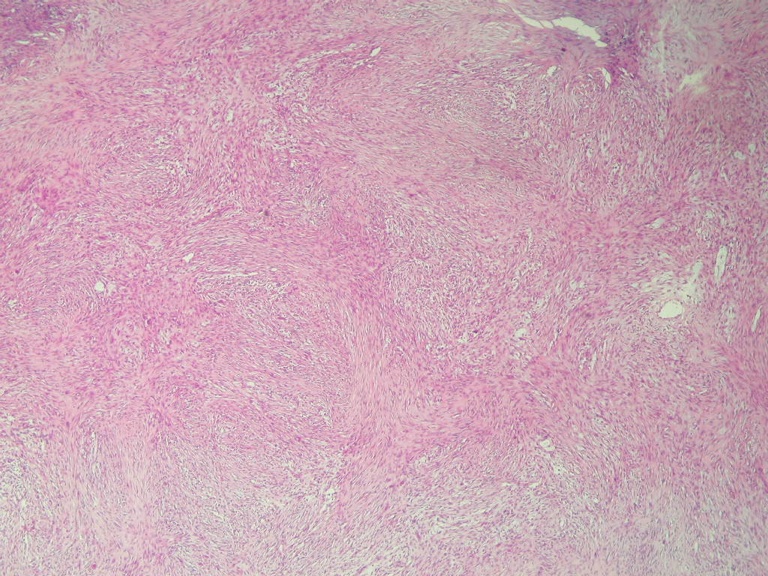
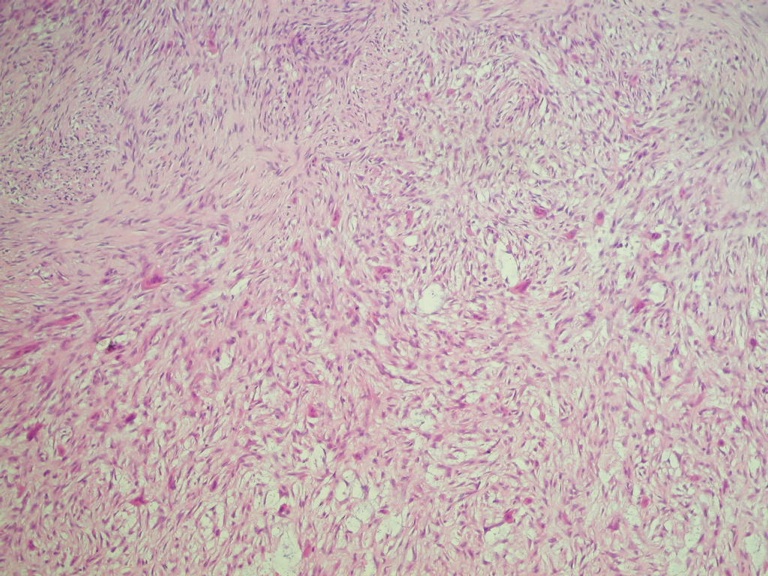
The frozen section resembled a schwannoma, with cellular palisading spindled areas mixed with hypocellular, more myxoid areas. Permanent sections show a poorly circumscribed and nonencapsulated mass. The cellular areas are composed of spindle shaped, wavy cells, often in clusters in a plexiform pattern. Interspersed between the cellular areas are plump cells with abundant eosinophilic cytoplasm but no atypia, consistent with histiocytes, including many multinucleated forms. There are rare mitotic figures but no necrosis.
Plexiform fibrohistiocytic tumor is a dermal or subcutaneous, plexiform or multinodular proliferation of fibrohistiocytic cells and osteoclast-like giant cells with a chronic inflammatory infiltrate. It was first described in 1988 (Am J Surg Pathol 1988;12:818). It usually affects children and young adults and 80% of patients are female. It presents as a small, slow growing dermal or subcutaneous mass, often affecting the upper extremity (65%) or lower extremity (27%).
Grossly, it appears as a multinodular, poorly circumscribed, firm mass up to 3 cm. Histologic examination shows a deep dermal or subcutaneous tumor with a ray like extension into skeletal muscle or adipose tissue. The overlying epidermis and dermis is usually normal. The tumor cells and stroma are as described above. Vessels are prominent and dilated. There is often hemorrhage and hemosiderin and occasional vascular invasion.
As in the present case, the spindle cells are immunoreactive for vimentin and smooth muscle actin. The giant cells and mononuclear histiocyte-like cells are positive for CD68. These cells do not stain for S100, keratin, CD34, CD45, factor VIII or desmin.
Recent publications suggest that plexiform fibrohistiocytic tumor (PFHT) may have common histogenesis with cellular neurothekeoma (Am J Surg Pathol 2009;33:905, Ultrastruct Pathol 2009;33:286). However, PFHT has distinct nodules of histiocytoid cells and osteoclast-like giant cells and is podoplanin negative, in contrast to cellular neurothekeoma (Am J Surg Pathol 2007;31:329, Am J Dermatopathol 2009;31:137).
The differential diagnosis also includes:
Treatment consists of simple excision. PFHT is considered to have low grade malignant behavior due to local recurrence and rare nodal or pulmonary metastases (Am J Surg Pathol 1999;23:662)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. David Cohen, Herzliyah Medical Center, Israel, for contributing this case.
The Genomic Health Oncotype DX Breast Cancer Assay provides early-stage ER-positive breast cancer patients with an individualized Recurrence Score result that assesses the benefit of chemotherapy and the likelihood of 10-year distant recurrence.
The Recurrence Score is calculated using RT-PCR technology to assess the expression of 21 genes in a patient's FPET core biopsy or surgical excision sample. The assay is precise, accurate, and highly reproducible over a wide dynamic range, with a success rate of >97%. The assay is validated in 13 clinical studies involving more than 4000 patients.
For more information, please visit www.oncotypedx.com.
Oncotype DX and Recurrence Score are registered trademarks of Genomic Health, Inc.
Website news:
(1) In April 2010, we had record traffic of 274,366 visits (8.5 million hits). Thanks for your support!
(2) How can you tell what fellowship openings have recently been added? We now have a link on the main fellowships page (sorted by Specialty) at the top that lists fellowships by date added, similar to the feature on the Jobs page.
Visit and follow our Blog to see recent updates to the website.
(1) In April 2010, we had record traffic of 274,366 visits (8.5 million hits). Thanks for your support!
(2) How can you tell what fellowship openings have recently been added? We now have a link on the main fellowships page (sorted by Specialty) at the top that lists fellowships by date added, similar to the feature on the Jobs page.
Visit and follow our Blog to see recent updates to the website.
Case #180
Clinical history:
A 29 year old woman presented with a soft, friable, mildly tender subcutaneous occipital mass, which was excised. It was 3 x 2 cm, gray-tan, solid and nodular.
The tumor cells were negative for keratin, S100, MelanA, HMB45 and CD34.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Plexiform fibrohistiocytic tumor
Immunohistochemistry images:
CD68
Smooth muscle actin
Discussion:
The frozen section resembled a schwannoma, with cellular palisading spindled areas mixed with hypocellular, more myxoid areas. Permanent sections show a poorly circumscribed and nonencapsulated mass. The cellular areas are composed of spindle shaped, wavy cells, often in clusters in a plexiform pattern. Interspersed between the cellular areas are plump cells with abundant eosinophilic cytoplasm but no atypia, consistent with histiocytes, including many multinucleated forms. There are rare mitotic figures but no necrosis.
Plexiform fibrohistiocytic tumor is a dermal or subcutaneous, plexiform or multinodular proliferation of fibrohistiocytic cells and osteoclast-like giant cells with a chronic inflammatory infiltrate. It was first described in 1988 (Am J Surg Pathol 1988;12:818). It usually affects children and young adults and 80% of patients are female. It presents as a small, slow growing dermal or subcutaneous mass, often affecting the upper extremity (65%) or lower extremity (27%).
Grossly, it appears as a multinodular, poorly circumscribed, firm mass up to 3 cm. Histologic examination shows a deep dermal or subcutaneous tumor with a ray like extension into skeletal muscle or adipose tissue. The overlying epidermis and dermis is usually normal. The tumor cells and stroma are as described above. Vessels are prominent and dilated. There is often hemorrhage and hemosiderin and occasional vascular invasion.
As in the present case, the spindle cells are immunoreactive for vimentin and smooth muscle actin. The giant cells and mononuclear histiocyte-like cells are positive for CD68. These cells do not stain for S100, keratin, CD34, CD45, factor VIII or desmin.
Recent publications suggest that plexiform fibrohistiocytic tumor (PFHT) may have common histogenesis with cellular neurothekeoma (Am J Surg Pathol 2009;33:905, Ultrastruct Pathol 2009;33:286). However, PFHT has distinct nodules of histiocytoid cells and osteoclast-like giant cells and is podoplanin negative, in contrast to cellular neurothekeoma (Am J Surg Pathol 2007;31:329, Am J Dermatopathol 2009;31:137).
The differential diagnosis also includes:
- Benign fibrous histiocytoma: older patients, prominent foam cells, no plexiform extensions of fibrous tissue, no nodules of histiocyte like cells, no multinucleated giant cells
- Fibromatosis: centered in muscle, diffusely infiltrative, no nodules
- Fibrous hamartoma of infancy: immature cells present, also myxoid stroma
- Giant cell tumor: infiltrative nodules of mixed giant cells and spindle cells, frequent mitotic figures
- Neurofibroma: no distinct nodules, S100+
Treatment consists of simple excision. PFHT is considered to have low grade malignant behavior due to local recurrence and rare nodal or pulmonary metastases (Am J Surg Pathol 1999;23:662)
