
6 November 2009 Case of the Week #161
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email lists, email subscribePath@gmail.com, indicating subscribe or unsubscribe to [name of email]. Our email lists are described here.


This 20-hour workshop is designed to address the activities and issues faced by the surgical pathologist.
The 24th Annual Surgical Pathology Workshop consists of short lectures and case-oriented discussions. Microscopes will be available. Participants will be asked to examine microscopic images and formulate a diagnosis and patient management strategy. The faculty pathologist will then discuss the diagnosis, differential diagnosis, patient management, and other pertinent features. Cases will be selected to represent common and/or difficult diagnostic problems.
This workshop will be held at The Canyons in Park City, Utah. Bring the family and have an incredible winter getaway! Click here for more information.
Advertisement
Website News:
(1) We make it easy for you to advertise your pathology / laboratory jobs. For Pathologist / PhD jobs, we offer a 20% discount for purchasing a package of 6 or more jobs, with prepayment. A single job posting is $700 for posting until the position is filled, up to 6 months (12 months for academic positions). For Other Laboratory jobs, we offer a discounted rate of $1000 with prepayment for posting up to 5 ads. A single ad can be for multiple positions, but is limited to 300 words. Just email the first ad to PathOutads@gmail.com, with a copy to NatPernick@gmail.com, and mention the discount (if applicable) to get started. Note that these rates may change after 12/31/09.
(2) Based on feedback at the CAP and ASCP conferences, we are planning to update our chapters more frequently with more authors and reviewers. Well keep you advised.
(3) Do you shop at Amazon.com? If so, you can help support PathologyOutlines.com by entering Amazon.com through our Home Page banner or by clicking here. Amazon tags any purchases you make as originating from our website, and pays us a referral fee. It doesnt cost you anything.
All cases are archived on our website. To view them sorted by category, diagnosis, or date, visit our Home Page and click on the Case of the Week button on the left hand side.
Thanks to Dr. S. Yasir Zaidi, Sinai-Grace Hospital, Wayne State University, Detroit, MI (USA), for contributing this case. To contribute a Case of the Week, follow the guidelines on the Case of the Week page.
Case of the Week #161
Clinical History
An 18 year old man presented with abdominal pain. CT scans showed a large abdominal mass. A core biopsy was obtained.
Micro images:
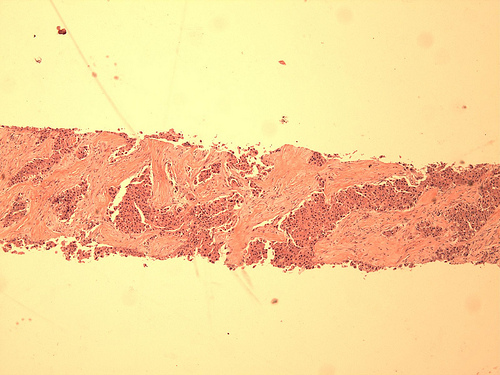
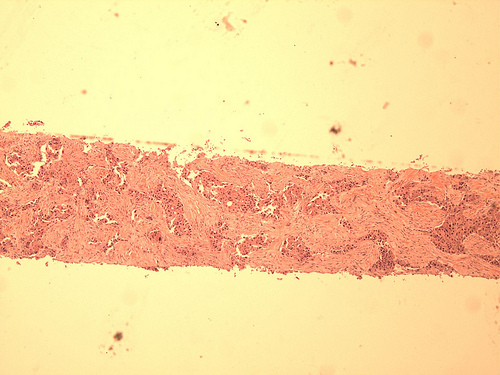
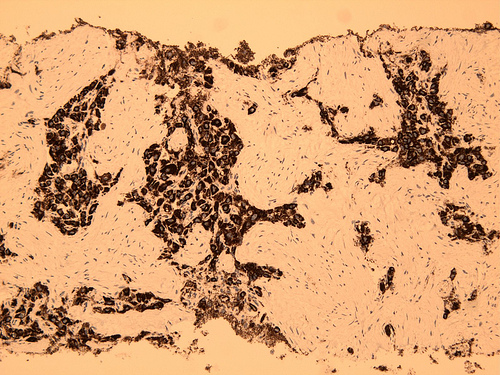
H&E, low power
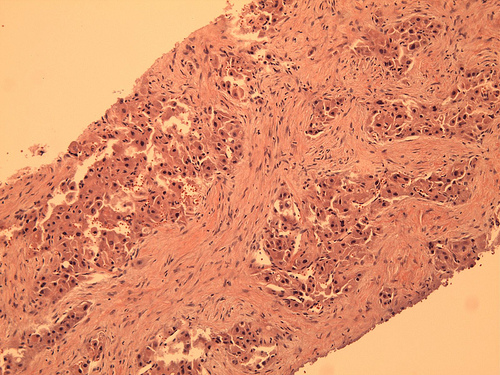
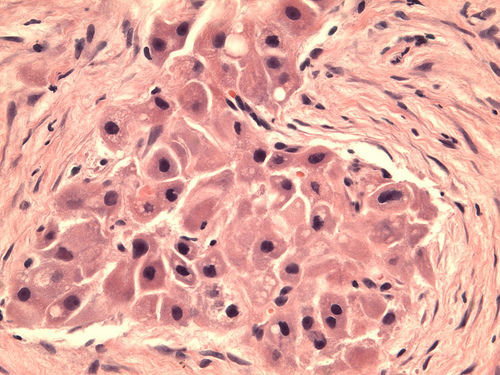
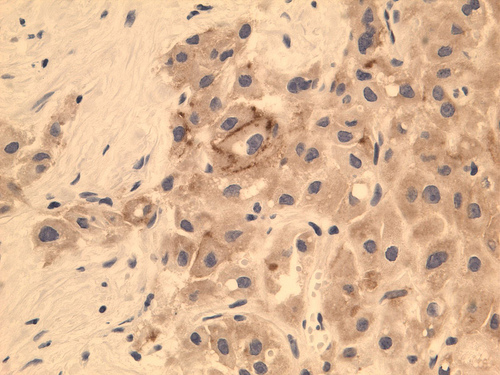
H&E, high power Pale bodies, high power
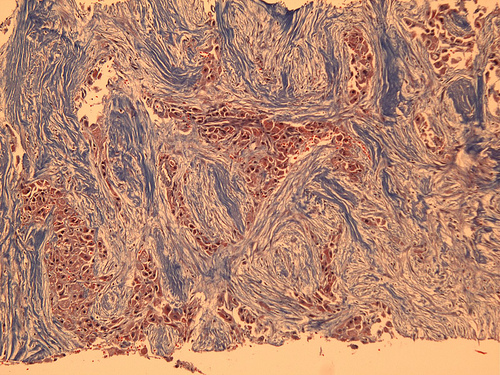
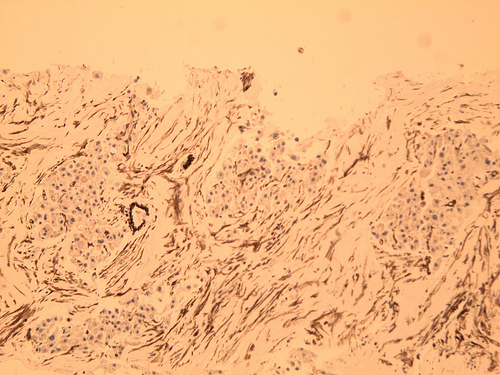
Trichrome
Immunostains:
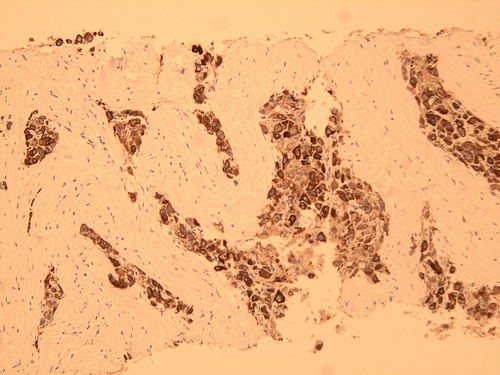
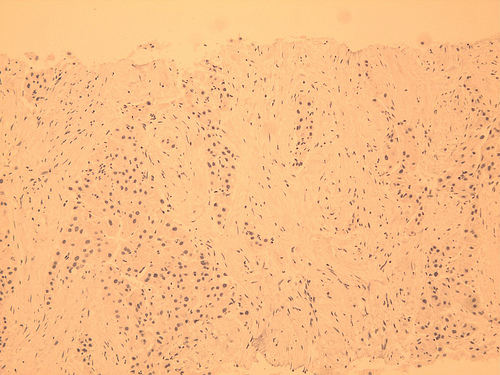
CK7 CK20 HepPar

Ki67 pCEA Vimentin
What is your diagnosis?
Diagnosis:
Hepatocellular carcinoma, fibrolamellar variant
Discussion:
Fibrolamellar hepatocellular carcinoma is uncommon, and usually affects young adults aged 20-40 years (eMedicine). It accounts for fewer than 10% of all cases of HCC, but 35% of all cases in patients younger than 50 years.
Fibrolamellar carcinoma is typically not associated with underlying liver disease, jaundice or elevated serum levels of alpha-fetoprotein. The tumors are typically large at diagnosis (mean 10-20 cm), with regional lymph node metastases in 50-70%.
Microscopically, fibrolamellar carcinomas have nests, sheets or cords of malignant cells, which are separated by lamellar bands of dense, hypocellular collagen connective tissue. The fibrotic connective tissue coalesces into the central scar. The malignant cells are usually large, well-differentiated polygonal cells containing granular cytoplasm, large nuclei, and prominent nucleoli (Adv Anat Pathol 2007;14:217). Vascular invasion and necrosis are common, and mitotic figures may be present. Fibrolamellar carcinoma is typically immunoreactive for HepPar and CK7 (Am J Clin Pathol 2005;124:512).
The differential diagnosis includes:
Focal nodular hyperplasia: usually 5 cm or less, fibrous stroma contains bile ductules and inflammatory cells, no hepatocyte atypia
Hepatocellular carcinoma, sclerosing variant: pseudoglandular pattern common, no oncocytes, smaller tumor cells
Cholangiocarcinoma
Adenosquamous carcinoma with sclerosis
Metastatic carcinoma with sclerotic stroma
Paraganglioma: may have nesting pattern at biopsy, round nuclei without atypia, vascular stroma but typically no dense fibrosis, positive for neuroendocrine markers (Am J Surg Pathol 2002;26:945)
Fibrolamellar hepatocellular carcinoma is treated with aggressive surgery (Am J Gastroenterol 2009;104:2617). The 5 year survival is 60-75%, better than classic hepatocellular carcinoma (Cancer 2006;106:1331). Early detection of relapse combined with multimodality therapy has been recommended (Eur J Surg Oncol 2009;35:617). These tumors overall show fewer chromosomal abnormalities than classic HCC, and tumors with no cytogenetic changes appear to behave less aggressively (Mod Pathol 2009;22:134)
Additional references: Mod Pathol 2005;18:1417, AJSP 1986;151:518, Ishak: Tumors of the Liver and Intrahepatic Bile Ducts (Atlas of Tumor Pathology, 3rd Series, Vol 31, 2001).
Nat Pernick, M.D., President,
and Kara Hamilton, M.S., Assistant Medical Editor
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com